










Services on Demand
Journal
Article
 text in
text in  English (pdf)
English (pdf)
 Article in xml format
Article in xml format Article references
Article references
 Send this article by e-mail
Send this article by e-mailIndicators
-
 Cited by SciELO
Cited by SciELO -
 Access statistics
Access statistics
Related links
-
 Cited by Google
Cited by Google -
 Similars in
SciELO
Similars in
SciELO -
 Similars in Google
Similars in Google
Share

 Permalink
PermalinkColombian Journal of Anestesiology
Print version ISSN 0120-3347
Rev. colomb. anestesiol. vol.45 no.1 Bogotá Jan./June 2017
Are we meeting current recommendations for the initial management of penetrating trauma? A preliminary analysis from a Colombian institutional registry☆
¿Estamos logrando las recomendaciones actuales en trauma penetrante? Análisis preliminar de un registro institucional colombiano
Fredy Arizaa,*, Beatriz Elena Sáncheza, Alberto Federico Garcíab, Fernando Raffán-Sanabriac, Manuel Quintana-Díazd, Jorge Humberto Mejía-Mantillaa
a Anesthesiology and Perioperative Medicine - Fundación Valle del Lili, Cali, Colombia
b Trauma Surgery and Intensive Care, Fundación Valle del Lili, Cali, Colombia
c Department of Anesthesiology and Resuscitation, Fundación Santa Fé de Bogotá, Bogotá D.C., Colombia
d Emergency and Intensive Care Service, Hospital Universitario La Paz, Madrid, Spain
☆ Please cite this article as: Ariza F, Sánchez BE, García AF, Raffán-Sanabria F, Quintana-Díaz M, Mejía-Mantilla JH. ¿Estamos logrando las recomendaciones actuales en trauma penetrante? Análisis preliminar de un registro institucional colombiano. Rev Colomb Anestesiol. 2017;45:39-45.
* Corresponding author at: Fundación Valle del Lili, Av. Simón Bolívar, Carrera 98, No. 80-45, Cali, Colombia.
E-mail address: fredyariza@hotmail.com (F. Ariza).
Article history:
Received 22 October 2015 Accepted 26 September 2016 Available online 8 December 2016
Abstract
Introduction: To achieve minimal physiological goals in patients with penetrating thoracoabdominal trauma (TAPT) is essential to ensure adequate outcomes.
Objectives: To determine the success in meting basic standards at the end of damage control surgery in subjects with TAPT: (1) Monitoring and prevention of hyperfibrinolysis; (2) central temperature >35 °C; (3) platelet count >50,000/mm3 and serum fibrinogen >150mg/dl; (4) hemoglobin levels >7.5 mg/dl and base deficit <6.
Methods: Subjects >18 years old undergoing damage control surgery as a result of TAPT were prospectively collected at a referral center between October Oct-2012 and Dec-2014. Comparisons were done according to the Injury Severity Score (ISS) with a severity value indicator of >25. A p < 0.05 value was considered significant.
Results:106 subjects with TAPT were enrolled. Administration of tranexamic acid was only reported in 52.7% of the patients, particularly in the group with low severity scores [Group ISS < 25 36.3% vs. group ISS > 25 65.8%. OR 3.37 (95% CI 1.2-9.85); p = 0.01]. Although the temperature was reported in 91% of the cases, only 66.2-71.4% reached the recommended goal. Serum fibrinogen was measured in 59.5% of the cases and only 52% met the recommended level. The base deficit values of <6 at the end of surgery were only accomplished in 40-43.8% of the subjects, with a significantly lower probability in the more severe patients [53% vs. 35.9%. OR 2.04 (95% CI 1.2-6.02); p = 0.042].
Conclusions: A considerable proportion of patients with TAPT does not meet the current recommendations at the end of damage control surgery.
Keywords: Mortality, Tranexamic acid, Blood coagulation disorders, Multiple trauma, Abdomen.
Resumen
Introducción: El logro de metas fisiológicas mínimas en pacientes con trauma toracoabdominal penetrante (TTAP) es fundamental para garantizar adecuados desenlaces.
Objetivos: Determinar el éxito en el logro de estándares básicos al final de la cirugía de control de daños en sujetos con TTAP: 1.Monitorización y prevención de hiperfibrinolisis; 2.Temperatura central > 35 °C; 3.Niveles plaquetarios>50.000/mm3 y de fibrinógeno sérico > 150 mg/dl; 4.Niveles de hemoglobina > 7.5 mg/dl y déficit de base < 6.
