










Services on Demand
Journal
Article
 text in
text in  English (pdf)
English (pdf)
 Article in xml format
Article in xml format Article references
Article references
 Send this article by e-mail
Send this article by e-mailIndicators
-
 Cited by SciELO
Cited by SciELO -
 Access statistics
Access statistics
Related links
-
 Cited by Google
Cited by Google -
 Similars in
SciELO
Similars in
SciELO -
 Similars in Google
Similars in Google
Share

 Permalink
PermalinkColombian Journal of Anestesiology
Print version ISSN 0120-3347
Rev. colomb. anestesiol. vol.43 no.3 Bogotá July/Sept. 2015
Scientific and Technological Research
Lactated Ringer's vs. normal saline solution for renal transplantation: Systematic review and meta-analysis*
Lactato de Ringer vs. Solución salina normal para trasplante renal. Revisión sistemática y meta-análisis
Jorge Alejandro Trujillo-Zeaa, Natalia Aristizábal-Henaob, Nelson Fonseca-Ruizc,**
a Anesthesiologist, Universidad Pontificia Bolivariana, Medellín, Colombia
b Internist, Universidad Pontificia Bolivariana, Medellín, Colombia
c Anesthesiologist, Intensivist, Epidemiologist, Universidad Pontificia Bolivariana, Medellín, Colombia
* Please cite this article as: Trujillo-Zea JA, Aristizabal-Henao N, Fonseca-Ruiz N. Lactato de Ringer vs. Solución salina normal para trasplante renal. Revisión sistemática y metaanálisis. Rev Colomb Anestesiol. 2015;43:194-203.
** Corresponding author at: Calle 36 AA sur No. 25B-99 1129, Medellín, Colombia. E-mail address: nfonseca@une.net.co (N. Fonseca-Ruiz).
Article info
Article history: Received 19 March 2014 Accepted 8 March 2015 Available online 20 May 2015
Abstract
Background: The administration of potassium solutions may result in hyperpotassemia during surgery; normal saline solution (NSS) traditionally used in renal transplant may cause hyperchloremic acidosis.
Objective: To compare the safety of Lactated Ringer's (LR) against NSS in renal transplantation.
Search strategy: A systematic review was completed on Central Cochrane Registry - controlled trials, Medline, Lilacs, EBSCO and Embase, accessing review articles and contacting expert clinicians. There was no language restriction.
Selection criteria: Randomized controlled trials on adult patients undergoing renal transplantation.
Data collection and analysis: Independent trial selection, quality assessment and data extraction were performed. The mean differentials were estimated with a 95% confidence interval (95% CI). Heterogeneity was evaluated with statistic I-square(I2) and the fixed and random effect models were used.
Results: Four trials with a total of 237 patients were included. At the end of surgery, the potassium differential was non-significant (means difference (MD: -0.26 mEq/L; CI 95%: -0.58 to 0.05 p = 0.10; I2 = 75%); the pH was lower in the NSS group (MD: 0.06; CI 95%: 0.05-0.08; p < 0.001; I2 = 17%). No difference in Creatinine was identified on the third postoperative day (MD: -0.05; CI 95%: -0.59 to 0.48; p = 0.85; I2 = 0%).
Condusions: The use of RL vs. NSS during the renal transplantation perioperative period results in lower potassium and chloride levels and a higher pH, with no significant Creatinine changes.
Keywords: Kidney transplantation, Acidosis, Hyperkalemia, Sodium chloride, Perioperative Period.
Resumen
Antecedentes: La administración de soluciones con potasio puede causar hiperpotasemia durante cirugía, la Solución Salina Normal (SSN), usada tradicionalmente en trasplante renal, puede generar acidosis hiperclorémica.
Objetivo: Comparar la seguridad del Lactato de Ringer (LR) con SSN en trasplante renal. Estrategia de búsqueda: Se realizó una revisión sistemática en el Registro Cochrane Central de ensayos controlados, Medline, Lilacs, EBSCO y Embase, en artículos de revisión y contactando clínicos expertos. No hubo restricción de idioma.
Criterios de selección: Se incluyeron ensayos controlados aleatorios en pacientes adultos sometidos a trasplante renal.
Recogida y análisis de datos: De forma independiente se realizó selección de estudios, evaluación de la calidad y extracción de datos. Se calculó diferencia de medias con su intervalo de confianza del 95% (IC 95%). Se evaluó la heterogeneidad con el estadístico I-cuadrado (I2). Se usaron los modelos de efectos fijos y aleatorios.
