










Services on Demand
Journal
Article
 text in
text in  English (pdf)
English (pdf)
 Article in xml format
Article in xml format Article references
Article references
 Send this article by e-mail
Send this article by e-mailIndicators
-
 Cited by SciELO
Cited by SciELO -
 Access statistics
Access statistics
Related links
-
 Cited by Google
Cited by Google -
 Similars in
SciELO
Similars in
SciELO -
 Similars in Google
Similars in Google
Share

 Permalink
PermalinkColombian Journal of Anestesiology
Print version ISSN 0120-3347
Rev. colomb. anestesiol. vol.43 no.4 Bogotá Oct./Dec. 2015
Review
Utility of ultrasound in resuscitation*
Utilidad del Ultrasonido en Reanimación
Juan David Pérez-Coronadoa,**, Germán Andrés Franco-Gruntoradb
a Resident in Anesthesiology, Fundación Cardioinfantil, Bogotá, Colombia
b Cardiovascular Anesthesiologist, Fundación Cardioinfantil, Bogotá, Colombia
* Please cite this article as: Pérez-Coronado JD, Franco-Gruntorad GA. Utilidad del Ultrasonido en Reanimación. Rev Colomb Anestesiol. 2015;43:321-330.
** Corresponding author at: Calle 163a Número 13B - 60. Segundo Piso Torre A. Fundación Cardioinfantil Instituto de Cardiología. Bogotá, Colombia.
E-mail address: perezjuand@hotmail.com (J.D. Pérez-Coronado).
Article info
Article history: Received 10 September 2014 Accepted 2 March 2015 Available online 6 June 2015
Abstract
Ultrasound has become a diagnostic and therapeutic tool for critical situations. This article reviews the development of ultrasound with respect to critical events and its impact on reducing morbidity and mortality from abdominal and chest trauma, on the recognition of reversible causes of pulseless electrical activity, on decision-making in acute respiratory failure, and on predicting survival and reducing complications associated with invasive procedures. We revised how ultrasounds performed by non-experts with a minimum of training and focused on recognizing specific situations have a good degree of correlation with expert conducted ultrasounds. Some protocols of ultrasound in resuscitation described in the literature are reviewed and a description is made of the most relevant variables in critical situations, including left ventricular function, volume responsiveness, cardiac tamponade, right ventricular dilatation, and pulmonary evaluation.
Keywords: Ultrasonics, Cardiopulmonary resuscitation, Cardiac tamponade, Stroke volume, Ventricular dysfunction Right.
Resumen
El ultrasonido se ha convertido en una herramienta diagnóstica y terapéutica en situaciones críticas. Este artículo revisa la evolución del ultrasonido en eventos críticos y su impacto a través de la disminución de morbimortalidad en trauma abdominal y torácico, en el reconocimiento de causas reversibles en actividad eléctrica sin pulso, en la toma de decisiones en falla ventilatoria aguda, en predicción de supervivencia y en la disminución de complicaciones en procedimientos invasivos. Se revisa cómo el ultrasonido realizado por no expertos con mínimo entrenamiento enfocado al reconocimiento de situaciones específicas tiene una adecuada correlación con el experto. Se revisan algunos protocolos de ultrasonido en reanimación descritos en la literatura y se hace una descripción de las variables más con relevantes en situaciones críticas como la función ventricular izquierda, respuesta a volumen, taponamiento cardíaco, dilatación del ventrículo derecho y la evaluación pulmonar.
Palabras clave: Ultrasonido, Resucitación cardiopulmonar, Taponamiento Cardíaco, Volumen Sistólico, Disfunción ventricular Derecha.
Introduction
Ultrasound technology has become one of the most useful diagnostic and therapeutic tools of our time. Since leaving the exclusive domain of radiologists and being used by Emergency and Intensive Care Unit (ICU) departments, the ultrasound has arrived in the operating room and is now a tool for perioperative care, regional anesthetics, and vascular access.
In the 1970s, the use of echocardiography in the ICU was limited to evaluating systolic volume and cardiac output.1 In the 1980s and 1990s, it quickly developed to aid in the identification of acute events like cardiac tamponade,2 complications from myocardial infarction,3 hemodynamic assessments in cases of hypotension,4 sepsis,5 and the detection of ruptured aortic aneurisms.6
In trauma, the use of the ultrasound began in 1980 in Europe and Japan.7 In 1992, it was used in the USA to detect hemoperitoneum in cases of closed abdominal trauma.8 Rozycki and collaborators demonstrated the effectiveness of ultrasonography in detecting pericardial effusion and intraperitoneal fluid with 81% sensitivity and 99% specificity. They described it with the acronym "FAST" (Focused Abdominal Sonography for Trauma) for evaluating abdominal trauma.9 In 1997, through international consensus, the 'A' was changed from "Abdominal" to "Assessment" and it was included in ATLS.10 In addition, there are a great quantity of studies on the utility of ultrasonography in other scenarios such as pneumothorax,11 hemothorax,12 and vascular accesses.13-15
Thanks to these descriptions, many algorithms for the use of ultrasounds in resuscitation have been published (FATE, CAUSE, RUSH), and, in 2004, the American College of Emergency Physicians (ACEP) considered that bedside ultraso-nography should be integrated into routine practice. In 2010, the American Heart Association guides for advanced life support recommend echocardiography for diagnosing treatable causes of cardiac arrest where defibrillation is impossible and to orient treatment.16
What has been the impact of ultrasonography in resuscitation?
