










Services on Demand
Journal
Article
 text in
text in  English (pdf)
English (pdf)
 Article in xml format
Article in xml format Article references
Article references
 Send this article by e-mail
Send this article by e-mailIndicators
-
 Cited by SciELO
Cited by SciELO -
 Access statistics
Access statistics
Related links
-
 Cited by Google
Cited by Google -
 Similars in
SciELO
Similars in
SciELO -
 Similars in Google
Similars in Google
Share

 Permalink
PermalinkColombian Journal of Anestesiology
Print version ISSN 0120-3347
Rev. colomb. anestesiol. vol.44 no.2 Bogotá Apr./June 2016
Case report
Horner syndrome after epidural analgesia for labor. Report on three cases*
Síndrome de Horner tras analgesia epidural para el parto. Informe de 3 casos
Eduardo Rodríguez-Sáncheza,**, Juan Manuel Vadillob, Pablo Herrera-Cálob, María Luisa Marenco de la Fuenteb
a Resident Medical Intern in Anesthesiology and Resuscitation, Hospitales Universitarios Virgen del Rocío, Seville, Spain
b Specialist in Anesthesiology and Resuscitation, Hospitales Universitarios Virgen del Rocío, Seville, Spain
* Please cite this article as: Rodríguez-Sánchez E, Vadillo JM, Herrera-Calo P, Marenco de la Fuente ML. Sindrome de Horner tras analgesia epidural para el parto. Informe de 3 casos. Rev Colomb Anestesiol. 2016;44:170-173.
** Corresponding author at: C/ Persefone, número 7, bloque 37°. 1, 41012 Sevilla, Spain. E-mail address: edurodriguez87@yahoo.es (E. Rodríguez-Sánchez).
Article history: Received 10 August 2015 Accepted 28 January 2016 Available online 16 March 2016
Abstract
Epidural analgesia is assumed to be the technique of choice for the relief of pain in labor. Multiple adverse neurological effects have been reported, one of which is the so-called Horner syndrome (ptosis, myosis, anhidrosis). Its evolution is usually benign and does not require specific management, except clinical monitoring for the more than probable cephalic spread of local anesthetic. Most of the cases that exist in the literature are isolated; in our work we present a series of 3 clinical cases and review the pathogenesis and management in the obstetric patient.
Keywords: Anesthesia epidural, Horner syndrome, Cesarean section, Anesthesia obstetrical, Delivery obstetric.
Resumen
La analgesia epidural supone la técnica de elección para el alivio del dolor del parto. Se han descrito múltiples efectos adversos a nivel neurológico, uno de ellos es el llamado Síndrome de Horner (ptosis,miosis, anhidrosis), suele presentar evolución benigna y no requiere manejo especifico, salvo vigilancia clínica por la más que probable difusión cefálica del anestésico local. La mayor parte de los casos existentes en la literatura son aislados, en nuestro trabajo presentamos una serie de 3 casos clínico y repasamos su etiopatogenía y manejo en la paciente obstétrica.
Palabras clave: Anestesia epidural, Síndrome de Horner, Cesárea, Anestesia obstétrica, Parto.
Introduction
Horner syndrome was first described in 1879 by Swiss ophthalmologist Johann Friedrich Horner. It is characterized by the presence of myosis, ptosis, and anhidrosis, with or without enophthalmos.1 Its primary cause is the ipsilateral interruption of the sympathetic nerve fibers that innervate the pupil, the upper eyelid lifter muscle, and the facial region.2
Any obstacle that affects this neuronal region, from the origin to the last synapse, can lead to this clinical picture. Acquired causes are the most frequent, as are iatrogenic causes due to neuraxial anesthesia, and, in certain populations (such as the obstetric population), the incidence increases considerably due to anatomical and physiological changes that occur. Epidural analgesia is considered the analgesic technique of choice for labor.3 Horner syndrome associated with epidural analgesia for labor was described by Kepes in 1972. Its incidence is estimated at between 0.4 and 4%.4-7
In our study, we present a series of three clinical cases of Horner syndrome in pregnant patients that received epidu-ral analgesia for labor. We also review the physiopathology, implications, and management of the labor.
