










Services on Demand
Journal
Article
 text in
text in  English (pdf)
English (pdf)
 Article in xml format
Article in xml format Article references
Article references
 Send this article by e-mail
Send this article by e-mailIndicators
-
 Cited by SciELO
Cited by SciELO -
 Access statistics
Access statistics
Related links
-
 Cited by Google
Cited by Google -
 Similars in
SciELO
Similars in
SciELO -
 Similars in Google
Similars in Google
Share

 Permalink
PermalinkColombian Journal of Anestesiology
Print version ISSN 0120-3347
Rev. colomb. anestesiol. vol.44 no.2 Bogotá Apr./June 2016
Scientific and Technological Research
The anaesthetist's role from the patient's perspective*
Rol del anestesiólogo: punto de vista de los pacientes
Jesús Acosta-Martíneza,*, Rosana Guerrero-Domíngueza, Daniel López-Herrera-Rodrígueza, Francisco Sánchez-Carrillob
a Clinical Management, Anaesthesia and Resuscitation Unit, Hospitales Universitarios Virgen del Rocío, Seville, Spain
b Director, Clinical Management, Anaesthesia and Resuscitation Unit, Hospital General Virgen del Rocío, Seville, Spain
* Please cite this article as: Acosta-Martínez J, Guerrero-Rodríguez R, López-Herrera-Rodríguez D, Sánchez-Carrillo F. Rol del anestesiól-ogo: punto de vista de los pacientes. Rev Colomb Anestesiol. 2016;44:121-127.
** Corresponding author at: Calle Castillo de Marchenilla n°5, núcleo 1, 3°C, CP 41013 Sevilla, Spain.
E-mail address: acostamartinez.jesus@gmail.com (J. Acosta-Martínez).
Article history: Received 18 May 2015 Accepted 2 February 2016 Available online 7 April 2016
Abstract
Introduction: Despite advances in anesthesiology over the past decades, patient knowledge regarding the specialty appears to be scant.
Objective: To determine the degree of knowledge among patients about anaesthesiology and the role of anaesthetists, and to identify the demographic factors associated with greater knowledge about the specialty.
Materials and method: Prospective study based on a survey questionnaire conducted in a Level III hospital in Spain, in which all the patients coming for preoperative assessment during a two-week period were interviewed. The survey included questions on different aspects of the specialty covering the preoperative and intraoperative contexts, as well as other areas of anaesthesiology.
Results: Overall, 306 patients were included in the study Of the population interviewed, 80% believe that anaesthetists are specialized physicians. Many patients did not understand the role of the anaesthetist in the treatment of intraoperative medical conditions, the importance of the pre-anaesthesia visit, or the role of the anaesthetist outside the operating room.
Conclusions: The results show that patient knowledge regarding anaesthesia and the role of the anaesthetist is scant, the level of education being the only variable that shows differences between the groups. We believe that anaesthetists and related scientific organizations must try to communicate more information about the speciality in order to help improve health education in the general population, and increase the knowledge about anaesthesiology.
Keywords: Anestesiology, Health surveys, Demographic data, Inpatients, Anesthesia.
Resumen
Introducción: Pese a los avances de la anestesiología en las últimas décadas, el conocimiento por parte de los pacientes sobre la especialidad parece escaso.
Objetivo: Determinar el grado de conocimiento que poseen los pacientes sobre la anestesiología y la función de los anestesiólogos, y establecer qué factores demográficos condicionan un mayor conocimiento de la especialidad.
Material y método: Estudio prospectivo formado por una encuesta-cuestionario realizado en un hospital español de tercer nivel, en el que durante dos semanas se entrevistaron a todos los pacientes que acudieron a la consulta de valoración preoperatoria. El cuestionario incluía preguntas relacionadas con diversos aspectos de la especialidad, desde su vertiente preoperatoria, contextos intraoperatorios y otras áreas de la anestesiología.
Resultados: El estudio pudo completarse en un total de 306 pacientes. El 80% de la población encuestada cree que los anestesiólogos eran médicos especializados. Muchos pacientes no entendieron el papel del anestesiólogo en el tratamiento de cuestiones médicas intraop-eratorias, la importancia de la valoración preanestésica o el papel de los anestesiólogos fuera del quirófano. El factor más relevante que condicionó una tasa mayor de respuestas correctas fue el nivel educativo del paciente.