Its impact can be seen in the reduction of morbidity and mortality from trauma, the recognition of potentially reversible causes of non-shockable cardiac arrest and shock, the prediction of survival, in decision-making in cases of acute respiratory failure, and in the reduction of complications from invasive procedures.
Trauma
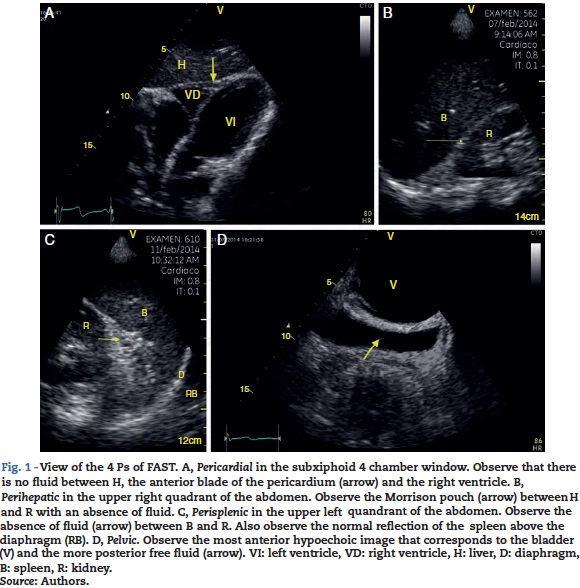
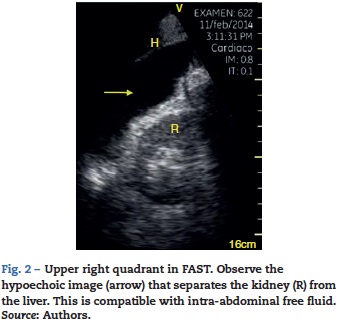
FAST consists of the evaluation of four points (pericardial, perihepatic, perisplenic, and pelvic (Fig. 1)) to detect hypoechoic images related to free pericardial and intra-abdominal fluids of up to 100 ml (Fig. 2) with a sensitivity of 50-88%. Its application has managed to reduce mortality from cardiac and abdominal trauma.17 Its extended application to the thorax (EFAST) for detecting pneumothorax and hemothorax has been very important.18 Firstly this is because it is more sensitive than radiography techniques for diagnosing pneumothorax (48% vs. 20%),17 a pathology that is calculated to be hidden in 5% of all traumas19 and in up to 55% of severe traumas.20 Secondly, echography may detect fluid with a volume of 20 ml while radiography detects 200 ml.21 Thus, echography has a superior sensitivity and specificity when it comes to detecting hemothorax.22
Cardiac arrest and shock
Survival for Pulseless Electric Activity (PEA) and asystole is much less than for other cardiac arrest rhythms. This is probably due to the fact that they depend on the correct identification and rapid treatment of underlying causes.16 Of these causes, only hypoxemia, hypothermia, and hypo/hyperkalemia are easily diagnosed.23 Furthermore, only 45% of physicians correctly diagnose a lack of pulse in cardiac arrest without differentiating between PEA and pseudo PEA. This may lead to physicians not treating a reversible cause.23
In shock, morbidity and mortality also depend on the duration and the rapid treatment of the cause. However, the clinical differentiation between hypovolemic, distributive, car-diogenic, or obstructive shock cannot always be correctly performed24 since the physical examination detects only 57% of cardiac anomalies.25
Ultrasonography plays an important role in these non-shockable cardiac arrest and shock scenarios since it allows physicians to rapidly exclude potentially reversible causes of cardiogenic shock, hypovolemia, cardiac tam-ponade, pneumothorax, and hemothorax.23-25 Moreover, it increases the exactness of the cardiac physical examination by 60-90% for pericardial effusion, left ventricular function, and cardiomegaly.26 It also helps to differentiate a pseudo PEA from a true one so that behavior can be changed in up to 78% of cases.27
Predicting survival
Ultrasonography has been suggested as a tool for ceasing resuscitation since, when there is no evidence of myocar-dial contractility, the probability of return of spontaneous circulation is 3% in cases of PEA28 and the probability of survival is 2% in cases of trauma.29
Acute respiratory failure
Proper decision-making in this scenario was documented in 2008 with the BLUE protocol, an observational study that evaluated criteria like pleural sliding and the consolidation and presence of A or B lines in 3 zones of the thorax called: zone 1 (anterior), zone 2 (lateral), and zone 3 (posterolateral). Each of these zones is halved to create a total of 6 investigation areas. Based on these findings, 6 profiles were established (A, A', B, B', AB, C) that, compared to the final diagnosis, had a sensitivity and specificity of greater than 80% and 90% respectively for detecting COPD, asthma, pneumothorax, pulmonary edema, pneumonia, and pulmonary thromboembolism.30
In addition, echography has a high concordance with radiography in various acute pulmonary pathologies (effusions, consolidation, edema) and can be performed in less time.31
Invasive procedures
When inserting a central venous catheter (CVC), ultrasonography reduced mechanical complications and insertion time, especially in the internal jugular.32 Furthermore, it determines the correct placement of the point of the CVC with a sensitivity of 70% and a specificity of 100% with the saline flush test.33 In cases of thoracentesis, ultrasound increases the probability of success and reduces the risk of organ puncture.34 For pericardiocentesis, the incidence of complications drops 50-4.7%.35
What does a non-expert need to train themselves and how reliable is it?