Resultados: Se incluyeron cuatro estudios con un total de 237 pacientes. Al final de cirugía la diferencia de potasio no fue significativa (Diferencia de Medias (DM: -0,26 mEq/L; IC 95%: -0,58 a 0,05 p = 0,10; I2 = 75%), el pH fue menor en el grupo de SSN (DM: 0,06; IC 95%: 0,05 a 0,08; p < 0,001; 12:17%). No hubo diferencia en la creatinina al tercer día posoperatorio (DM: -0,05; IC 95%: -0,59 a 0,48; p = 0,85; I2 = 0%).
Conclusiones: El uso de LR comparado con SSN en el perioperatorio de trasplante renal genera menores niveles de potasio y cloro y mayor pH, sin cambios significativos en la creatinina.
Palabras clave: Transplante de riñon, Acidosis, Hiperpotasemia, Cloruro de sodio, Periodo perioperatorio.
Introduction
Intraoperative fluid management during renal transplantation has traditionally been done with normal saline solution (NSS) because the administration of potassium solutions such as Lactated Ringer's (LR) in large volumes to surgical patients may lead to hyperpotassemia1. Several papers have been published on the topic, showing that the administration of large volumes of NSS, as is usually the case in patients undergoing renal transplantation (RT), is associated with hyperchloremic metabolic acidosis1-4.
According to Steward's theory, fluids usually administered during surgery may alter the acid-base balance and predispose to metabolic acidosis due to a rise in chloride levels5,6. Such acidosis may lead to hyperpotassemia due to the extracellular shifts of potassium ions1-3,7. Hyperchloremia may at the same time result in vasoconstriction of the afferent arteriole and renal graft injury2,3. Other acidosis-related complications may be changes in mental status and abdominal discomfort due to disruptions of the splanchnic vasculature7 and it has even been associated with higher mortality in surgical patients8.
Kidney transplant is the most usual transplantation in our country and around the world9; RT results have improved with the advancement of surgical, immune suppressor, and anesthesia techniques. The presence of hyperpotassemia associated with hyperchrolemic metabolic acidosis may contribute to the graft dysfunction, and hence should be prevented in these patients10.
Several trials have been published comparing the use of LR with NSS but they include few patients2,3,11-14. We did a metaanalysis to assess the effects of LR vs. NSS on the incidence of hyperchloremic metabolic acidosis, hyperpotassemia, volume of fluids infused and kidney graft dysfunction in patients undergoing renal transplant.
Methodology
This systematic review followed the methodology recommended by the Cochrane Collaboration14. This protocol has not been published and was not registered.
Eligibility criteria
The search included randomized, clinical controlled trials with no restrictions as to language, date or status of publication, comparing the use of LR against NSS as fluid therapy in renal transplantation patients, over 18 years old. The outcomes evaluated were the level of serum potassium, bicarbonate, chloride, Creatinine and the postoperative pH. The deadline of publication established was July 8, 2013.
Search strategies
Independently, the three authors did an electronic database search, contacting expert clinicians and searching review articles. No language and date of publication restrictions were applied.
The databases accessed were the Central Cochrane Registry of Controlled Trials, Medline (1966-2013), Lilacs (1982-2013), EBSCO and Embase (1980-2013).
The search terms used were "renal transplant", "acidosis", "acidemia", "hyperpotassemia", "graft dysfunction", "Lactate Ringer's" and "saline solution".
Trial selection and evaluation
Two of the authors independently reviewed all the titles and abstracts identified in the bibliography searched and excluded the irrelevant trials. The remaining assays were evaluated in full text and disagreements were settled with the participation of the third author.
All three researchers - in accordance with the Cochrane Collaboration guide - independently assessed the validity of the trials selected15. The random sequence generation, the sequence hiding, blinding, information gathering, losses to follow-up during the trial, inclusion of incomplete data, selective outcome reporting, and other biases were all evaluated. Based on this methodology, the risk of biases was classified into high, uncertain, and low.
Data collection
Based on the recommendations from Cochrane Consumers and Communication Review data extraction template14 the analysis of the information extracted was done using an information extraction table. The information that was required but not available after reading the articles was requested to the authors directly. The article with the largest sample was written in Farsi13 and only the abstract was available in English. There were failed attempts to contact the authors in order to obtain the complete data. An investigator extracted the information from the trials, following the table closely. To ensure the accuracy of the data, a second investigator then reviewed the information collected.