Conclusiones: Los resultados han mostrado que el conocimiento de los pacientes sobre anestesiología y el papel de los anestesiólogos es escaso, siendo el nivel educativo la única variable que muestra las diferencias entre los grupos. Creemos que los anestesiólogos y las organizaciones científicas relacionadas deben hacer un esfuerzo para proporcionar más información acerca de la especialidad, con el objetivo de mejorar la educación sanitaria de la población general y su conocimiento sobre la anestesiología.
Palabras clave: Anestesiología, Encuestas epidemiológicas, Datos demográficos, Pacientes internos, Anestesia.
Introduction
Despite significant advances in anaesthesiology over the past decades, there is little knowledge in society about the specialty. The lack of information applies to the intraoperative period as well as to the role of the anaesthetist in other healthcare situations (chronic pain unit, postoperative recovery, acute postoperative pain, emergencies). In terms of the surgical process, patients perceive the surgeon as the professional responsible for performing the tasks pertaining to the realm of anaesthesia. Although not many articles have been published on this topic, they have reflected the lack of knowledge about anaesthesiology in many countries,1-4 but this has not been documented in studies conducted in Spain to this date.
Information disseminated in the media regarding the specialty, besides being insufficient, emphasizes complications and legal repercussions associated with the practice of anaesthesia, creating confusion and anxiety when individuals are faced with the possibility of a surgical intervention.5,6
The objective of this study is to determine the degree of knowledge among Spanish patients regarding the specialty of anaesthesia and the role of the anaesthetist inside and outside the operating room. It also seeks to identify patient-related factors that may influence the degree of knowledge, basing the analysis on age, gender, schooling and a history of previous interventions.
Materials and methods
The study was conducted in a level III institution with more than 1100 inpatient beds, 50 operating rooms and approximately 60,000 surgical procedures per year. A survey was given to all adult patients who attended the pre-anaesthesia consultation during the first 2 weeks of June 2014. Overall, 306 questionnaires were completed.
The study was approved by the Ethics Committee of the hospital where it was conducted, and all the patients included gave their consent.
The questionnaire was designed by anaesthesia specialists based on previously published surveys and on the professional experience of the pre-anaesthesia consultation.
The patients completed the questionnaire given to them by nursing staff before the consultation, with no help from the healthcare professionals. The exclusion criteria were patient refusal to participate, inability to read, or being under 18 years of age. We did not find any case of inability to understand the questionnaire.
Patient demographics were included in the first part of the questionnaire (age, sex, schooling and number of prior surgical procedures). After that, the patients were asked to answer 10 multiple choice questions regarding the specialty, given the codes Q1-Q10 (Annex 1; underlined is the answer considered to be right by the authors).
The SPSS software version 22 was used for the statistical analysis. The results were subjected to a descriptive analysis and a comparison between demographic groups (age, sex, schooling and previous procedures) by means of crosstabs using the Chi square or the Fisher's exact test when tables of 2 x 2 are obtained, considering p <0.05 as significant, as well as the corrected remainders. After the crosstabs were done, an individualized analysis was performed of the relationships where p < 0.05. Variables were reformulated for each relationship in order to find statistically significant relations, eliminating the answers that were seldom selected.
Prior recent studies in neighbouring countries have shown that 80% of patients recognize the anaesthetist as being a specialized physician; consequently, we considered a similar estimated percentage in our population. Therefore, for a 95% confidence interval and 5% accuracy, the sample size selected was 300 using the nQuery Advisor® software.
Results
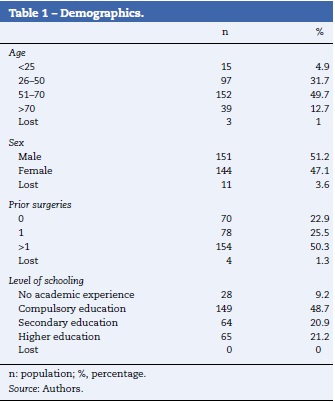
Overall, 306 surveys were conducted. Those that had some unanswered questions were also included in the analysis as lost values. In 50% of cases, age was between 51 and 70. The number of males interviewed was slightly higher. Half of the population interviewed had had surgery more than once in the past, while 22% had never had surgery. Compulsory education was the maximum level of schooling in 48.7% of the sample (Table 1). Therefore, the sample was not homogeneous for "age", "prior surgical procedures" and "schooling". The group analysis was performed according to "age", "sex", "schooling" and "prior surgical procedures".