The American Society of Echocardiography (ASE) determines that the main use of portable ultrasound is to extend the exactitude of the physical examination. It should be objective-guided. For this to take place, at least a basic level of training, including performing 75 examinations and interpreting 150, is required.36
The Council of Emergency Medicine Residency Directors recommends that Emergency training programs include 2 weeks/80 h of training and 150 evaluations in critical situations, including 40 FAST examinations, 30 deep vein thrombosis (DVT) examinations, and 10 procedure examinations.37
Intensive care programs recommend training in general concepts that include the pleura, thorax, vascular system, and abdomen in addition to basic echocardiography to recognize blood volume, biventricular function, cardiac tamponade, and severe acute valve failure.38 10 h of theoretical training in each module and 30 trans-thoracic echocardiograms are recommended.39
Several studies have shown the correlation of non-expert personnel and expert personnel in specific situations. Nien-dorff et al.40 evaluated residents that received training in the subcostal window for recognizing cardiac tampon-ade, pulmonary embolism, hypovolemia, and reduction in contractility with a concordance in 80% over 7 min in PEA scenarios. Another study, performed on residents and involving 100 cases found a strong correlation in terms of the evaluation of left ventricular function, and pleural, pericardial and moderate effusion to quantify vena cava and valve failure in 6 min.41
How to perform and evaluation with echography in resuscitation?
There are many protocols described in the literature that include echocardiography, EFAST, the lung, the aorta, the vena cava, DVT, and ectopic pregnancy, etc. For example, the consensus from the ACEP on echocardiograms at the patient's bedside is focused on pericardial effusion, systolic function, right ventricular growth, intravascular volume, and on confirming transvenous pacemakers.42 The FATE protocol (Focus Assessed Transthoracic Echocardiographic) focuses its evaluation on pericardial effusion, the thickness and dimensions of the heart chambers, contractility, and on the pleura.43 The RUSH (Rapid Ultrasound in Shock) protocol establishes a standpoint for differentiating between hypovolemic, cardiogenic, distributive, and obstructive shock based on 3 variables: (1) The pump (pericardial effusion, left ventricular contractility, and dilation of the right ventricle), (2) the tank (inferior vena cava for hypovolemia, EFAST or pulmonary edema to evaluate leaks and pneumothorax for compression), and (3) the pipes (aortic aneurism and DVT).24
Of these variables we must choose the most relevant ones for evaluating critical events in operating rooms such as shock with unclear etiology, cardiorespiratory arrest with non-shockable rhythms, and hypoxemia. The evaluation should be organized and directed depending on the clinical situation and should include: left ventricular function to rule out myocardial dysfunction, volume responsiveness to evaluate hypovolemia, pericardial effusion for cardiac tamponade, dilation of the right ventricle for pulmonary embolism, and pulmonary ultrasound to rule out pneumothorax, hemothorax, and pulmonary edema.
Left ventricular systolic function
Contractility can be evaluated qualitatively and quickly through the thickening of the endocardium to differentiate between normal and severe dysfunction. This approach is useful for determining the presence of cardiogenic shock and for guiding the use of inotropic/vasopressor medications or intravenous fluids.44 The standard quantitative evaluation is the calculation of the ejection fraction using Simpson's method.