Results analyzed
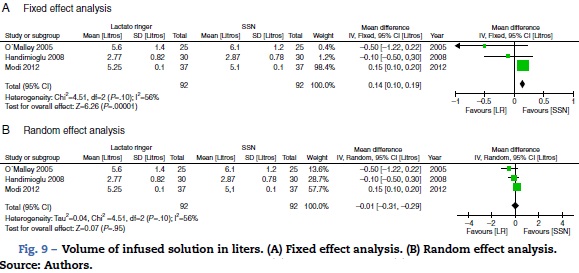
The results analyzed included the average serum potassium in mEq/L during the postoperative period, serum Creatinine in mg/dL three days after surgery, pH immediately after surgery, the volume of infused solution in liters and bicarbonate and chloride in the arterial blood expressed in mEq/L following surgery.
Statistical analysis
This meta-analysis estimated the mean difference with its respective 95% confidence interval (95% CI) for the variables considered, using Review Manager software, version 5.1. An analysis using the fixed or random effects model was completed, based on the existence of statistical heterogeneity. The statistical heterogeneity was evaluated using the Q Cochrane test and the I2 statistic. When I2 was less than 40%, we used the fixed effects model and if I2 was above 40%, the random effects model was used. The sensitivity analysis was completed based on the methodological quality of the trials, removing some trials and re-analyzing the data. Similarly, a sub-group analysis was done, based on the patients' characteristics and the mode of intervention used.
Results
Trial selection process
The initial search identified 187 articles, of which 182 were ruled out due to failure to meet the eligibility criteria (Fig. 1).

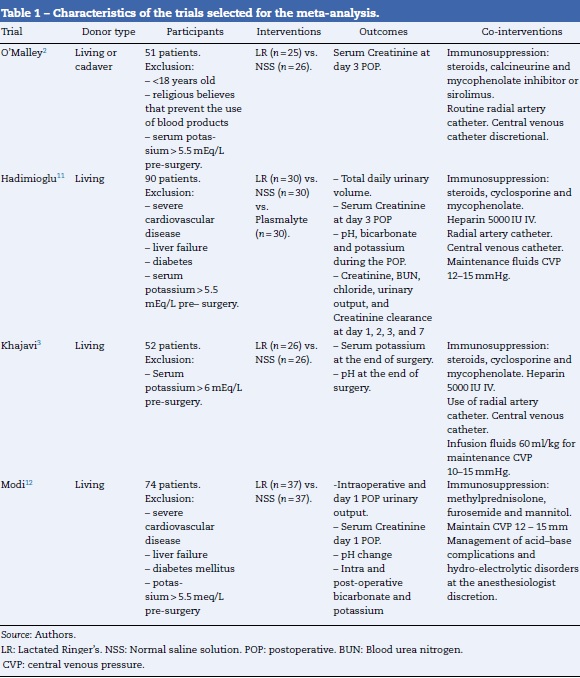
Characteristics of the trials included
Four randomized controlled trials were identified with 237 participants that met the inclusion criteria. All of the trials were double blind. The main characteristics of these trials are shown in Table 1. Lactated Ringer's was used as the "experimental" intervention, while NSS was used as the "control"; observation times and follow-up after renal transplantation were variable for the various trials, and hence the results of the measurements at similar time intervals were used to make them comparable.
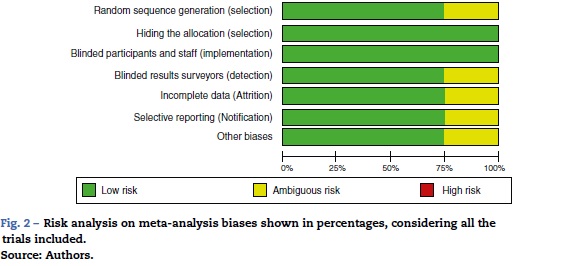
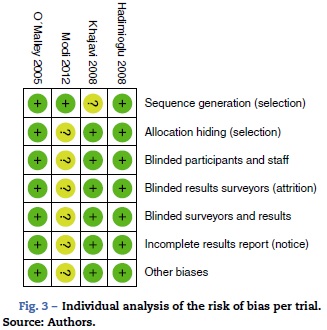
When evaluating the risk of biases in the articles included, we found that most of them used computerized software for randomization. However, the Khajavi et al3. trial is the exception as it fails to indicate how the randomization process was done. All of them used opaque envelopes to hide the allocation and a proper masking method was used in every case. The Modi et al12. trial was classified as "ambiguous risk" due to missing information to rule out any detection, attrition and notification risks. Figs. 2 and 3 illustrate the bias risks.