Métodos: Se recolectaron prospectivamente sujetos > 18 años llevados a cirugía de control de daños por TTAP en un centro de remisión entre Oct-2012 y Dic-2014. Las comparaciones se realizaron según el Injury severity score (ISS) teniendo como indicador de severidad un valor >25. Se consideró significativo un valor de p < 0.05.
Resultados: Se registraron 106 sujetos con TTAP. La aplicación de ácido tranexámico solo se reportó en 52.7% de los pacientes, especialmente en el grupo con puntajes de severidad bajos [Grupo ISS<25 36.3% vs. grupo ISS > 25 65.8%. OR 3.37 (IC95% 1.2-9.85); p = 0.01]. A pesar de que la temperatura fue reportada en 91% de los casos, solo 66.2-71.4% alcanzaron la meta recomendada. El fibrinógeno sérico fue valorado en 59.5% de los sujetos y solo 52% alcanzaron la recomendación. Valores de déficit de base < 6 Al final de cirugía solo se lograron en 40-43.8% de los sujetos, con una probabilidad significativamente menor en los sujetos más graves [53% vs. 35.9%. OR 2.04 (IC95% 1.2-6.02); p = 0.042].
Conclusiones: Una proporción considerable de pacientes con TTAP no logran las recomendaciones actuales al final de la cirugía de control de daños.
Palabras clave: Mortalidad, Ácido tranexámico, Trastornos de la coagulación, sanguínea, Traumatísmo múltiple, Abdomen.
Introduction
Increasing incidence of major and high impact trauma makes it a world public health problem,1,2 resulting in a growing number of up-to-dates, new concepts and guidelines based on the best available evidence about the optimal use of pharmacological/non-pharmacological strategies and devices for physiological stabilization.3,4 Early recognition and treatment of shock and coagulopathy are cornerstones in this setting. There have been important advances in these concepts leading to more specific recommendations about markers of adequate hemostasis and microcirculation.5
Perioperative treatment of patients with severe trauma is quite heterogeneous among different institutions. This observation is even a fact among the healthcare providers within the same institution, in terms of the approach to the problem and the perception about the best therapeutic option for each situation, specially in the absence of institutional treatment guidelines to address this patients.6,7 Numerous publications recommend structuring a trauma team with clear objectives and the ability to define the role of each team member.
However, initial caregivers in the OR are exceptionally important, both in the accomplishment of these goals, as well in helping to reduce the rate of adverse outcomes and mortality.
This paper analyzed the achieving of the current recommendations8-10 by the surgical team of a referral center during the initial care of penetrating chest and/or abdomen trauma patients (TAPT) at the end of damage control surgery (DCS) globally and according to the severity of the injury based on the Injury Severity Score (ISS).11
Design and study population
An observational cohort study was performed based on a prospective trauma registry at a Colombian trauma referral center (CERATI registry - prospective Cohort study of Early Reintervention in Abdominal and Thoracic Penetrating Injuries) approved by the Committee of Ethics in Biomedical Research of the Fundación Valle del Lili (Protocol No. 635). Subjects 18 years or older requiring DCS due to TAPT within the first 24 hours after trauma occurrence or those who were admitted from other centers within 12 hours after initial treatment were prospectively enrolled. Patients admitted to the OR with no vital signs were excluded as well as those that did not survive to surgery; patients with a history of known hemostatic disorders and those who had been under systemic anticoagulation or platelet aggregation therapy.
In order to implement this registry, a centralized database (DB) was developed under a Web platform (BD-Clinic, CIC-FVL, Cali, Colombia) with controlled access by two of the authors (BS & FA) to data uploading and reading. Through continued education sessions directed to the anesthetists and surgeons involved with the registry, some suggested principles for basic care for transfusion therapy, resuscitation drugs, hemostasis control and active warming were previously established. Assessment of shock, anemia and coagulopathy at admission (first 15 mins of care) and at the end of DCS or admission to ICU was agreed and protocolized.