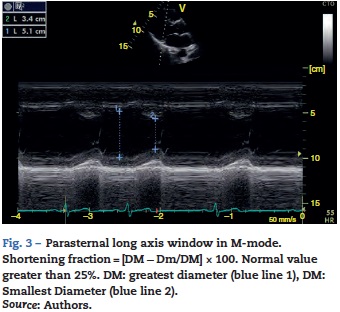
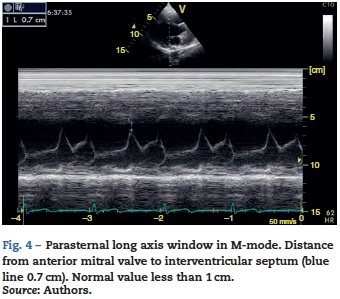
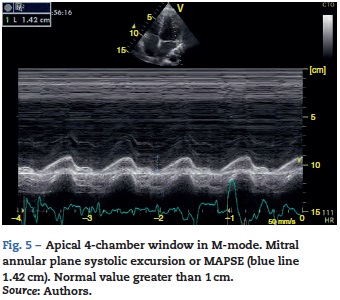
However, this requires 2 planes (apical 4-chamber and 2-chamber) and an advanced calculation that is not always available in these scenarios.45 The M-mode (movement in time) is a more simple method used in the FATE protocol. It allows for the calculation of the shortening fraction (normal greater than 25%) (Fig. 3) and for the approximation of the distance from the anterior mitral valve to the interven-tricular septum (normal less than 1cm) in parasternal long axis (Fig. 4).43 This method should not be considered appropriate in alterations of segmentary contractility.45 The M-mode evaluates systolic function with mitral annular plane systolic excursion (MAPSE) in apical 4-chamber view (normal greater than 15 mm) (Fig. 5).43 Another method is the calculation of systolic volume (normal 45 ± 13 ml) with the Doppler mode and the formula Pi x R2 x VTI (velocity time integral) from the left ventricle outflow tract (LVOT), where R is the radius of the LVOT. The VTI is also indicative of systolic function with 18-20 cm being normal and less than 12 cm considered shock.45
Blood volume
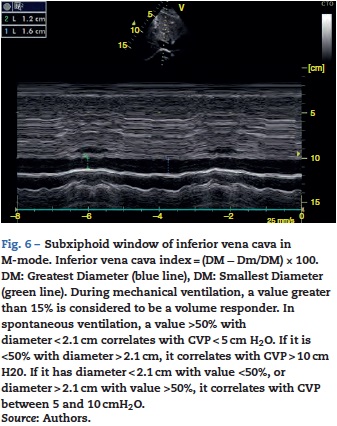
The systolic obliteration of the left ventricle (kissing pap-illar muscle sign) can be related to hypovolemia, although other parameters have shown better predictions of volume responsiveness, such as respiratory changes in the diameter of the vena cava (vena cava index, VCI) (Fig. 6) and in the maximum velocity of the systolic volume. En patients with invasive mechanical ventilation, inferior VCI greater than 15%46 and a superior VCI greater than 36% is considered to be a volume responder.47 In cases of spontaneous respiration, an adequate correlation with volume responsiveness has not been achieved.48 It has, however, been achieved with values of central venous pressure (CVP), given that inferior VCI > 50% with a diameter >2.1 cm correlates with CVP < 5 cm H2O, if it is <50% with diameter > 2.1 cm it correlates with CVP > 10 cm H20, and if it does not comply with either, 5-10 cm H20.49
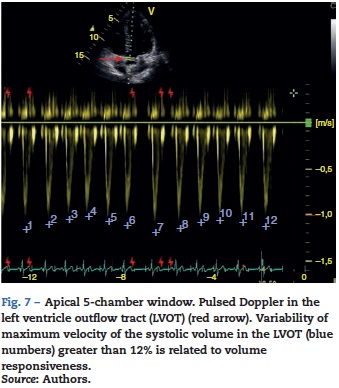
Respiratory changes in the maximum velocity of systolic volume in the LVOT should be greater than 12% to respond to volume (Fig. 7).50
Cardiac tamponade
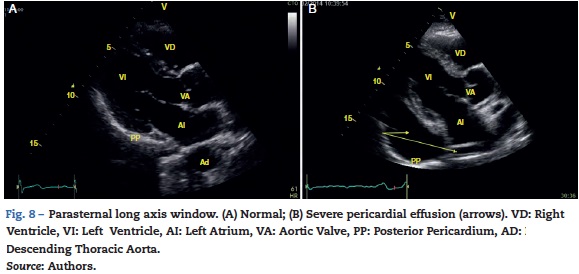
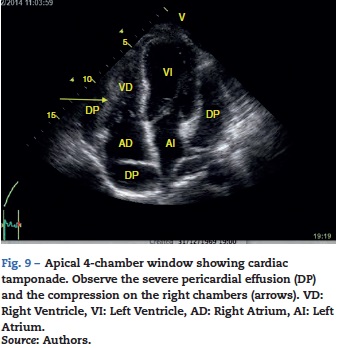
Pericardial effusion is identified as a hypoechoic image between the hyperechoic pericardial blades (Fig. 8) and later it is determined whether it contributes to the patient's instability. As cardiac tamponade is produced when the pressure inside the pericardium impedes filling during the relaxation phase, diastolic collapse should be searched for initially in the right cavities since they have lower pressure (Fig. 9).24,51 The spectrum of presentation of the tamponade can range from an inward deviation of the atrium to a complete compression of the chamber in diastole.51 In addition, a distended inferior vena cava can be seen as part of the diagnosis.24
Right ventricle (RV)
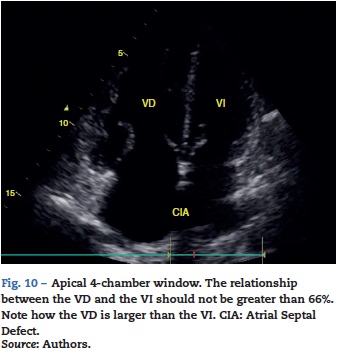
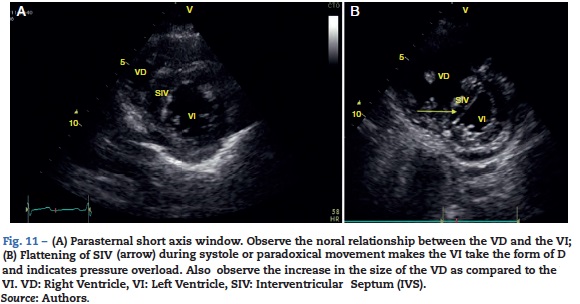
Any condition that suddenly increases pulmonary vascular resistance can result in the acute dilation of the RV. The main cause of this condition is pulmonary embolism.24 This event can be observed through the deformation and dilation of the RV, whose normal relationship with the left ventricle is 66%, and this is better observed in apical 4 chamber or parasternal short axis windows (Fig. 10).49 Another sign that is indicative of an increase in pressure in the RV is the paradoxical movement of the interventricular septum (Fig. 11).24 Some researchers have reported the sensitivity and specificity of the ultrasound for detecting pulmonary embolism as 55% and 69% respectively52 while in the BLUE protocol, a normal pulmonary examination with evidence of DVT indicates PTE with a sensitivity of 81% and a specificity of 99%.28
