










Services on Demand
Journal
Article
 text in
text in  English (pdf)
English (pdf)
 Article in xml format
Article in xml format Article references
Article references
 Send this article by e-mail
Send this article by e-mailIndicators
-
 Cited by SciELO
Cited by SciELO -
 Access statistics
Access statistics
Related links
-
 Cited by Google
Cited by Google -
 Similars in
SciELO
Similars in
SciELO -
 Similars in Google
Similars in Google
Share

 Permalink
PermalinkColombian Journal of Anestesiology
Print version ISSN 0120-3347
Rev. colomb. anestesiol. vol.42 no.4 Bogotá Oct./Dec. 2014
https://doi.org/10.1016/j.rca.2014.04.002
Case report
A rare cause of severe metabolic acidosis: Presurgical fasting*
Una causa inusual de acidosis metabólica severa: ayuno prequirúrgico
b Anesthesiologist, Hospital Universitario Mayor Méderi, Bogotá, Colombia
c Police Clinic, Bogotá, Colombia
d Undergraduate medical student, Universidad del Rosario, Bogotá, Colombia
Corresponding author at: Cra 23 n°. 118-31 apt. 302, Bogotá, Colombia. E-mail addresses: celaverde@husi.org.co, kakayy@gmail.com (C.E. Laverde-Sabogal).
*Please cite this article as: Laverde-Sabogal CE, Cárdenas ARV, Sandoval CAV. Una causa inusual de acidosis metabolica severa: ayuno prequirúrgico. Rev. Colomb. Anestesiol. 2014;42:312316.
Received 8 July 2014 - Accepted 18 July 2014
Abstract
Objectives: To discuss a clinical case and a non-systematic literature review on severe metabolic acidosis due to pre-surgical fasting, its incidence, etiology, and pathophysiology.
Materials and methods: Discussion of a case of a patient with fasting-induced severe metabolic acidosis during a laparoscopic cholecystectomy, its management and outcomes. The Ethics Committee of our institution approved the case discussion. The literature search included Pub Med, Scielo and Bireme.
Results: Fasting-induced metabolic acidosis is underdiagnosed and is related to the search for an alternate energy source in the absence of glucose and glycogen. Free fatty acids are these alternate source and generate ketone bodies that accumulate and lead to the development of acidosis. This is the first case of a non-diabetic patient at our institution. We found no other reports at the national level. There are some cases in the world literature associated with fasting from vomiting during the third trimester of pregnancy, psychiatric disorders, strict dieting, gastric band dysfunction and alcohol abuse
Conclusions: The anesthesiologist must be aware of this possibility in patients with fasting induced metabolic acidosis with normal lactate values and hemodynamic impairment that are either too young or too old, non-diabetic and with no history of alcohol abuse. The anion gap calculation tool is a simple diagnostic approach. The incidence of the condition increases during pregnancy.
Keywords: Fasting, Ketoacidosis, Metabolic acidosis, Anion gap.
Resumen
Objetivos: Presentación de un caso clínico y revisión no sistemática de la literatura sobre acidosis metabólica severa por ayuno prequirúrgico, su incidencia, etiología y fisiopatología.
Materiales y métodos: Con autorización del Comité de ética de nuestra institución, se presenta el caso de un paciente con acidosis metabólica severa inducida por ayuno durante una colecistectomía laparoscópica, su manejo y desenlace. La búsqueda bibliográfica se realizó en PubMed, Scielo y Bireme.
Resultados: La acidosis metabólica secundaria a ayuno es subdiagnosticada y está relacionada con la búsqueda de una fuente alterna de energía en ausencia de glucosa y glucógeno. Los ácidos grasos libres constituyen esta alternativa, generando cuerpos cetónicos que, al acumularse, desencadenan una cetoacidosis. Este el primer caso en nuestra institución en un paciente no diabético. No encontramos reportes a nivel nacional. Existen en la literatura médica mundial casos asociados a ayuno secundarios a vómito durante el tercer trimestre de embarazo, trastornos psiquiátricos, dietas estrictas, disfunción de banda gástrica y abuso de alcohol.
Conclusiones: El anestesiólogo debe contemplar esta posibilidad en pacientes con acidosis metabólica inducida por ayuno con valores de lactato normal y clínica de deterioro hemodinámico, que estén en los extremos de la vida, no diabéticos ni con antecedentes de abuso de alcohol. El cálculo de anión gap es una herramienta sencilla de aproximación diagnóstica. Su incidencia aumenta durante el embarazo.
