










Services on Demand
Journal
Article
 text in
text in  English (pdf)
English (pdf)
 Article in xml format
Article in xml format Article references
Article references
 Send this article by e-mail
Send this article by e-mailIndicators
-
 Cited by SciELO
Cited by SciELO -
 Access statistics
Access statistics
Related links
-
 Cited by Google
Cited by Google -
 Similars in
SciELO
Similars in
SciELO -
 Similars in Google
Similars in Google
Share

 Permalink
PermalinkColombian Journal of Anestesiology
Print version ISSN 0120-3347
Rev. colomb. anestesiol. vol.43 no.3 Bogotá July/Sept. 2015
Case report
Recurrent hepatic artery thrombosis in three instances of liver transplant in a single patient: Case report*
Trombosis recurrente de la arteria hepática en tres trasplantes hepáticos sobre el mismo paciente: informe de caso
Jesús Acosta-Martíneza,**, Rosana Guerrero-Domíngueza, Daniel López-Herrera Rodrígueza, Marta López-Sánchezb
a MD, UGC in Anaesthesiology and Resuscitation, Hospital Universitario Virgen del Rocío, Seville, Spain
b MD, Staff Physician, Resuscitation Unit, Hospital Universitario A Coruña, Coruña, Spain
* Please cite this article as: Acosta-Martínez J, Guerrero-Domínguez R, López-Herrera Rodríguez D, López-Sánchez M. Trombosis recurrente de la arteria hepática en tres trasplantes hepáticos sobre el mismo paciente: Informe de caso. Rev Colomb Anestesiol. 2015;43:237-240.
** Corresponding author at: Calle Castillo de Marchenilla No. 5, núcleo 1, 3°C, CP 41013 Seville, Spain.
E-mail address: acostamartinez.jesus@gmail.com (J. Acosta-Martínez).
Article info
Article history: Received 23 April 2014 Accepted 11 February 2015 Available online 16 May 2015
Abstract
Introduction: Orthotopic liver transplantation (OLT) is currently the treatment of choice for patients with end-stage liver disease. Vascular complications can trigger a failure of treatment, so it must be watched closely.
Clinical, diagnostic evaluation and interventions: We report the case of a patient taken three times to liver transplantation due to recurrent hepatic artery thrombosis. The perfusion defect persisted after the third transplant, although the short-term course was favourable.
Conclusion: Hepatic artery thrombosis varies in its clinical presentation, but it usually requires early and aggressive management.
Keywords: Thrombosis, Hepatic artery, Hepatic failure, Patients, Perfusion.
Resumen
Introducción: El trasplante ortotópico hepático (TOH) es actualmente el tratamiento de elección para pacientes con enfermedades hepáticas terminales. Las complicaciones vasculares pueden desencadenar un fracaso del tratamiento, por lo que deben ser vigiladas estrechamente.
Hallazgos clínicos, evaluación diagnóstica e intervenciones: presentamos el caso de un paciente sometido en tres ocasiones a trasplante hepático por trombosis recurrente de la arteria hepática. Tras el tercer trasplante persiste el defecto de perfusión, pese a lo cual la evolución a corto plazo fue favorable.
Conclusión: las presentaciones clínicas de la trombosis de la arteria hepática son variables, pero suelen requerir un manejo agresivo y precoz.
Palabras clave: Trombosis, Arteria Hepática, Fallo Hepático, Pacientes, Perfusión.
Introduction
Orthotopic liver transplant (OLT) has become the treatment of choice in cases of end-stage liver disease. In the immediate postoperative period, it is critical to identify life-threatening complications for the patient and the graft. Of these, vascular complications (hepatic artery, portal vein, inferior vena cava or suprahepatic veins) pose a diagnostic challenge for the critical care physician, given a prevalence of approximately 9% and the potentially devastating consequences1,2, requiring early surgical treatment in the majority of cases.
Adequate blood supply from the hepatic artery (HA) is essential in OLT, because hypoperfusion triggers graft ischaemia and necrosis, favouring colonization by microorganisms that may be lethal for the patient in the event timely diagnosis and treatment are not achieved3. Four causes of hepatic artery hypoperfusion have been described: arterial thrombosis, stenosis, pseudoaneurysm and arterial steal syndrome.
Clinical case
The following is the case of a patient taken to retransplant surgery three times due to hepatic artery thrombosis (initial indication was alcoholic cirrhosis and hepatocarcinoma), with residual HA thrombosis after the third transplant surgery.