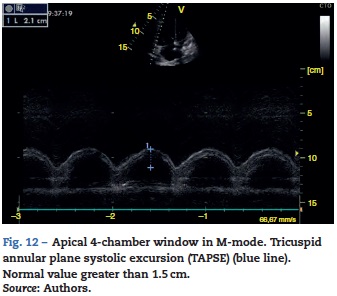
Right ventricular function can also be assessed in M-mode in the apical 4 chamber window with the tricuspid annular plane systolic excursion (TAPSE) that should be greater than 15 mm (Fig. 12).49 The change on the fractional area (area end diastole - area end systole/area end diastole x 100) greater than 35% is indicative of normal systolic function.49
Lung
To rule out pneumothorax, pulmonary edema, consolidation, and pleural effusion in the patient with hypoxemia or shock, we must search for pleural sliding and the A or B lines in the 6 quadrants described in the BLUE protocol as well as signs of pleural effusion.
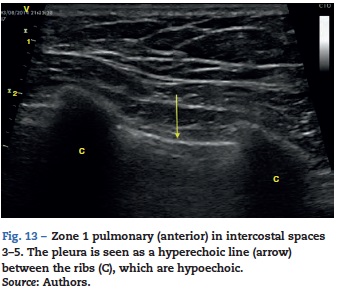
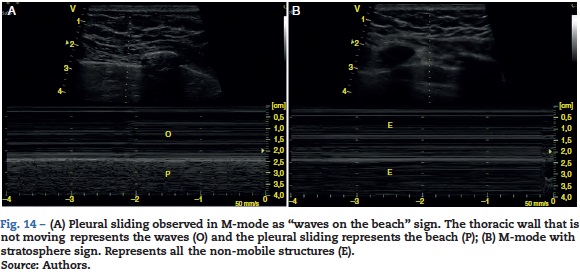
To determine the presence of pneumothorax, with the patient in supine, the pleural line is located (the hypere-chogenic line between the ribs) between intercostal spaces 3-5 and movement of the 2 blades (pleural sliding) should be absent.24 Sliding should also be observed in M-mode as the "waves on a beach" sign (Figs. 13 and 14). In addition, the A lines, which represent horizontal artifacts and are the reflection of the air/tissue interface that causes reverberation between the transductor and the lung, should be searched for. It is key that the A lines be accompanied by an absence of sliding (Profile A') for a diagnosis of pneumothorax, because these lines can be found in healthy individuals or in patients with COPD or asthma (Profile A).28,53,54
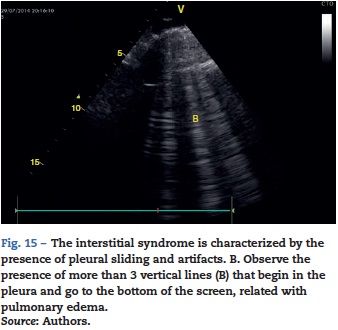
To establish the presence of pulmonary edema, B lines should be identified. These are vertical artifacts of reverberation within the lung that initiate in the pleura toward the bottom of the screen without disappearing and they move with pleural sliding. These B lines with pleural sliding form the interstitial syndrome (Profile B) and are associated with an increase in interstitial water (Fig. 15).28,53,54 When no pleural sliding is present, the B lines are associated with pneumonia, atelactasis, or pulmonary contusions (Profile B').28,53,54
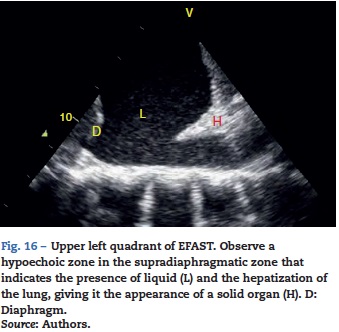
Pleural effusion should be searched for in the perisplenic and perihepatic quadrants of EFAST, moving two intercostal spaces in the direction of the head to locate the diaphragm.24 Normally, in the direction of the head from the diaphragmatic cupola there is a reflection of the spleen or the liver (Fig. 1C) while, in the presence of pleural effusion, a hypoechoic image can be observed and the lung compresses giving it the appearance of a solid organ (hepatization) (Fig. 16).24
Conclusion
Ultrasonography is an important tool for diagnosis and managing critical events, for reducing morbidity and mortality and predicting survival in cases of trauma and PEA, reducing complications from invasive procedures, and improving decision-making in cases of cardiac arrest and acute respiratory failure. Ultrasounds performed by non-experts with a minimum of training focused on recognizing specific situations have an adequate correlation with those performed by experts. The variables of evaluation that are most relevant in critical situations in the operating room are left ventricular function, volume responsiveness, cardiac tamponade, and pulmonary evaluation.
Funding
The authors did not receive sponsorship to undertake this article.
Conflicts of interest