Palabras clave: Ayuno, Cetoacidosis, Acidosis metabólica, Anión gap.
Introduction
The fasting-induced metabolic acidosis diagnostic of the presurgical patient is a challenge to the anesthesiologist. The causes of euglycemic ketosis are tow-fold: the first one is a drop in the amount of circulating glucose due to vomiting, extreme dieting and pregnancy. The second one is due to excessive hydrogen ions resulting from salicylate poisoning, methanol and sepsis, inter alia.1,2
Lower glucose levels and glycogen stores from poor intake results in reduced insulin secretion and increased lipolysis. These fatty acids are oxidized in the liver and develop into ketone bodies: B-hydroxybutyrate, acetoacetate and acetone. Then the tissues are transformed via mitochondrial succinyl CoA into Acetyl coA, enabling the onset of Krebs cycle and generating a alternate energy source.3 One gram of beta hydroxybutirate produces 4.69 calories as compared to glucose with 3.72 calories. The accumulation of the former causes metabolic acidosis.4-7
In clinical practice, fasting is seldom the suspect as the cause of metabolic acidosis, much less in asymptomatic, nonpregnant, non-diabetic, patients who are not alcohol users.8 Moreover, pre-surgical fasting in children and blood glucose levels below 144 mg/dl are also associated with a decrease in gastric emptying.9
Case report
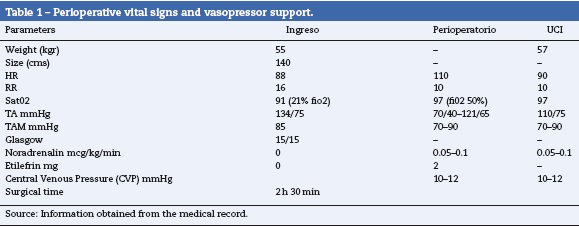
With the authorization of the Ethics Committee, this is the first case in the institution. 71-Year old male patient, mestizo ethnicity, farmer with 48 h of colicky abdominal pain in the midgut and right hypochondrium, associated with multiple vomiting and no fever. A cholecystitis-cholelithyasis is documented and the patient is scheduled for laparoscopic cholecystectomy and cholangiography. Patient Background: dyslipidemia treated with lovastatin. Oral antihypertensive therapy is initiated for uncontrolled high blood pressure. His EKG and paraclinical tests are normal. No new vomiting episodes recorded in the last 48 h. Rapid sequence intubation was performed free of complications with midazolam 2 mg, fentanyl 150 mcg, Propofol 70 mg, rocuronium 50 mg. The patient continued to develop hypotension refractory to crystalloid and vasopressors management. The perioperative and postoperative arterial and venous gasses evidence severe metabolic acidosis with no tissue hypoperfusion. The patient is transferred to the ICU with invasive ventilation support and vasopressor (Tables 1 and 2).

In the ICU, the cardiac enzymes curve was negative. The blood chemistry, coagulation and urinary output were all normal. The positive findings were: elevated anion gap value with low SID and normal lactate. The urine test showed positive ketones (three crosses). Fasting metabolic acidosis was suspected and managed with 10% dextrose for 12 h; the acid-base status was then normalized. 24 h later the ventilation support and vasopressors were removed (Tables 2 and 3).