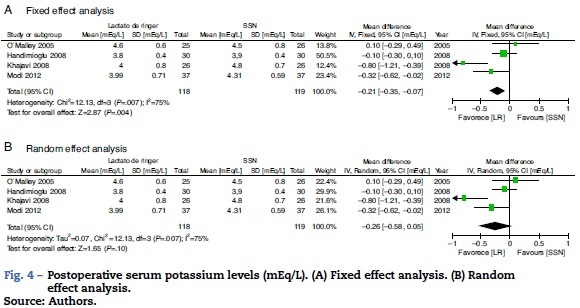
The results considered for the analysis included the laboratory measurements during the perioperative period that the authors rated as most significant. The potassium difference was not significant at the end of surgery (mean difference (MD): -0.26 mEq/L; 95% CI: -0.58 to 0.05; p = 0.10; I2 = 75%) although it was done through fixed effects; RL resulted in a lower value (Fig. 4).
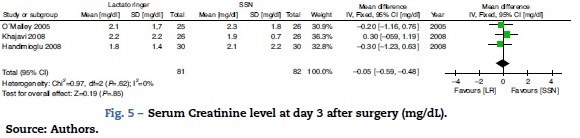
The secondary results considered show that there is no difference in the Creatinine value expressed in mg/dL on the third postoperative day (MD: -0.05; 95% CI: -0.59 to 0.48; p = 0.85; I2 = 0%)(Fig. 5).
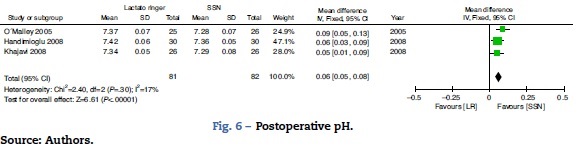
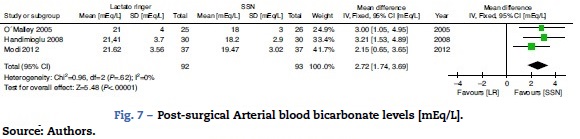
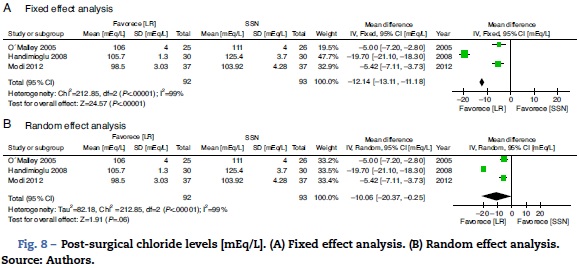
With regard to the acid-base status, the NSS group exhibited higher acidosis, the pH was higher in the LR group (MD: 0.06; 95% CI: 0.05-0.08; p < 0.001; I2 = 17%) (Fig. 6) and bicarbonate was also higher for the LR group (MD: 2.72; 95% CI: 1.74-3.69; p < 0.001; I2 = 0%) (Fig. 7). Chloride was lower during the postoperative period, though based on the random analysis method the value is not statistically significant (MD: 10.06; 95% CI: -20.37 to 0.25; p = 0.06; I2 = 99%) (Fig. 8).
There was no significant statistical difference in the fluid volume infused in liters (MD: -0.01; 95% CI: -0.31 to 0.29; p = 0.95; I2 = 56%), though according to fixed methods, the LR group is higher (Fig. 9).
Discussion
Renal transplant has actually become one additional option for the treatment of chronic renal disease15. The 5-year survival is 70%, while the survival for patients that continue on dialysis is only 30%15-19. Patients undergoing renal transplant have multiple comorbidities, including cardiovascular19, hypertension, dyslipidemia, hyperphosphatemia and hyperhomocysteinemia20-23, in addition to pulmonary hypertension24. This represents an anesthetic challenge for the perioperative period25. According to the government data there were 2693 renal transplants in 2008, and 3691 in 2010; this shows a growing number of transplant procedures in the country26,27. General anesthesia is currently the technique of choice; however, regional techniques have proven to be beneficial, particularly in terms of postoperative pain28,29. An in-depth knowledge of the various surgical steps is critical to optimize the surgical conditions30-32.
The use of large volumes of fluids during the intraoperative period has typically reported improved graft function10,25,32-39.