Patient information
A 65-year-old retired patient was presented with a history of chronic alcoholism (stopped drinking 13 months before the transplant), smoking, and alcoholic cirrhosis (compounded by hepatic encephalopathy, hydropic decompensation and oesophageal varices I/II). During follow-up of his liver disease, a lesion was found in the right hepatic lobe, suggestive of hepatocarcinoma. The patient was listed for liver transplant. The initial clinical course was favourable and the patient was discharged home.
Clinical findings, diagnostic assessment and interventions
Five months after transplant, the patient was taken to cholan-giography due to a laboratory test showing a pattern of cholestasis. A mismatch was found between donor and recipient biliary tract size and the patient was then submitted to endoscopic retrograde cholangiopancreatography (ERCP) for stenting. Given that there was no improvement despite this procedure, hepaticojejunostomy and surgical biliary tract cleansing were performed, and the patient was discharged home.
One month later, the patient was admitted because offever, and an abdominal CT scan revealed bilioportal fistula and biliary tract necrosis as a result of hypoperfusion through the hepatic artery (seen on the arteriogram). Consequently, the patient was listed for retransplant and the procedure was performed the following month.
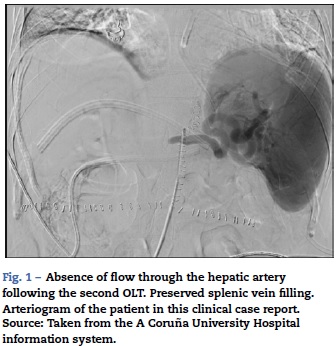
After the second OLT, despite the fact that the patient evolved well from the clinical and laboratory standpoint, a follow-up Doppler ultrasound of the graft performed after the first 24 h showed absence of flow through the hepatic artery, probably due to a surgical complication. Arteriogra-phy was performed (Fig. 1), confirming the diagnosis, and the patient was taken to surgery for thromboectomy and angioplasty plus the postoperative addition of intraportal prostaglandin E1 infusion4 (through a ligamentum teres intra-operative approach). However, ultrasound again showed a persistent perfusion defect leading to urgent retransplantation performed within the following 48 h, in which the surgical team transferred the arterial anastomosis to the splenic artery.
Calendar
Not specified due to the clinical case format.
Follow-up and result
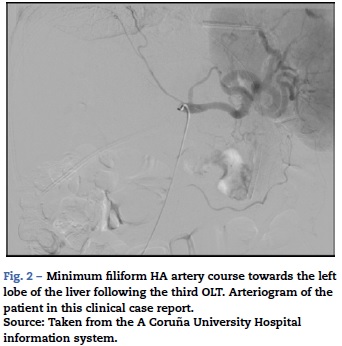
The postoperative course was uneventful, except for isolates in cultures taken through the Kher of Enterococcus faecium and Staphylococcus aureus with prior initiation of empirical treatment with imipenem, linezolid and anidulafungin. The patient evolved well from the clinical and laboratory standpoint but liver Doppler performed within the first postoperative hours and the follow-up arteriogram showed absence of arterial flow to the graft (Fig. 2). In view of the sequence of events, the decision was made to wait and see. The patient had an adequate postoperative recovery and was eventually discharged 12 days after the last transplant. Seven months after hospital discharge, the patient was taken to elective surgery for hepaticojejunostomy because of biliary tract hypoperfusion.
Discussion
Discussion of the medical literature
HA thrombosis is the most frequent vascular complication, accounting for up to 60% of all vascular complications in some series, with an incidence of approximately 3-5% in adult liver transplantation (higher in children). It is associated with high mortality and it is the second cause of early liver failure and one of the main reasons for retransplantation.
Risk factors for this complication include acute rejection, anatomical mismatch between the donor and the recipient, prolonged cold ischaemia of the graft, CMV infection, arterial diameter <3 mm, low intra-operative arterial flow, inti-mal damage during the anastomosis or associated with prior chemoembolizations, advanced donor age, and Leiden factor V mutation5,6.
The clinical presentation depends primarily on the time of onset, because it may be early (<2-4 weeks) or late. In the early phase, findings show ischaemic liver failure with elevated cytolysis enzymes and diminished bile production, and even biliary tract infections due to necrosis as a result of biliary tract dependence on arterial blood supply only. Biliary complications may also occur with late presentation, where there is a possibility of developing collateral circulation, although usually not sufficient to avoid retransplantantion7. Finally, there are case descriptions of asymptomatic patients where HA thrombosis is found incidentally during follow-up ultrasound8.