Literature review
The anion gap, the SIDa and the lactate measurement are simple tools for the diagnostic approximation of metabolic acidosis.10
SIDa (strong ions difference) refers to the difference of the sum of all anions and strong cations; in other words, they completely dissociate in water, representing a high electrochemical power on the water dissociation and hence on the concentration of hydrogen ions. In healthy humans, the plasma SID value is 40-42 meq/Lt.11
The anion gap is the difference between the concentration of cations (positively-charged ions) y anions (negativelycharged ions) in blood, plasma or urine.1,12 The anion gap is calculated with the following formula:
- Anióngap : (Na + K)-(Cl + HCO3)orNa-(Cl + HCO3)
Usually, the cation concentration exceeds the proportion of anions in the body so that the anion gap ranges between 8 and 16 mEq/L.8 The anion gap helps to: (1) identify the source of the metabolic acidosis; (2) determine the additional basic or acid sources that contribute to worsen the mixed origin acidosis; and (3) to assess the risk assessment of critically ill patients. When the anion gap is low, acidosis is secondary to anion (albumin, hydroxybutyrate) or cations (K, Ca, Mg, and Li) disruptions, not measured routinely.1,13-15
In 1970 Feling and Linch described a higher incidence during the third trimester of pregnancy. During this last trimester, the placenta increases the production of glucagon, cortisol, and lactogen resulting in increased insulin peripheral resistance as well as an increased production of ketone bodies as a biochemical energy source. Vomiting is a stressor that increases the endogenous non-placenta production of glucagon and cortisol, leading to more acute acidosis.4,10 This fact has been described in eight case reports with the following characteristics: onset of vomiting in less than 24 h, two cases of infection, one case of gestational diabetes and moderate to severe metabolic acidosis. All these cases were managed with 10% dextrose infusion, control of the infection site, fetal monitoring, C-section in some cases, and strict gas monitoring in the ICU.10,14-20
The findings in fasting non-pregnant voluntary adults showed a 10% glucose-dependent caloric input, 32% depended on ketone bodies and 50% on free fatty acids, with a peak production of ketones by the third day of fasting. During pregnancy, metabolic acidosis occurs earlier due to a higher caloric intake and subsequent ketone production, associated with the physiological insulin resistance as mentioned above.15
Ketoacidosis in diabetic patients has a de novo occurrence due to inadequate treatment (euglicemia) or is associated with infection. It is also associated with alcohol abuse, strict dieting (fruitarianism, Atkins diet), extreme exertion or malnutrition with extremely poor intake.21,22 Also patients with dysfunctional gastric banding leading to chronic vomiting that some times requires surgical correction.23,24
David & cols describe the case of a young non-pregnant patient who presents with three-day vomiting resulting in severe ketoacidosis that was managed and resolved with 10% dextrose for 12 h.24,25 Toth & Greenbaum also report a case of a one-year old child, post-resuscitation with cerebral edema and suspicious hypoxic brain injury. The bay received intravenous fluids with no dextrose or nutritional support for five days because of an apparent deleterious cerebral effect of hyperglycemia. Severe metabolic acidosis was diagnosed, with elevated anion gap and positive ketones. The patient was treated with dextrose.26 We could not find any specific case of pre-surgical fasting.
Discussion
We present a case of an elderly patient with severe metabolic acidosis after fasting for over 8 h, with no glucose or nutritional support. The diagnosis of fasting metabolic acidosis was made upon screening for other conditions, assisted by an elevated anion gap with ketones in the urine and rapid therapeutic response. This is a rare case considering the ripe age of the patient, with no history of diabetes or alcohol abuse. Polypnea was the only factor contributing to the severe ketosis.
Our findings indicate that the time to develop fasting ketosis is 3 days in healthy volunteers, but less that 24 h in children and elderly people, because of the depletion of glycogen stores, which is consistent with our patient’s fasting time. The patient presents with a moderate severity and a bicarbonate level between 17 through 22-mEq/L (17-22-mmol/L), explained by decreased catecholamine and cortisol synthesis to prevent the excessive production of ketones. In our patient, the severity of the acidosis is explained by the multiplicity of factors.
The metabolic cost of fasting is underestimated, particularly in the asymptomatic patient, the compensatory response-Ketosis, as well as its physiological impact encourages to consider a change in attitude2,3
Conclusions
The anesthesiologist should consider this possibility in patients with fasting-induced metabolic acidosis, with normal lactate values and hemodynamic involvement and who are either too young or too old, non-diabetic and no history of alcohol abuse. The anion gap calculation is a simple diagnostic approach tool. Its incidence rises during pregnancy.
Funding
No.
Conflicts of interest
No.