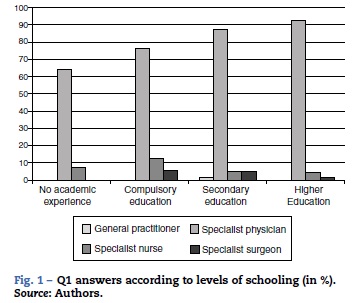
Of the surveyed population, 80% (Q1) recognized the anaesthetist as a specialist physician. A trend to give the correct answer as a function of schooling was found during the comparative analysis between the demographic variables (Fig. 1). When the answers that were just "general practitioner" or "surgeon with specialized training" were eliminated, the proportion of correct answers among the people with higher education or secondary education was 94%, while 29% of those who had no academic experience reported not knowing the answer (p < 0.01).
When asked about the roles of the specialist during a surgical intervention (Q2), 70% of the sample gave the right answer, whereas 23% thought the role consisted only of inducing sleep (or anaesthetize some region of the body) and waking the patient at the end of the procedure. No significant differences were found between the groups, but a growing relationship was found between giving the right answer and the level of schooling (53%, 65%, 72% and 92%, respectively). When the answers that were just "presence not necessary" or "is called only when there are problems" were eliminated, six respondents were lost, but a statistically significant relationship was found between the right answer and the level of schooling (55.6%, 66.2%, 71.9% and 92.2%; p<0.001).
Regarding the selection of a given anaesthetic technique (Q4), 18% of the respondents considered that the anaesthetist uses his/her own experience, the type of intervention, the patient's wishes and characteristics as a basis for making the decision, whereas the rest of the respondents considered that there was only one determining factor of the choice, highlighting the type of intervention in 56% of cases. There were no statistically significant differences between the different population groups.
In terms of blood product transfusions during a surgical procedure (Q6), 12.4% of the respondents answered that this was the responsibility of the anaesthetist, and this percentage was lower than those who believed that it was the job of the haematologist (15%) or the surgeon (49%). In reference to schooling level, a trend of a higher percentage of correct answers with higher schooling was found and it was statistically significant (p < 0.001) when one of the answers was excluded ("depending on the results of the analysis," answered by 13 patients) under Q6.
In relation to the coordination of the response in case of cardiorespiratory arrest (Q10) in the operating room, 16% of the patients surveyed recognized that the anaesthetist is the professional in charge of taking on that role. Another 37.6% considered that the person responsible was the surgeon, 15.7% the cardiovascular surgeon, 4.9% the intensive care physician, and 22% were not able to identify a specific professional. For this question, there was a statistically significant difference between the groups as a function of schooling. Of those who had completed higher education, 26% recognized that the anaesthetist was the professional responsible for taking that role, while the percentages for the other groups were 7%, 12% and 21% (p <0.05).
Of the respondents, 85.9% knew that the route of administration of epidural analgesia or anaesthesia is a lumbar puncture (Q8). In analysing the relationship between gender and the answer to this question, when only the selected answers are eliminated (32 patients are lost), a statistically significant difference in favour of women is obtained (95.8% vs. 81.5%; p <0.05). When asked about the route of administration of general anaesthesia (Q9), only 35.9% were aware of the possibility of administration through the inhaled route or the intravenous route, with statistically significant differences between the groups according to the level of schooling (25.9%, 29.9%, 38.7%, 53.8%; p<0.01). There was also a relationship between the tendency to answer correctly and younger ages of the population (35%, 24%, 14% and 16%).
For the question on the role of the pre-anaesthesia assessment (Q3), 25% of the population gave the wrong answer -thinking that the only role was to weigh and measure the patient (18.6%) or give small doses of anaesthetics in order to assess tolerance (1.6%) - or did not respond. No assumptions of statistically significant differences by demographic groups can be made, although the number of right answers increases as a function of schooling (63%, 70%, 81%, 94%). The pre-anaesthesia visit was not recognized by 27% of the patients as the place to determine the surgical risk, assess the patient's clinical condition and optimize it for the surgery, and no differences were found among the different groups (Q5).