The authors have no conflicts of interest to declare.
References
1. Shors C. Cardiac function determined by echocardiogram. Crit Care Med. 1975;3:5-7. [ Links ]
2. Armstrong WF, Schilt BF, Helper DJ, Dillo JC, Feigenbaum H. Diastolic collapse of the right ventricle with cardiac tamponade: an echocardiographic study. Circulation. 1982;65:1491-6. [ Links ]
3. Horowitz RS, Morganroth J, Parrotto C, Chen CC, Soffer J, Pauletto FJ. Immediate diagnosis of acute myocardial infarction by two dimensional echocardiography. Circulation. 1982;65:323-9. [ Links ]
4. Reichert CLA, Visser CA, Koolen JJ, vd Brink RB, van Wezel HB, Meyne NG, et al. Transesophageal echocardiography in hypotensive patients after cardiac operations. Comparison with hemodynamic parameters. J Thorac Cardiovasc Surg. 1992;104:321-6. [ Links ]
5. Vieillard-Baron A, Prin S, Chergui K, Dubourg O, Jardin F. Hemodynamic instability in sepsis: bedside assessment by Doppler echocardiography. Am J Respir Crit Care Med. 2003;168:1270-6. [ Links ]
6. Vignon P, Gueret P, Vedrinne JM, Lagrange P, Cornu E, Abrieu O, et al. Role of transesophageal echocardiography in the diagnosis and management of traumatic aortic disruption. Circulation. 1995;92:2959-68. [ Links ]
7. Gruessner R, Mentges B, Duber C, Ruckert K, Rothmund M. Sonography versus peritoneal lavage in blunt abdominal trauma. J Trauma. 1989;29:242-4. [ Links ]
8. Tso P, Rodriguez A, Cooper C, Militello P, Mirvis S, Badellino MM, et al. Sonography in blunt abdominal trauma: a preliminary progress report. J Trauma. 1992;33:39-44. [ Links ]
9. Rozycki GS, Ochsner MG, Schmidt JA, Frankel HL, Davis TP, Wang D, et al. A prospective study of surgeon performed ultrasound as the primary adjuvant modality for injured patient assessment. J Trauma. 1995;39:492-8. [ Links ]
10. Scalea TM, Rodriguez A, Chiu WC, Brenneman FD, Fallon WF Jr, Kato K, et al. Focused assessment with sonography for trauma (FAST): results from an international consensus conference. J Trauma. 1999;46:466-72. [ Links ]
11. Dulchavsky SA, Schawarz KL, Kirkpatrick AW, Billica RD, Williams DR, Diebel LN, et al. Prospective evaluation of thoracic ultrasound in the detection of pneumothorax. J Trauma. 2001;50:201-5. [ Links ]
12. Sisley AC, Rozycki GS, Ballard RB, Namias N, Salomone JP, Feliciano DV. Rapid detection of traumatic effusion using surgeon performed ultrasonography. J Trauma. 1998;44:291-6. [ Links ]
13. Vargas F, Gruson D, Valentino R, Bui HN, Salmi LR, Gilleron V, et al. Transesophageal pulsed Doppler echocardiography of pulmonary venous flow to assess left ventricular filling pressure in ventilated patients with acute respiratory distress syndrome. J Crit Care. 2004;19:187-97. [ Links ]
14. Vieillard-Baron A, Prin S, Chergui K, Dubourg O, Jardin F. Echo-Doppler demonstration of acute cor pulmonale in the medical intensive care unit. Am J Respir Crit Care Med. 2002;166:1310-9. [ Links ]
15. National Institute for Clinical Excellence. Guideline on the use of ultrasound location devices for placing central venous catheters. London, 2002. [ Links ]
16. Neumar RW, Otto CW, Link MS, Kronick SL, Shuster M, Callaway CW, et al. Part 8: adult advanced cardiovascular life support: 2010 American Heart Association Guidelines for Cardiopulmonary Resuscitation and Emergency Cardiovascular Care. Circulation. 2010;122 Suppl 3:S729-67. [ Links ]
17. Matsushima K, Frankel HL. Beyond focused assessment with sonography for trauma: ultrasound creep in the trauma resuscitation area and, beyond. Curr Opin Crit Care. 2011;17:606-12. [ Links ]
18. Kirkpatrick AW, Sirois M, Laupland KB, Liu D, Rowan K, Ball CG, et al. Hand-held thoracic sonography for detecting post-traumatic pneumothoraces: the Extended Focused Assessment with Sonography for Trauma (EFAST). J Trauma. 2004;57:288-95. [ Links ]