References
1. Forni LG, McKinnon W, Hilton PJ. Unmeasured anions in metabolic acidosis: Unravelling the mystery. Crit Care. 2006;10:220. [ Links ]
2. Carrillo R. Acidosis metabólica hiperclorémica hiperclorémica en el perioperatorio. Rev Mex Anestesiol. 2006;29:5. [ Links ]
3. Mendoza A. Importancia de la grasa para la supervivencia en el ayuno, vista a través de una enzimopatia. Rev Mex Anestesiol. 2010;29:9. [ Links ]
4. Cahill GF. Starvation in man. Clin Endocrinol Metab. 1976;5:397-415. [ Links ]
5. Lipnick MS, Braun AB, Cheung JT, Gibbons FK, Christopher KB. The difference between critical care initiation anion gap and prehospital admission anion gap is predictive of mortality in critical illness. Crit Care Med. 2013;41:49-59. [ Links ]
6. Davids MR, Segal AS, Brunengraber H, Halperin ML. An unusual cause for ketoacidosis. QJM. 2004;97:365-76. [ Links ]
7. Cahill GF. Fuel metabolism in starvation. Annu Rev Nutr. 2006;26:1-22. [ Links ]
8. Domínguez-Cherit G, Namendys-Silva SA. Changes in the anion gap: A novel marker of outcome in critically ill patients. Back to the basis. Crit Care Med. 2013;41:336-7. [ Links ]
9. Reyes R, Alvarez L. Ayuno preoperatorio en niñnos sanos de 2, 4 y 6 h. Rev Colomb Anestesiol. 2009;37:63-70. [ Links ]
10. Frise CJ, Mackillop L, Joash K, Williamson C. Starvation ketoacidosis in pregnancy. Eur J Obstet Gynecol Reprod Biol. 2013;167:1-7. [ Links ]
11. Kellum J. Determinants of plasma acid-base balance. Critical Care Clinics. 2005;21:329-46. [ Links ]
12. Forni LG, McKinnon W, Lord GA, Treacher DF, Peron JM, Hilton PJ. Circulating anions usually associated with the Krebs cycle in patients with metabolic acidosis. Crit Care. 2005;9:R591-5. [ Links ]
13. Reilly R, Anderson RJ. Interpreting the anion gap. Crit Care Med. 1998;26:1771-2. [ Links ]
14. Espes D, Engström J, Reinius H, Carlsson PO. Severe diabetic ketoacidosis in combination with starvation and anorexia nervosa at onset of type 1 diabetes: A case report. Ups J Med Sci. 2013;118:130-3. [ Links ]
15. Patel A, Felstead D, Doraiswami M, Stocks GM, Waheed U. Acute starvation in pregnancy: A cause of severe metabolic acidosis. Int J Obstet Anesth. 2011;20:253-6. [ Links ]
16. Joseph F, Anderson L, Goenka N, Vora J. Starvation-induced true diabetic euglycemic ketoacidosis in severe depression. J Gen Intern Med. 2009;24:129-31. [ Links ]
17. Burbos N, Shiner AM, Morris E. Severe metabolic acidosis as a consequence of acute starvation in pregnancy. Arch Gynecol Obstet. 2009;279:399-400. [ Links ]
18. Keay S, Fox R. Maternal ketoacidosis complicating acute starvation in pregnancy. J Obstet Gynaecol. 2000;20:539. [ Links ]
19. Mahoney CA. Extreme gestational starvation ketoacidosis: Case report and review of pathophysiology. Am J Kidney Dis. 1992;20:276-80. [ Links ]
20. Scholte JB, Boer WE. A case of nondiabetic ketoacidosis in third term twin pregnancy. J Clin Endocrinol Metab. 2012;97:3021-4. [ Links ]
21. Causso C, Arrieta F, Hernández J, Botella-Carretero JI, Muro M, Puerta C, et al. Severe ketoacidosis secondary to starvation in a frutarian patient. Nutr Hosp. 2010;25:1049-52. [ Links ]
22. Miaskiewicz S, Levey GS, Owen O. Severe metabolic ketoacidosis induced by starvation and exercise. Am J Med Sci. 1989;297:178-80. [ Links ]
23. Lulsegged A, Saeed E, Langford E, Duffield C, El-Hasani S, Pareek N. Starvation ketoacidosis in a patient with gastric banding. Clin Med. 2011;11:473-5. [ Links ]
24. Bruegger D, Rehm M, da Silva l. Severe metabolic acidosis resulting from a dislocated gastric band. Obes Surg. 2004;14:555-8. [ Links ]
25. Owen D, Little S, Leach R, Wyncoll D. A patient with an unusual aetiology of a severe ketoacidosis. Intensive Care Med. 2008;34:971-2. [ Links ]
26. Toth HL, Greenbaum LA. Severe acidosis caused by starvation and stress. Am J Kidney Dis. 2003;42:E16-9. [ Links ]