Fluid therapy is a critical element in the intraoperative management of a patient undergoing renal transplantation10,40, particularly because the multiple physiological and pathological variables increase the complexity of the procedure41. Classically, the administration of large volumes of potassium solutions, such as LR, may lead to hyperpotassemia and hence NSS1 has been used instead; several studies indicate that NSS continues to be the choice for this procedure2. Recent studies, however, suggest that more balanced approaches, such as LR, may prevent hyperchloremic metabolic acidosis3-5, and this is not the case if large NSS volumes are used, as has been shown in other types of patients4,8,42-45.
There is some controversy about the best type of crystalloids to use in a RT patient46-48. The use of colloids in these patients is limited48,34 and it is not recommended because of adverse events, including renal failure49-52.
This meta-analysis showed that the administration of LR may be an option for fluid management therapy in renal transplantation since contrary to old beliefs, this solution did not elicit higher hyperpotassemia or higher rates of graft dysfunction as shown by the fact that no differences were identified in the Creatinine values three days after surgery. The potassium difference was not significant at the end of surgery, though when fixed effects were used, LR showed a lower value (Fig. 4). Further analysis of this variable indicated that although there is significant heterogeneity in the results, such heterogeneity decreases upon removing the Khajavi et al.3 trial; the explanation could be the difference in renal ischemia time that was loner in the NSS group. The presence of hyperpotassemia in the NSS group could be mainly explained because potassium acts as a buffer in the presence of acidosis. And, as mentioned above, the administration of large volumes of NSS causes hyperchloremic metabolic acidosis4,8,42-45.
The meta-analysis confirms that the NSS causes metabolic acidosis, probably as a result of hyperchloremia, as illustrated in Figs. 6-8. The patients who received NSS had lower pH values and lover serum bicarbonate, and the data were not heterogeneous for the various trials. Serum chloride was higher in the NSS group, as compared against the patients receiving LR, though there is significant heterogeneity with this particular variable. It should be mentioned however that other anions such as sulfates and phosphates, inter alia, may accumulate in patients with chronic renal disease; nevertheless, crystalloids do not affect the concentration and chloride could be the key factor in the development of metabolic acidosis52. To this date, several trials show that hyperchloremia per se could be the cause for an unfavorable outcome in renal function44,45,52-54. The success in preventing perioperative complications includes proper patient identification and optimization, with an anesthetic plan that integrates the various variables affecting the evolution of the renal transplant. It should be highlighted however, that no significant differences were identified between the 2 groups in terms of amount of infused solution in the three trials analyzed; this certainly deserves some consideration since classically hyperchloremic metabolic acidosis has been associated with the infusion of large volumes of fluids. Further trials with larger numbers of patients and long-term follow-up are needed, in order to obtain a better understanding of the clinical implications of hyperchloremic metabolic acidosis.
The clinically relevant result, Creatinine levels at day 3, showed no differences between the two groups. This indicates that the administration of LR is safe for patients undergoing renal transplantation surgery. The heterogeneity of the trials is low in terms of this variable, making the result even stronger. No adverse effects were described in any of the trials using Lactated Ringer's therapy, so no conclusions can be made on this particular point.
This meta-analysis exhibits a number of limitations including the small number of trials and a small number of patients, in addition to differences in follow-up times and in the variables evaluated. The observation and follow-up times after renal transplantation varied among the various trials, but the results of the measurements used were from similar time intervals to make them comparable. The outcome that evaluates renal function using 3rd postoperative day Creatinine was only reported in three trials. This limits the interpretation of this variable, because the number of patients is further reduced. The heterogeneity of some of the variables was important; however, it is impossible to avoid heterogeneity in this type of trials, considering the differences in the populations evaluated, the respective treatment protocols and the duration of the trials. The Nuraei et al13. trial was excluded because it was written in Farsi and despite numerous attempts to contact the authors, no replies were received. The exclusion criteria were strict and hence some patients with cardiovascular complications could have been excluded preventing a definite conclusion about this group of patients.
Nevertheless, this paper may still be the best available evidence to approach the issue of identifying the best fluid therapy option for patients undergoing kidney transplantation procedures.
Conclusion
The use of LR in the perioperative period of renal transplant procedures results in similar potassium levels during the postoperative period, higher pH and bicarbonate levels, and lower chloride, with no significant changes on the 3rd day postoperative Creatinine values, despite using a similar infusion volume as compared to NSS.