Clinical case
The technique used in the three cases is described as follows: we use an 18 gauge Touhy needle. The space chosen was L3-L4 with an intervertebral approach. Once the epidural space was located through the loss of resistance to saline technique, a multi-perforated epidural catheter was place 4 cm within the space. The technique was applied in all cases without incident. After the administration of one bolus of 0.16% ropivacaine with 1 [xm/ml of fentanyl, the perfusion of anesthetic at the same concentration was initiated. As a test dose, we used 4ml of bupivacaine at 0.25% with 1/200,000 epinephrine.
Case 1
27-Year-old patient in her first gestation in spontaneous labor at 38 weeks of gestation, 172 cm tall and 75 kg body weight, without medical antecedents of interest. A significant characteristic to highlight was a noticeable lumbar hyperlor-dosis. The epidural catheter was placed at 4cm dilation, after which 11 ml of ropivacaine with fentanyl at the concentration described above was administered. Continuous perfusion of 10mlh-1 of the same anesthetic solution was initiated. She did not receive any supplementary boluses. After the dilation phase and 95 min after the initiation of the perfusion, the patient complained of symptomatology compatible with brachial palsy. After neurological exploration, a motor deficit was observed (level 3 on the Medical Research Council scale) that included the entire upper limb, as well as unspecific soreness at the ipsilateral ocular level with evidence of ptosis, myosis, and anhidrosis compatible with Horner syndrome. The level of sensory block reached T2. After the perfusion was detained, motor and ocular clinical presentation reversed after 115 min.
Case 2
28-Year-old patient in her first gestation in spontaneous labor at 37 weeks of gestation. 160 cm tall and 55 kg body weight without personal antecedents of interest. 8 ml of ropivacaine and fentanyl were administered in the initial bolus followed by continuous perfusion at 8mlh-1. The patient received two supplementary boluses, first 30min after the start of perfusion, and the second 45 min after the previous bolus. During the dilation phase and 80 min after the last bolus, the patient described ptosis, myosis, and enophthalmos, without manifested anhidrosis. Motor deficit was not present; the sensory deficit rose to T3. The clinical presentation disappeared 130 min after detaining the perfusion.
Case 3
32-Year-old patient in her first gestation in induced labor at 41 weeks of gestation. 155 cm tall and 60 kg body weight. She had chronic arterial hypertension as an antecedent of interest. An initial bolus of 9 ml of ropivacain and fentanyl was administered, followed by a continuous perfusion of 8mlh-1. After 45 min, and due to risk of loss of fetal wellness, the decision was made to initiate an emergency cesarean section. For this, 9 ml of 2% lidocaine was administered. After the beginning of the cesarean section, a clinical presentation suggesting Horner syndrome was observed (see Fig. 1) only 15 min after the administration of the anesthetic bolus of lidocaine. No motor symptoms were reported. The sensory level reached metamere T2. After 95 min of observation, the clinical presentation disappeared without further measures.

After the clinical diagnosis from evidence of ptosis, myosis, enophthalmos, and anhidrosis, an neurological (sensory level and motor function) and cardiorespiratory (continuous monitoring of blood oxygen saturation with pulse oximetry, electrocardiography, and non-invasive blood pressure) exploration was initiated.
The perfusion of local anesthetic was detained in all the cases. None of the patients presented with cardiorespiratory complication, maintaining a heart rate of around 70 beats per minute, average blood pressure above 65 mm/hg, and blood oxygen saturation above 95% with no need for supplementary oxygen. The clinical presentation reversed in a variable time after perfusion was stopped.
There were no neonatal repercussions in any of the cases presented.
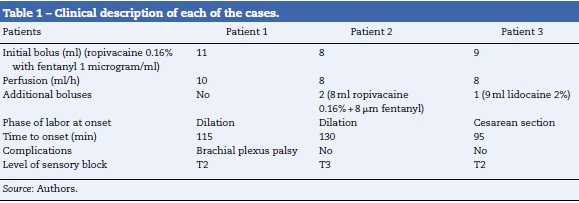
Table 1 summarizes the clinical characteristics of the patients.