The anaesthetist's roles outside the operating room (Q7) were recognized by 10.5% of the patients surveyed. The remaining 89.5% attributed those roles to other professionals (11.4%) or only identified some of them as pertaining to the specialty (recovery units 66%, postoperative pain 6.9%, and chronic pain units 1.3%). No differences were found between the groups regarding this question.
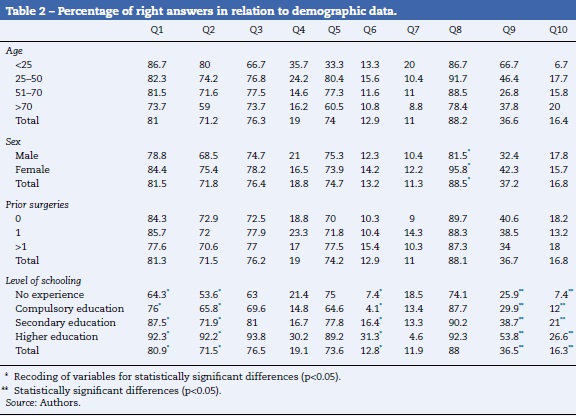
Table 2 shows the overall percentage of right answers by groups, i.e. a descriptive data analysis. The boxes in dark grey highlight the relationships with statistically significant differences after recoding certain variables. The boxes in light grey highlight those relationships with statistically significant differences. Variable recoding was performed in order to exclude from the statistical analysis those questions barely answered because their scatter hampered statistical significance.
Discussion
Patient knowledge about anaesthesiology and the role of the anaesthetist is scant. The data were consistent with previous studies in which the percentage of patients who recognized the anaesthetist as a specialist physician ranged between 49% and 95.5%, and there was no improvement in the data withthe passage of time.7,8 This study showed that 80% of the respondents gave the right answer regarding the level of training. Schooling level is the only variable that showed differences between the groups, where the higher the schooling level the higher the percentage of right answers.
Despite the high number of patients who had knowledge about the anaesthetist's training, the answers from patients who were asked about the roles associated with the specialty are quite striking. The fact that only 12.4% or 16% of the respondents considered that the anaesthetist is responsible for blood product transfusions or for assisting CPR revealed underestimation of the professional and of the specialty per se. In fact, it was peculiar to find that patients believed that it is other specialists who are responsible for those tasks. Regarding these two aspects, it was found that the higher the level of schooling the higher the percentage of right answers.
An area in which the population was found to be informed was the route of administration of epidural anaesthesia, considering that more than 85% answered correctly. This finding maybe attributed to the universal use of epidural analgesia in labour and childbirth, reinforced by the fact that the female patients interviewed had a higher percentage of right answers to the question about the technique.
A similar finding relates to the role of the specialist after anaesthetic induction. In this area, a considerable difference was found depending on the schooling level of the patients. Likewise, too many of the patients interviewed did not attach the importance that pre-anaesthesia assessment and the selection of the adequate anaesthetic technique deserve.
Regarding the roles outside the operating room, they only identified some of the tasks as pertaining to the specialty, mainly care in the recovery units. The figures are lower in this study compared to previous studies, although scant knowledge had also been reported in this area as well.9-12
This poor knowledge about anaesthesiology among patients is in contrast with the growing demand for health information by the population. Consequently, it is of critical importance for anaesthetists to offer more information during pre-anaesthesia visits and to require scientific societies to promote awareness about the specialty. A study published in 2011 found that anaesthetist perception and patient satisfaction increased significantly with just one postoperative visit by the anaesthetist.13 Worth highlighting from this study is the fact that there was no improvement in the knowledge about the specialty as a result of prior surgical experience; this might mean that the information we provide is insufficient or not understood reasonably well. A recent study conducted in Colombia shows similar data to those obtained in this work, despite the high level of patient satisfaction with the work of the anaesthetists.14
Although this study includes data collected from 306 patients surveyed, it is not free of limitations. It was conducted in a single public institution. Even though it shows a positive relationship between knowledge of the subject matter and the level of schooling, this study is not sufficiently powered to make a strong statement. The sample being heterogeneous, particularly in terms of age groups and level of schooling, all results cannot be considered significant even when p < 0.05, as discussed in the section on results.