19. Ball CG, Kirkpatrick AW, Feliciano DV. The occult pneumothorax: what have we learned? Can J Surg. 2009;52:E173-9. [ Links ]
20. Ball CG, Kirkpatrick AW, Laupland KB, Fox DI, Nicolaou S, Anderson IB, et al. Incidence, risk factors and outcomes for occult pneumothoraces in victims of major trauma. J Trauma. 2005;59:917-24. [ Links ]
21. Ma OJ, Mateer JR. Trauma ultrasound examination versus chest radiography in the detection of hemothorax. Ann Emerg Med. 1997;29:312-5. [ Links ]
22. Reardon R, Joing S. Hemothorax after a stab wound to the chest, with clear breath sounds and a normal radiograph. Acad Emerg Med. 2006;13:786. [ Links ]
23. Price S, Uddin S, Laupland KB, Quinn T. Echocardiography in cardiac arrest. Curr Opin Crit Care. 2010;16:211-5. [ Links ]
24. Perera P, Mailhot T, Riley D, Mandavia D. The RUSH Exam: rapid ultrasound in shock in the evaluation of the critically III. Emerg Med Clin North Am. 2010;28:29-56. [ Links ]
25. Arntfield RT, Millington SJ. Point of care cardiac ultrasound applications in the emergency department and intensive care unit-a review. Curr Cardiol Rev. 2012;8:98-108. [ Links ]
26. Martin D, Howell EE, Ziegelstein RC, Martire C, Whiting-O'Keefe QE, Shapiro EP, et al. Hand-carried ultrasound performed by hospitalist: does it improve the cardiac physical examination? Am J Med. 2009;122:35-41. [ Links ]
27. Breitkreutz R, Price S, Steiger HV, Seeger FH, Ilper H, Ackermann H, et al., Emergency Ultrasound Working Group of the Johann Wolfgang Goethe-University Hospital, Frankfurt am Main. Focused echocardiographic evaluation in life support and peri-resuscitation of emergency patients: a prospective trial. Resuscitation. 2010;81:1527-33. [ Links ]
28. Blyth L, Atkinson P, Gadd K, Lang E. Bedside focused echocardiography as predictor of survival in cardiac arrest patients: a systematic review. Acad Emerg Med. 2012;19:1119-26. [ Links ]
29. Cureton EL, Yeung LY, Kwan RO, Miraflor EJ, Sadjadi J, Price DD, et al. The heart of the matter: utility of ultrasound of cardiac activity during traumatic arrest. J Trauma Acute Care Surg. 2012;73. [ Links ]
30. Lichtenstein DA, Meziere GA. Relevance of lung ultrasound in the diagnosis of acute respiratory failure: the BLUE protocol. Chest. 2008;134:117-25. [ Links ]
31. Zanobetti M, Poggioni C, Pini R. Can chest ultrasonography replace standard chest radiography for evaluation of acute dyspnea in the ED? Chest. 2011;139:1140-7. [ Links ]
32. McGee D, Gould MK. Preventing complications of central venous catheterization. N Engl J Med. 2003;348:1123-33. [ Links ]
33. Weekes A, Johnson DA, Keller SM, Efune B, Carey C, Rozario NL, et al. Central vascular catheter placement evaluation using saline flush and bedside echocardiography. Acad Emerg Med. 2014;21:65-72. [ Links ]
34. British Thoracic Society. Pleural disease guideline 2010. A quick reference guide. [ Links ]
35. Tibbles CD, Porcaro W. Procedural applications of ultrasound. Emerg Med Clin North Am. 2004;22:797-815. [ Links ]
36. Seward JB, Douglas PS, Erbel R, Kerber RE, Kronzon I, Rakowski H, et al. Hand-carried cardiac ultrasound (HCU) device: recommendations regarding new, technology. A report from the echocardiography task force on new technology of the Nomenclature and Standards Committee of the American Society of Echocardiography. J Am Soc Echocardiogr. 2002;15:369-73. [ Links ]
37. Puyana JC, Rubiano AM, Hernando Ulloa J, Perdomo MA, editors. Ultrasonido en emergencias y trauma (USET). Bogotá: Distribuna Editorial; 2007. [ Links ]
38. Mayo PH, Beaulieu Y, Doelken P, Feller-Kopman D, Harrod C, Kaplan A, et al. American College of Chest Physicians/La Societé de Réanimation de Langue Francaise statement on competence in critical care ultrasonography. Chest. 2009;135:1050-60. [ Links ]