Once the patient was identified, data was registered on a previous designed form including demographic characteristics, severity of the lesions, information about the time of care and preoperative treatment provided, characteristics of the fluids used for resuscitation, blood products administered (type and amount), use of rapid infusion systems, red blood cells salvage and shock markers [lactic acid, base deficit (BD)], erythrocyte mass and platelet count, and hemostatic profile [Thromboelastography (TEG®), serum fibrinogen) at the beginning and end of the procedure. A previously trained and independent assistant monitored the patients every 8 h, either physically or reviewing the electronic medical record (SAP, Net Weaver GUI for Windows Business Software. Germany) and a laboratory reporting system (http://datalabfvlapl/consulta/default.aspx) during the first three days and then everyday for the first week. After that, a weekly follow-up was done either physically or by call up to 30 days after the DCS. Quarterly reports and quality controls were performed in order to verifying the proper conduct of this prospective registry.
Methods and variables
Information was classified into three universal categories: (1) assessment and prophylaxis of hyperfibrinolysis (intraoperative monitoring of serum fibrinogen and administration of tranexamic acid at any time during the procedure), (2) protection against hypothermia (achieving a central temperature of >35 °C at the end of surgery); (3) hemostatic resuscitation (serum fibrinogen levels of >150 mg/dl at the end surgery and a platelet count of >50,000/mm3); (4) microcirculation and reed blood cells count improvement at the end of surgery (proportion of subjects with BD > 6 and levels of hemoglobin >7.5 mg/dl).
Analysis plan
Information recorded in the DB was edited and inconsistent data were corrected upon matching against the medical and laboratory records. STATA 10.1 (StataCorp 4905 Lakeway Dr., Texas, USA) package was used to perform descriptive and analytical statistics according to the ISS score estimated at admission, determining a severity cut point value of >25.
Chi-square test was used for the analysis of categorical variables and Mann-Whitney test (two-sample Wilcoxon rank-sum test) for continuous ones. A sensitivity analysis was performed for potential values in individuals with some missing data. Results are expressed as frequencies for dichotomous variables and as means (interquartile ranges, ICR) for continuous ones given their non-parametric behavior. A p < 0.05 value was considered statistically significant.
Results
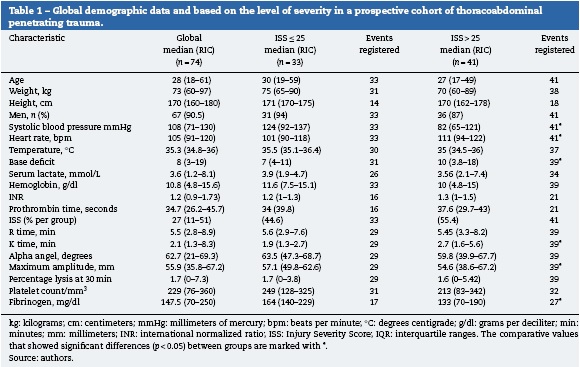
From 338 patients who underwent surgery due to any type of trauma during this period of time, 103 subjects were identified as TAPT. There were 16 (15%) cases of intraoperative death. Additionally, 13 subjects was retired from analysis due to data omissions and/or failure to obtain results from tests considered extremely important to perform statistical correlations. Hence, 74 TAPT patients admitted for DCS were included, all of them treated within three hours following the trauma event. 55.4% of the subjects studied presented penetrating injuries of a high grade of severity at admission (ISS > 25) (Table 1). Global mortality due to TAPT, including subjects who died before, during and after the DCS was 18%, while for the cohort that survived to the DCS the rate or reoperation due to bleeding was 2.7% with an accumulated mortality of 4%. All of these patients died within the first 24 postoperative hours (Table 2).
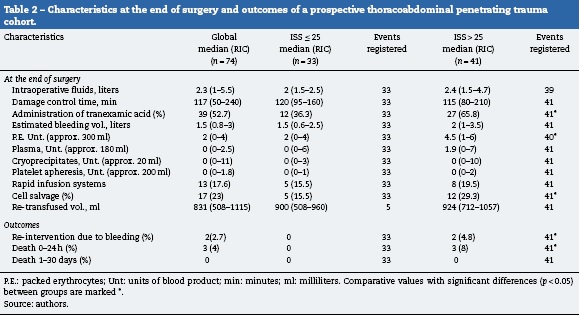
When comparing the group with severe lesions (ISS > 25; n = 41) against the subjects with lower severity scores (ISS < 25; n = 33), there were significant differences in heart rate and systolic blood pressure measurements at admission [111 (94-122) vs. 101 (90-108) bpm, p = 0.048 and 82 (65-121) vs. 124 (92-137) mmHg, p = 0.002; respectively]. The analysis of some of the conventional diagnostic tests at the start of surgery showed statistically significant differences in the BD and serum fibrinogen levels [10 (3.8-18) vs. 7 (4-11), p = 0.005 and 133 (70-190) vs. 164 (140-229) mg/dl, p = 0.023; respectively]. Based on the thromboelastographic parameters at the start of the DCS, only K time and maximum amplitude (MA) were significantly correlated with the presence of critical lesions [2.7 (1.6-5.6) vs. 1.9 (1.3-2.7) min, p = 0.006 and 54.6 (38.6-67.2) vs. 57.1 mm (49.8-62.6) min, p = 0.042; respectively].