As far as diagnosing the condition is concerned, echo Doppler has been shown to have good sensitivity and specificity (70-100% and 97-100%, respectively)9. The most frequent ultrasound pattern is absent HA pulse in the liver hilum and the main branches. Reference techniques include arteriography and angio-CT, which must be performed in patients with suspected HA thrombosis in whom echo Doppler findings are inconclusive. Given potential complications, some centres advocate the use of serial Doppler ultrasound imaging for routine monitoring of OLT, while others use ultrasound driven by the clinical findings.
In the event of confirmed suspicion or high probability of HA thrombosis, surgical reintervention is required for graft revascularization (thromboectomy), liver retransplant being the option when reoperation is not successful.
Management of our patient
The clinical presentation of hepatic artery thrombosis in our patient has been described in the medical literature10. It is occasionally an incidental finding during follow-up. The peculiarity of the clinical case reported here is the recurrent thrombosis of the HA with latent, non-fulminant clinical manifestations in any of the three OLT, despite the absence of sufficient collateral circulation, leading to the choice of conservative treatment after the third OLT.
Lessons
A proposed improvement over the current intra-operative management of our patient is the need for early intra-operative arterial flow monitoring using Doppler ultrasound of the vascular bed.
Patient perspective and informed consent
We did not interview the patient for confirmation of this experience. Informed consent was obtained for all diagnostic and therapeutic procedures and for the publication of this case, in which no patient identity details are disclosed.
Funding
The authors did not receive sponsorship to undertake this article.
Ethical disclosures
Protection of human and animal subjects. The authors declare that no experiments were performed on humans or animals for this study.
Confidentiality of data. The authors declare that no patient data appear in this article.
Right to privacy and informed consent. The authors declare that no patient data appear in this article.
Conflicts of interest
The authors have no conflict of interests to declare.
References
1. Quiroga S, Sebastia MC, Margarit C, Castells L, Boyé R, Álvarez-Castells A. Complications of orthotopic liver transplantation: spectrum of findings with helical CT. Radiographics. 2001;21:1085-102. [ Links ]
2. Itri JN, Heller MT, Tublin ME. Hepatic transplantation: postoperative complications. Abdom Imaging. 2013;38:1300-33. [ Links ]
3. Langnas AN, Marujo W, Stratta RJ, Wood RP, Shaw BW Jr. Vascular complications after orthotopic liver transplantation. Am J Surg. 1991;161:76-83. [ Links ]
4. Shin M, Song SH, Kim JM, Kim SJ, Joh JW, Lee SK, et al. Effectiveness of intraportal prostaglandin E1 after liver transplantation. Transplant Proc. 2012;44:500-4. [ Links ]
5. Miyagi S, Kawagishi N, Nakanishi W, Fujio A, Miyazawa K, Maida K, et al. Risk factors for hepatic artery thrombosis alter microsurgical vascular reconstruction in liver transplantation. Transplant Proc. 2013;45:1994-6. [ Links ]
6. Fan J, Nishida S, Selvaggi G, Levi D, Tekin A, Weppler D, et al. Factor V Leiden mutation is a risk factor for hepatic artery thrombosis in liver transplantation. Transplant Proc. 2013;45:1990-3. [ Links ]
7. Norhover J, Terblanche J. Bile duct blood supply: its importance in human liver transplantation. Transplantation. 1978;26:67-9. [ Links ]
8. Shaked A, McDiarmid SV, Harrison RE, Gelebert HA, Colonna JO 3rd, Busuttil RW. Hepatic artery thrombosis resulting in gas gangrene of the transplanted liver. Surgery. 1992;111:462-5. [ Links ]
9. Wellings RM, Olliff SP, Olliff JFC, Deakin M, Alton H. Duplex Doppler detection of hepatic artery thrombosis following liver transplantation. Clin Radiol. 1993;47:180-2. [ Links ]
10. Fouzas I, Sklavos A, Bismpa K, Paxiadakis I, Antoniadis N, Giakoustidis D, et al. Hepatic artery thrombosis after orthotopic liver transplantation: 3 patients with collateral formation and conservative treatment. Transplant Proc. 2012;44:2741-4. [ Links ]