In conclusion, there is a lack of information among patients about our specialty, as well as little recognition of the roles played by anaesthetists. These data are similar to those obtained in prior studies, some of them even going back to the 1970s, although there are no data regarding the Spanish population in the literature.5 Low schooling level appears to be associated with a greater lack of knowledge, with not too many differences according to age groups, gender or prior surgical experiences. Anaesthetists and the scientific societies that represent them should try to provide more information about the specialty in an attempt to help improve health education in the population.15
Ethical disclosures
Protection of human and animal subjects. The authors declare that no experiments were performed on humans or animals for this study.
Confidentiality of data. The authors declare that no patient data appear in this article.
Right to privacy and informed consent. The authors declare that no patient data appear in this article.
Funding
The authors did not receive sponsorship to undertake this article.
Conflicts of interest
The authors have no conflicts of interest to declare.
References
1. Baaj J, Takrouri MS, Heussein BM, Al Ayyaf H. Saudi patients' knowledge and attitude toward anesthesia and anesthesiologists. A prospective cross-sectional interview questionnaire. Middle East J Anesthesiol. 2006;18:679-91. [ Links ]
2. Tohmo H, Pálve H, Illman H. The work, duties and prestige of Finish anesthesiologists: patients' view. Acta Anaesthesiol Scand. 2003;47:664-6. [ Links ]
3. Braun AR, Leslie K, Morgan C, Bugler S. Patients' knowledge of the qualifications and roles of anesthetists. Anaesth Intensive Care. 2007;35:570-4. [ Links ]
4. de Oliveira KF, Clivatti J, Munechika M, Falcão LF. What do patients know about the work of anesthesiologists? Rev Bras Anestesiol. 2011;61:720-7. [ Links ]
5. Klafta JM, Roizen MF. Current understanding of patients' attitudes toward and preparation for anesthesia: a review. Anesth Analg. 1996;83:1314-21. [ Links ]
6. Lee JJ, Lee NH, Park CM, Hong SJ, Kong MH, Lee KH, et al. Public awareness about the specialty of anesthesiology and the role of anesthesiologists: a national survey. Korean J Anesthesiol. 2014;66:12-7. [ Links ]
7. Irwin MG, Fung SKY, Tivey S. Patient's knowledge of and attitudes towards anaesthesia and anaesthetists in Hong Kong. Hong Kong Med J. 1998;4:16-22. [ Links ]
8. Calman LM, Mihalache A, Evron S, Ezri T. Current understanding of the patient's attitude toward the anesthetist's role and practice in Israel: effect of the patient's experience. J Clin Anesth. 2003;15:451-4. [ Links ]
9. Gottschalk A, Seelen S, Tivey S, Gottschalk A, Rich G. What do patients know about anesthesiologists? Results of a comparative survey in an U.S., Australian, and German university hospital. J Clin Anesth. 2013;25:85-91. [ Links ]
10. Hariharan S, Merritt-Charles L, Chen D. Patient perception of the role of anesthesiologists: a perspective from the Caribbean. J Clin Anesth. 2006;18:504-9. [ Links ]
11. Swinhoe CF, Groves ER. Patientsknowledge of anesthetic practice and the role of anesthetist. Anaesthesia. 1994;49:165-6. [ Links ]
12. Ho RY, Wong DT. Anesthesiology: the misunderstood occupation! Can J Anaesth. 2005;52:208-9. [ Links ]
13. Saal D, Heidegger T, Nuebling M, Germann R. Does a postoperative visit increase patient satisfaction with anesthesia care? Br J Anaesth. 2011;107:703-9. [ Links ]
14. Giraldo VL, Castillo GG, Quintero U, Palacio L, Díaz Y, Palacio M, et al. Percepción de la relación anestesiólogo-paciente valorada en el posoperatorio de pacientes ASA I y II en instituciones nivel III y IV (estudio RAP-2) en Cali, Colombia. Rev Colomb Anestesiol. 2014;42:20-7. [ Links ]
15. Agre P, Kurtz RC, Krauss BJ. A randomized trial using videotape to present consent information for colonoscopy. Gastrointest Endosc. 1994;40:271-6. [ Links ]