Ethical disclosures
Protection of human and animal subjects. The authors declare that no experiments were performed on humans or animals for this study.
Confidentiality of dat. The authors declare that no patient data appear in this article.
Right to privacy and informed consent. The authors declare that no patient data appear in this article.
Conflicts of interest
The authors have no conflict of interests to declare.
Funding
The authors did not receive sponsorship to undertake this article.
References
1. O'Malley CM, Frumento RJ, Bennett-Guerrero E. Intravenous fluid therapy in renal transplant recipients: results of a US survey. Transplant Proc. 2002;34:3142-5. [ Links ]
2. O'Malley CM, Frumento RJ, Hardy MA, Benvenisty AI, Brentjens TE, Mercer JS, et al. A randomized, double-blind comparison of Lactated Ringer's solution and 0.9% NaCl during renal transplantation. Anesth Analg. 2005;100:1518-24. [ Links ]
3. Khajavi MR, Etezadi F, Moharari RS, Imani F, Meysamie AP, Khashayar P, et al. Effects of normal saline vs. Lactated Ringer's during renal transplantation. Ren Fail. 2008;30:535-9. [ Links ]
4. Scheingraber S, Rehm M, Sehmisch C, Finsterer U. Rapid saline infusion produces hyperchloremic acidosis in patients undergoing gynecologic surgery. Anesthesiology. 1999;90:1265-70. [ Links ]
5. Prough DS, Bidani A. Hyperchloremic metabolic acidosis is a predictable consequence of intraoperative infusion of 0.9% saline. Anesthesiology. 1999;90:1247-9. [ Links ]
6. Yunos NM, Bellomo R, Story D, Kellum J. Bench-to-bedside review: chloride in critical illness. Crit Care. 2010;14:226. [ Links ]
7. Kaufman D, Kitching AJ, Kellum JA. Acid-base balance. In: Principles of critical care. 3rd edition New York: Gregory & Hall, McGraw-Hill; 2005. p. 1201-8. [ Links ]
8. Williams EL, Hildebrand KL, McCormick SA, Bedel MJ. The effect of intravenous Lactated Ringer's solution versus 0.9% sodium chloride solution on serum osmolality in human volunteers. Anesth Analg. 1999;88:999-1003. [ Links ]
9. Meier-Kriesche HU, Port FK, Ojo AO, Rudich SM, Hanson JA, Cibrik DM, et al. Effect of waiting time on renal transplant outcome. Kidney Int. 2000;58:1311-7. [ Links ]
10. Lemmens HJ. Kidney transplantation: recent developments and recommendations for anesthetic management. Anesthesiol Clin North Am. 2004;22:651-62. [ Links ]
11. Hadimioglu N, Saadawy I, Saglam T, Ertug Z, Dinckan A. The effect of different crystalloid solutions on acid-base balance and early kidney function after kidney transplantation. Anesth Analg. 2008;107:264-9. [ Links ]
12. Modi MP, Vora KS, Parikh GP, Shah VR. A comparative study of impact of infusion of Ringer's Lactate solution versus normal saline on acid-base balance and serum electrolytes during live related renal transplantation. Saudi J Kidney Dis Transpl. 2012;23:135-7. [ Links ]
13. Nuraei N, Khajenouri R, Soleimani M, Dabbagh A. The effects of intraoperative normal saline versus Lactated Ringer solution on clinical outcomes and laboratory findings in renal transplant patients. Tehran Univ Med J. 2010;68:872-7. [ Links ]
14. Higgins J, Green S. Cochrane handbook for systematic reviews of interventions 5.1.0. The Cochrane collaboration 2011. Available from: http://handbook.cochrane.org/ [Citado 06.02.14] [ Links ].
15. Wolfe RA, Ashby VB, Milford EL, Ojo AO, Ettenger RE, Agodoa LY, et al. Comparison of mortality in all patients on dialysis, patients on dialysis awaiting transplantation, and recipients of a first cadaveric transplant. N Engl J Med. 1999;341:1725-30. [ Links ]
16. Rabbat CG, Thorpe KE, Russell JD, Churchill DN. Comparison of mortality risk for dialysis patients and cadaveric first renal transplant recipients in Ontario, Canada. J Am Soc Nephrol. 2000;11:917-22. [ Links ]
17. Ojo AO, Hanson JA, Meier-Kriesche H, Okechukwu CN, Wolfe RA, Leichtman AB, et al. Survival in recipients of marginal cadaveric donor kidneys compared with other recipients and wait-listed transplant candidates. J Am Soc Nephrol. 2001;12:589-97. [ Links ]
18. Brunkhorst R, Lufft V, Dannenberg B, Kliem V, Tusch G, Pichlmayr R. Improved survival in patients with type 1 diabetes mellitus after renal transplantation compared with hemodialysis: a case-control study. Transplantation. 2003;76:115-9. [ Links ]
19. U.S. Renal Data System. USRDS 2013 annual data report: Atlas of chronic kidney disease and end-stage renal disease in the United States, National Institutes of Health, National Institute of Diabetes and Digestive and Kidney Diseases, Bethesda, MD; 2013. Available from: http://www.usrds.org/adr.aspx [Citado 06.02.14] [ Links ].