Overall, the use of tranesxamic acid at any time during the DCS was only reported in 52.7% of the patients with a significantly lower adherence in patients with low severity scores [65.8% vs. 36.3%. OR 3.37 (95% CI 1.2-9.85); p = 0.01]. Furthermore, fibrinogen monitoring at the start of surgery was only evaluated in 59.5% of the cases, with no significant differences between groups [65.8% vs. 51%. OR 1.05 (0.40-2.7); p = 0.89].
Despite temperature monitoring was reported in 91% of cases, only 66.2-71.4% reached values above 35 °C at the end of procedure, with no significant differences between groups [Group ISS > 25 61% vs. Group ISS < 25 72.7%. OR 1.7 (95% CI 0.57-5.25); p = 0.28] (Fig. 1). Up to 90-91.8% of the cases reached hemoglobin levels of >7.5 g/dl with no differences between groups (90.9% vs. 92.6%). However, when analyzing perfusion markers at the end of surgery, only 40-43.4% of the subjects reached values of BD < 6 overall, with a significant trend to reach lower levels in the group with high severity scores [35.9% vs. 53%. OR 2.04 (1.2-6.02); p = 0.042].
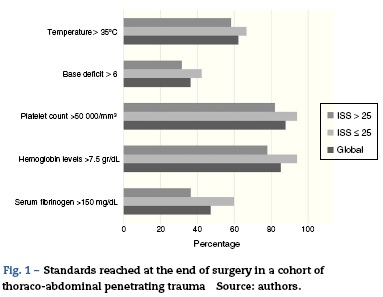
Between 91-94.5% of the subjects included in this analysis reached platelet levels of >50,000/mm3 at the end of DCS (Group ISS>25 87.1% vs. Group ISS ≤ 25 96%). In contrast, for the case of serum fibrinogen at the end of surgery (reported in 74.3% of the subjects), levels of >150 mg/dl were only reached in 52-55% overall, with a non-significant low rate in the group with more severe lesions [41.4% vs. 60.6%. OR 2.17 (95% CI 0.77-6.15); p = 0.1]. Sensitivity analysis showed that in the best of the cases, mínimum accepted levels of temperature and serum fibrinogen at the end of DCS was reached only in 72% and 65%, respectively.
Discussion
This safety analysis focused in patients with penetrating injuries is part of an institutional multidisciplinary effort to improve care results in these patients. This prospective registry was performed at a referral university center that continuously schedules multidisciplinary sessions and promotes a constant effort to assure availability of technologies for the care and diagnosis of specific situations for the treatment of severe trauma patients. There is enough evidence to support early monitoring and control of bleeding in patients with exsanguinating trauma as a determinant of the outcomes associated with morbidity and mortality.12,13 However, our study shows that a high rate of TAPT patients are in risk of not to meet the current recommendations on resuscitation, temperature preservation and management of hemostasis.
Our data show expected differences in terms of blood pressure values, heart rate and BD between patients with higher severity scores.14,15 However, despite an observed high proportion of severe injuries in our study, we found that adherence to recommended strategies aimed at reducing major bleeding during DCS was unacceptably low, as shown in the reported rate of administration of tranexamic acid, which was only administer to a little more than a half of the subjects, despite scientific evidence endorsingits use.16,17 Achievement of thermoprotection goal shows a similar trend; despite the availability of active warming technologies such as warming console guided systems and forced air blankets, and of the awareness about hypothermia-related derangements in hemostasis, inflammation and tissue perfusion in severely injured patients,7,18,19 one third of the subjects failed to reach this goal at the end of surgery.