Discussion
The clinical presentation of Horner syndrome is inconspicuous and can go unnoticed, with some authors affirming that it can go unobserved in 75% of births by cesarean section that use this anesthetic method.5 For the majority of our patients, the presentation was subtle with partial ptosis.
Multiple reasons have been described for explaining the physiopathology. The majority of authors agree that, for the syndrome to present, a cephalic spread of the local anesthetic is necessary, leading to an interruption of the sympathetic chain from C8 to T1 before entering the superior cervical ganglion. In gestating patients, a series of anatomical changes occur that favor the spread of the anesthetic to the upper levels: abdominal hyper-pressure from the gravid uterus, uterine contractions, and dilation of the epidural venous plexus that reduces such space. The higher sensitivity of the sympathetic fibers to the local anesthetic allows for their block while maintaining sensory and motor fibers. However, in some cases, like the one described above, it can be associated with brachial plexus palsy in a probable relationship with spread toward the subdural or subarachnoid space.8,9
There are anatomical variations that facilitate the ascension of local anesthetic, like the presence of fibrous septae in the epidural space, lumbar hyperlordosis, scoliosis, spondy-lolisthesis, post-surgical adhesions, and repeated epidural punctures. One of the patients presented with a noticeable lumbar hyperlordosis while the rest of the cases showed the normal anatomy of a pregnant woman.
Other theories that explain this phenomenon go beyond the changes that occur in the pregnant patient, arguing for an erroneous placement of the epidural catheter either in the subdural space or its paravertebral migration. The insertion of the catheter at the subdural level leads to the spread of the anesthetic to the subarachnoid space, leading to a sensory block that affects the more cephalic metameres for the volume and concentration used with a variable motor effect and even cardiorespiratory arrest.10 Due to the benign evolution, the subdural situation was not ruled out with radiology. It is probable that using multi-perforated catheters facilitates placement, albeit partially, in this space, since some orifices are at the epidural level and others at the subdural level.
The decubitus lateral position during puncture and the increase in sensitivity of pregnant patients to local anesthetics due to progesterone are other factors to take into account. All of the punctures in our patients were performed in a sitting position.
The anesthetic used does not seem to influence incidence, as in our series the syndrome appeared with both the administration of ropivacaine and lidocaine, although in the latter case, the latency and recovery times were considerably reduced. The repeated administration of the dose of local anesthetic can favor its cephalic spread. In two of the cases, additional boluses (i.e. apart from the initial one) were administered, one at the time of the cesarean section and the other during the dilation phase due to patient request (pain > 4 measured on the visual analog scale). One of the cases had the clinical presentation with continuous perfusion and without additional boluses. The volume of local anesthetic administered in the initial bolus was calculated at around 0.5-1 ml per metamere to be covered in function of the stage of labor.
The presentation of Horner syndrome is, in most cases, self-limiting and resolves itself in an average time of 215 min, with a relatively benign course.11 Generally, heart and respiratory stability is maintained, with maternal hypotension being infrequent. In the patients in our study, the clinical presentation disappeared in an average time of 113 min. All patients maintained cardiorespiratory stability.
However, despite their good evolution, the presence of the syndrome tells us of a sympathetic block that reaches thoracic levels with a potential risk of cardiorespiratory collapse. Therefore, surveillance of the patient is essential, especially if we opt to maintain the epidural catheter. With the least suspicion of an effect on the patient, the perfusion of local anesthetics should be withdrawn, and close monitoring of the maternal-fetal state should be performed.12 We opted for withdrawing the perfusion in those patients that presented with the syndrome in the dilation phase, evaluating the potential risk of maternal-fetal effects, as previously mentioned. The patient that suffered the episode during the cesarean section after the epidural bolus remained under close monitoring without complications in the recovery.
When this complication occurs, an exhaustive neurological exploration is recommended. Performing complementary tests is not recommended systematically; these are reserved for patients in which the clinical picture persists more than 12-24 h in order to rule out other causes (Pancoast tumor, carotid artery dissection).13,14
The majority of the series described in the literature are isolated cases.2-13 Few case series affecting multiple patients have been published.15 The main reason for this is probably the low degree of suspicion and the underdiagnosis of the syndrome-in other words, it has to be actively looked for. Despite its favorable prognosis, it can directly indicate a cephalic spread of local anesthetic to potentially dangerous levels. Therefore, observation and surveillance until the complete disappearance of the clinical presentation, along with suspension of perfusion of local anesthetic, are essential to its management.