20. Locatelli F, Bommer J, London GM, Martín-Malo A, Wanner C, Yaqoob M, et al. Cardiovascular disease determinants in chronic renal failure: clinical approach and treatment. Nephrol Dial Transplant. 2001;16:459-68. [ Links ]
21. Arici M, Walls J. End-stage renal disease, atherosclerosis, and cardiovascular mortality: is C-reactive protein the missing link? Kidney Int. 2001;59:407-14. [ Links ]
22. Lagrand WK, Visser CA, Hermens WT, Niessen HW, Verheugt FW, Wolbink GJ, et al. C-reactive protein as a cardiovascular risk factor: more than an epiphenomenon? Circulation. 1999;100:96-102. [ Links ]
23. Yigla M, Nakhoul F, Sabag A, Tov N, Gorevich B, Abassi Z, et al. Pulmonary hypertension in patients with end-stage renal disease. Chest. 2003;123:1577-82. [ Links ]
24. Rivera D, Tejada JH, Medina A, Martinez E, Nieto N. Anesthesia complications in renal transplantation. Rev Colomb Anestesiol. 2011;39:30-7. [ Links ]
25. Social MdP. Informe de pacientes trasplantados por departamento y EPS en Colombia; 2008-2010. Available from: http://www.cuentadealtocosto.org/byblos/Docs/Informe_de-trasplante_renal_enXolombia_segun_Departamento_2011.pdf [Citado 06 02 14] [ Links ].
26. Cubillos J, Sandoval CL, Andrade E, Hermida NH. Causas que contribuyen a la pérdida del trasplante renal de donante cadaverico en la fundación Surcolombiana de Trasplantes. Febrero 2007 a noviembre 2012, Neiva, Colombia. Rev Colomb Anestesiol. 2014;42:83-9. [ Links ]
27. Hirata ES, Baghin MF, Pereira RI, Alves Filho G, Udelsmann A. Influence of the anesthetic technique on the hemodynamic changes in renal transplantation: a retrospective study. Rev Bras Anestesiol. 2009;59:166-76. [ Links ]
28. Bhosale G, Shah V. Combined spinal-epidural anesthesia for renal transplantation. Transplant Proc. 2008;40:1122-1. [ Links ]
29. Humar A, Kerr SR, Ramcharan T, Gillingham KJ, Matas AJ. Peri-operative cardiac morbidity in kidney transplant recipients: incidence and risk factors. Clin Transplant. 2001;15:154-8. [ Links ]
30. Flechner SM. Current status of renal transplantation patient selection, results, and immunosuppression. Urol Clin North Am. 1994;21:265-82. [ Links ]
31. Luciani J, Frantz P, Thibault P, Ghesquièrre F, Conseiller C, Cousin MT, et al. Early anuria prevention in human kidney transplantation Advantage of fluid load under pulmonary arterial pressure monitoring during surgical period. Transplantation. 1979;28:308-12. [ Links ]
32. Carlier M, Squifflet JP, Pirson Y, Gribomont B, Alexandre GP. Maximal hydration during anesthesia increases pulmonary arterial pressures and improves early function of human renal transplants. Transplantation. 1982;34:201-4. [ Links ]
33. Thomsen HS, L0kkegaard H, Munck O. Influence of normal central venous pressure on onset of function in renal allografts. Scand J Urol Nephrol. 1987;21:143-5. [ Links ]
34. Dawidson IJ, Ar'Rajab A. Perioperative fluid and drug therapy during cadaver kidney transplantation. Clin Transpl. 1992:267-84. [ Links ]
35. Niemann CU, Eilers H. Abdominal organ transplantation. Minerva Anestesiol. 2010;76:266-75. [ Links ]
36. Marik PE, Baram M, Vahid B. Does central venous pressure predict fluid responsiveness? A systematic review of the literature and the tale of seven mares. Chest. 2008;134: 172-8. [ Links ]