This study also showed a broad heterogeneity in monitoring and intraoperative recovery of microcirculation approaches during massive bleeding and trauma. Newgard et al. showed that at least one third of trauma patients could present hemodynamic instability at the time of admission.20 In this regard, we aimed to analyse the quality of resuscitative strategies in this cohort through results of a recognized marker for hypovolemic shock such as BD which has been described to be as useful as serum lactate measurements in this scenario.21,22 In a retrospective cohort of 1026 trauma patients, BD showed a high predictive value for death, particularly during the first 24 hours after injury.23 Our study shows a poor success rate to achieve optimal levels of this microcirculatory surrogate, despite a high rate of success in correction of anemia. This observation may represent the need for studies that analyze microcirculation within the context of trauma and an opportunity to develop hospital care guidelines promoting early evaluation and the adequate use of fluid therapy strategies and goal-directed hemostatic resuscitation.24,25
We want to highlight the importance of assessment of fibrinogen as a factor independently associated to severity in major trauma.26-28 Our study shows a low proportion of subjects with an assessment of this so important substrate for hemostasis that could be explained at least in part by the limitations to obtain a quick result of the test. The usefulness of viscoelastic testing (TEG, ROTEM) and their predictive value are still a topic for debate due to the quality of the available evidence and non-conclusive results of recent reviews, despite our results ratify the association between thromboelastography components (K time and MA), fibrinogen levels and severity of injury reported in previous studies.29-31 Point of care fibrinogen assays have been recently developed and we think these technologies may be the future solution to current limitations to a timely assessment that could be associated with delayed recovery, particularly where only conventional tests for evaluating hemostasis are available.32,33
During the study period, the use of tranexamic acid (usual dose of 1 g IV, whether or not followed by a continuous IV infusion of 1 g/6 h) was maintained as a consensus in all severe trauma patients requiring DCS, based on a clinical trial that reported a significant association between this drug and an overall reduction in the incidence of death from all causes in this subpopulation.14 Very few studies on specific interventions in trauma have shown a significant change in this "hard" outcome. As described in a recent update of the European guidelines for care of severe bleeding and coagulopathy associated with severe trauma, we feel that the use of tranexamic acid within the first three hours is an important indicator of compliance with the current standards in trauma care associated with severe bleeding, that should be further evaluated for future studies.34
The significant heterogeneity observed in this study also included a large variability in the transfusion patterns reported. This observation is similar to findings of a recent study that reported a wide range of approaches resulting in a broad variation in the proportions of blood components used without an established pattern, even under controlled research settings.35 This situation may in part explain the low percentage of patients with fibrinogen targets above the current recommendation. However, we believe that this heterogenity may originate from a flaw in the continuous education processes that overcome the barriers of basic knowledge and the absence of specific trauma protocols that may integrate transfusional strategies with the other mainstays of therapy in this context.
We think this prospective registry has important limitations. Mortality rate may be affected by not including subjects that were admitted but died during DCS and influenced potential associations that we were unable to identify or overestimated others. In spite of the fact that a proportion of patients (12%) had to be excluded from analysis because missing data, we think that the sample analyzed is a good representative of this problem, showing a wide variability in achieving the goals, despite having enough human resources and availability of resources for high quality care, at least at the center where this registry was developed. Further trials that confirm our results are required, since if these are true, it will be necessary to adopt an urgent action plan for hospitals and scientific societies around the world.
In conclusion, this study suggests that currently a considerable proportion of penetrating trauma patients do not achieve the current minimum recommendations at the end of DCS. There is wide variability in assessment and interventional approaches related to resuscitative and hemostatic issues that affect early detection of independent markers for morbidity and mortality in this subpopulation. Institutions require not only to be focused toward getting resources and technologies for the attention of severe trauma, but also to optimize these resources through continuous education programs and institutional protocols to ensure a high level of compliance and adherence to recommendations.
Ethical disclosures
Protection of human and animal subjects. The authors declare that the procedures followed were in accordance with the regulations of the relevant clinical research ethics committee and with those of the Code of Ethics of the World Medical Association (Declaration of Helsinki).
Confidentiality of data. The authors declare that they have fol-lowed the protocols of their work center on the publication of patient data.
Right to privacy and informed consent. The authors declare that no patient data appear in this article.
Conflicts of interest
The authors have no conflicts of interest to declare.
Funding
The authors' resources.