Financing
The authors did not receive sponsorship to carry out this article.
Conflicts of interest
The authors have no conflicts of interest to declare.
References
1. Haslett C, Chilvers ER, Boon N. Davidsons principles and practice of medicine. 19th ed. Churchill Livingstone: Edinburgh; 2002. [ Links ]
2. Castilla Peinado G, Garcia Saura PL, Parrila Ruiz E, Hijona Elosegui JJ, Contreras Rodriguez A, Torres Marti JM. Sindrome de Horner despues de analgesia epidural para el trabajo de parto. Clin Invest Gin Obst. 2009;36:223-5. [ Links ]
3. Gonzalez Cárdenasa VH, Munar Gonzálezb F, Gómez Barajasc WJ, Cardonad AM, Roseroe BR, Manriquef AJ. Remifentanilo vs. analgesia epidural para el manejo del dolor agudo relacionado con el trabajo de parto. Revisión sistemática y meta-análisis. Rev Colomb Anestesiol. 2014;42: 281-94. [ Links ]
4. Tympa A, Grigoriadis C, Petropoulos G, Hassiakos D. Horner syndrome following bolus low dose epidural analgesia for labor. J Anesth. 2013;27:799-800. [ Links ]
5. Wong SY, Lin CF, Lo LM, Peng TC, Chuah EC. Postpartum unilateral Horner's syndrome following lumbar epidural anesthesia after a cesarean delivery. Chang Gung Med J. 2004;27:624-8. [ Links ]
6. Biousse V, Guevara RA, Newman NJ. Transient Horner's syndrome after lumbar epidural anesthesia. Neurology. 1998;51:1473-5. [ Links ]
7. Molins Ballabriga G, Vacas Y, Jiménez F, Borras J, Mailan R. Horner syndrome and brachial plexus blockade after epidural anesthesia for obstetric labor and cesarean section. Rev Esp Anestesiol Reanim. 2011;58:54-6. [ Links ]
8. Avellanosa J, Vera J, Morillas P, Gredilla E, Gilsanz F. Síndrome de Horner y bloqueo del plexo braquial ipsilateral en un caso de analgesia epidural para el trabajo de parto. Rev Soc Esp Dolor. 2006;13:481-4. [ Links ]
9. Jadon A. Horner's syndrome and weakness of upper limb after epidural anaesthesia for caesarean section. Indian J Anaesth. 2014;58:464-6. [ Links ]
10. De la Gala F, Reyes A, Avellanel M, Baticon F, Gonzalez-Zarco LM. Trigeminal nerve palsy and Horner's syndrome following epidural analgesia for labor: a subdural block? Int J Obstet Anesth. 2008;17:92-3. [ Links ]
11. Chauhan G, Nayar P, Kashyap C. Ipsilateral Horner's syndrome associated with epidural anesthesia in emergency cesarean section. J Obstet Anaesth Crit Care. 2012;2:112-3. [ Links ]
12. Al-Mustafa MM, Massad IM, Al-Ghanem SM, Badran IZ. Horner's syndrome after lumbar epidural analgesia during labor. Middle East J Anesthesiol. 2010;20:727-9. [ Links ]
13. Lynch JH, Keneally RJ, Hustead TR. Horner's syndrome and trigeminal nerve palsy following epidural analgesia for labor. J Am Board Fam Med. 2006;19:521-3. [ Links ]
14. Vidal M, Calderón E, Pernia A, Martínez J, Torres LM. Diagnóstico diferencial del síndrome de Horner en analgesia epidural obstétrica.¿Cuándo preocuparse? Rev Esp Anestesiol Reanim. 2005;52:57-8. [ Links ]
15. Rabinovich A, Abedelhady R, Mazor M, Piura B, Margolin E. Horner's syndrome following epidural analgesia during labor: report of six cases. Eur J Obstet Gynecol Reprod Biol. 2010;149:229–30. [ Links ]