37. Ferris RL, Kittur DS, Wilasrusmee C, Shah G, Krause E, Ratner L. Early hemodynamic changes after renal transplantation: determinants of low central venous pressure in the recipients and correlation with acute renal dysfunction. Med Sci Monit. 2003;9:CR61-6. [ Links ]
38. De Wilde RB, Schreuder JJ, van den Berg PC, Jansen JR. An evaluation of cardiac output by five arterial pulse contour techniques during cardiac surgery. Anaesthesia. 2007;62:760-8. [ Links ]
39. Feltracco P, Ori C. Anesthetic management of living transplantation. Minerva Anestesiol. 2010;76:525-33. [ Links ]
40. Brandstrup B. Fluid therapy for the surgical patient. Best Pract Res Clin Anaesthesiol. 2006;20:265-83. [ Links ]
41. McFarlane C, Lee A. A comparison of Plasmalyte 148 and 0.9% saline for intra-operative fluid replacement. Anaesthesia. 1994;49:779-81. [ Links ]
42. Waters JH, Gottlieb A, Schoenwald P, Popovich MJ, Sprung J, Nelson DR. Normal saline versus Lactated Ringer's solution for intraoperative fluid management in patients undergoing abdominal aortic aneurysm repair: an outcome study. Anesth Analg. 2001;93:817-22. [ Links ]
43. Gan TJ, Bennett-Guerrero E, Phillips-Bute B, Wakeling H, Moskowitz DM, Olufolabi Y, et al. Hextend, a physiologically balanced plasma expander for large volume use in major surgery: a randomized phase III clinical trial. Hextend Study Group. Anesth Analg. 1999;88:992-8. [ Links ]
44. Wilcox CS. Regulation of renal blood flow by plasma chloride. J Clin Invest. 1983;71:726-35. [ Links ]
45. Ricaurte L, Vargas J, Lozano E, Diaz L, Organ Transplant Group. Anesthesia and kidney transplantation. Transplant Proc. 2013;45:1386-91. [ Links ]
46. Schmid S, Jungwirth B. Anaesthesia for renal transplant surgery: an update. Eur J Anaesthesiol. 2012;29: 552-8. [ Links ]
47. Dawidson I, Peters P, Sagalowsky A, Abshier D, Coorpender L. 51. The effect of intraoperative fluid management on the incidence of acute tubular necrosis. Transplant Proc. 1987;19:2056-7. 52. [ Links ]
48. Willms CD, Dawidson IJ, Dickerman R, Drake D, Sandor ZF, Trevino G. Intraoperative blood volume expansion induces primary function after renal transplantation: a study of 96 paired cadaver kidneys. Transplant Proc. 1991;23:1338-9. 53. [ Links ]
49. Bunn F, Alderson P, Hawkins V. Colloid solutions for fluid resuscitation. Cochrane Database Syst Rev. 2003;1:CD001319. Review. Update in: Cochrane Database Syst Rev. 2008;1:CD001319. [ Links ]
50. Laxenaire MC, Charpentier C, Feldman L. Anaphylactoid 54. reactions to colloid plasma substitutes: incidence, risk factors, mechanisms. A French multicenter prospective study. Ann Fr Anesth Reanim. 1994;13:301-10. [ Links ]
51. Wilcox CS, Peart WS. Release of renin and angiotensin II into plasma and lymph during hyperchloremia. Am J Physiol. 1987;253:F734-41. [ Links ]
52. Etezadi F, Pourfakhr P, Mojtahedzade M, Najafi A, Moharari RS, Yarandi KK, et al. Effects of tight versus non tight control of metabolic acidosis on early renal function after kidney transplantation. Daru. 2012;20:36. [ Links ]
53. McCluskey SA, Karkouti K, Wijeysundera D, Minkovich L, Tait G, Beattie WS. Hyperchloremia after noncardiac surgery is independently associated with increased morbidity and mortality: a propensity-matched cohort study. Anesth Analg. 2013;117:412-21. [ Links ]
54. González VH, Vargas GJ, Echeverri JE, Díaz SM, Mena Y. Valoración preanestésica en el paciente con enfermedad renal crónica (énfasis en riesgo cardiovascular). Rev Colomb Anestesiol. 2013;41:139-45. [ Links ]