39. Expert Round Table on Ultrasound in ICU. International expert statement on training standards for critical care ultrasonography. Intensive Care Med. 2011;37:1077-83. [ Links ]
40. Niendorff D, Rassias AJ, Palac R, Beach ML, Costa S, Greenberg M. Rapid cardiac ultrasound of inpatients suffering PEA performed by nonexpert sonographers. Resuscitation. 2005;67:81-7. [ Links ]
41. Mj0lstad OC, Andersen GN, Dalen H, Graven T, Skjetne K, Kleinau JO. Feasibility and reliability of point of care pocket-size echocardiography performed by medical residents. Eur Heart J Cardiovasc Imaging. 2013;14:1195-202. [ Links ]
42. Labovitz AJ, Noble VE, Bierig M, Goldstein SA, Jones R, Kort S. Focused cardiac ultrasound in the emergent setting: a consensus statement of the American Society of Echocardiography and American College of Emergency Physicians. J Am Soc Echocardiogr. 2010;23:1225-30. [ Links ]
43. Jensen MB, Sloth E, Larsen KM, Schmidt MD. Transthoracic echocardiography for cardiopulmonary monitoring in intensive care. Eur J Anaesthesiol. 2004;21:700-7. [ Links ]
44. Cholley BP, Vieillard-Baron A, Mebazaa A. Echocardiography in the ICU: time for widespread use! Intensive Care Med. 2006;32:9-10. [ Links ]
45. Romero-Bermejo FJ, Ruiz-Bailen M, Guerrero-De-Mier M, Lopez-Alvaro J. Echocardiographic hemodynamic monitoring in the critically ill patient. Curr Cardiol Rev. 2011;7:146-56. [ Links ]
46. Barbier C, Loubieres Y, Schmit C, Hayon J, Ricome JL, Jardin F, et al. Respiratory changes in inferior vena cava diameter are helpful in predicting fluid responsiveness in ventilated septic patients. Intensive Care Med. 2004;30:1740-6. [ Links ]
47. Vieillard B, Chergui K, Rabiller A, Peyrouset O, Page B, Beauchet A, et al. Superior vena caval collapsibility as a gauge of volume status in ventilated septic patients. Intensive Care Med. 2004;30:1734-9. [ Links ]
48. Muller L, Bobbia X, Toumi M, Louart G, Molinari N, Ragonnet B, et al. Respiratory variations of inferior vena cava diameter to predict fluid responsiveness in spontaneously breathing patients with acute circulatory failure: need for a cautious use. Crit Care. 2012;16:R188. [ Links ]
49. Rudski L, Lai WW, Afilalo J, Hua L, Handschumacher MD, Chandrasekaran K, et al. Guidelines for the echocardiographic assessment of the right heart in adults: a report from the American Society of Echocardiography endorsed by the European Association of Echocardiography, a registered branch of the European Society of Cardiology, and the Canadian Society of Echocardiography. J Am Soc Echocardiogr. 2010;23:685-713. [ Links ]
50. Slama M, Masson H, Teboul JL, Arnout ML, Susic D, Frohkich E, et al. Respiratory variations of aortic VTI: a new index of hypovolemia and fluid responsiveness. Am J Physiol Heart Circ Physiol. 2002;283:1729-33. [ Links ]
51. Shabetai R. Pericardial effusion: haemodynamic spectrum. Heart. 2004;90:255-6. [ Links ]
52. Mansencal N, Vileillard-Baron A, Beauchet A, Farcot JC, El Hajjam M, Dufaitre G, et al. Triage patients with suspected pulmonary embolism in the emergency department usinga portable ultrasound device. Echocardiography. 2008;25:451-6. [ Links ]
53. Volpicelli G, Elbarbary M, Blaivas M, Lichtenstein DA, Mathis G, Kirkpatrick AW, et al. International Liaison Committee on Lung Ultrasound (ILC-LUS) for International Consensus Conference on Lung Ultrasound(ICC-LUS). International evidence-based recommendations for point-of-care lung ultrasound. Intensive Care Med. 2012;38:577-91. [ Links ]
54. Lichtenstein D. Lung ultrasound in the critically ill. Curr Opin Crit Care. 2014;20:315-22. [ Links ]