References
1. Murray CJ, Lopez AD. Alternative projections of mortality and disability by cause 1990-2020: Global Burden of Disease Study. Lancet. 1997;349:1498-504. [ Links ]
2. Cause-specific mortality and morbidity. World Health Organization; 2009. p. 47-57. Available from: http://www.who.int/whosis/whostat/EN_WHS09_Table2.pdf. [ Links ]
3. Sørensen B, Larsen OH, Rea CJ, Tang M, Foley JH, Fenger-Eriksen C. Fibrinogen as a hemostatic agent. Semin Thromb Hemost. 2012;38:268-73. [ Links ]
4. Wang HE, Callaway CW, Peitzman AB, Tisherman SA. Admission hypothermia and outcome after major trauma. Crit Care Med. 2005;33:1296-301. [ Links ]
5. Spivey M, Parr MJ. Therapeutic approaches in trauma-induced coagulopathy. Minerva Anestesiol. 2005;71:281-9. [ Links ]
6. Hoyt DB, Bulger EM, Knudson MM, Morris J, Ierardi R, Sugerman HJ, et al. Death in the operating room: an analysis of a multi-center experience. J Trauma. 1994;37:426-32. [ Links ]
7. Curry N, Stanworth S, Hopewell S, Dorée C, Brohi K, Hyde C. Trauma-induced coagulopathy-a review of the systematic reviews: is there sufficient evidence to guide clinical transfusion practice? Transfus Med Rev. 2011;25:217-31, e2. [ Links ]
8. Egea-Guerrero JJ, Freire-Aragón MD, Serrano-Lázaro A, Quintana-Díaz M, Grupo de Trabajo de Trauma y Neurointensivismo de SEMICYUC. Resuscitative goals and new strategies in severe trauma patient resuscitation. Med Intensiva. 2014;38:502-12. [ Links ]
9. Schöchl H, Grassetto A, Schlimp CJ. Management of hemorrhage in trauma. J Cardiothorac Vasc Anesth. 2013;27 Suppl:S35-43. [ Links ]
10. Spahn DR. TEG®- or ROTEM®-based individualized goal-directed coagulation algorithms: don't wait-act now! Crit Care. 2014;18:637. [ Links ]
11. Baker SP, O'Neill B, Haddon W Jr, Long WB. The injury severity score: a method for describing patients with multiple injuries and evaluating emergency care. J Trauma. 1974;14:187-96. [ Links ]
12. Gillman LM, Ball CG, Panebianco N, Al-Kadi A, Kirkpatrick AW. Clinician performed resuscitative ultrasonography for the initial evaluation and resuscitation of trauma. Scand J Trauma Resusc Emerg Med. 2009;17:34. [ Links ]
13. Johnson JW, Gracias VH, Schwab CW, Reilly PM, Kauder DR, Shapiro MB, et al. Evolution in damage control for exsanguinating penetrating abdominal injury. J Trauma. 2001;51:261-9, discussion 269-71. [ Links ]
14. Nunez TC, Voskresensky IV, Dossett LA, Shinall R, Dutton WD, Cotton BA. Early prediction of massive transfusion in trauma: simple as ABC (assessment of blood consumption)? J Trauma. 2009;66:346-52. [ Links ]
15. Mitra B, Rainer TH, Cameron PA. Predicting massive blood transfusion using clinical scores post-trauma. Vox Sang. 2012;102:324-30. [ Links ]
16. CRASH-2 trial collaboratorsShakur H, Roberts I, Bautista R, Caballero J, Coats T, et al. Effects of tranexamic acid on death, vascular occlusive events, and blood transfusion in trauma patients with significant haemorrhage (CRASH-2): a randomised, placebo-controlled trial. Lancet. 2010;376:23-32. [ Links ]
17. Sihler KC, Napolitano LM. Massive transfusion: new insights. Chest. 2009;136:1654-67. [ Links ]
18. Kutcher ME, Howard BM, Sperry JL, Hubbard AE, Decker AL, Cuschieri J, et al. Evolving beyond the vicious triad: differential mediation of traumatic coagulopathy by injury, shock, and resuscitation. J Trauma Acut Care Surg. 2015;78:516-23. [ Links ]
19. Simmons JW, Pittet JF, Pierce B. Trauma-induced coagulopathy. Curr Anesthesiol Rep. 2014;4:189-99. [ Links ]
20. Newgard CD, Meier EN, McKnight B, Drennan IR, Richardson D, Brasel K, et al. Understanding traumatic shock: out-of-hospital hypotension with and without other physiologic compromise. J Trauma Acute Care Surg. 2015;78:342-51. [ Links ]
21. Dunne JR, Tracy JK, Scalea TM, Napolitano LM. Lactate and base deficit in trauma: does alcohol or drug use impair their predictive accuracy? J Trauma. 2005;58:959-66. [ Links ]
22. Cheddie S, Muckart DJJ, Hardcastle TC. Base deficit as an early marker of coagulopathy in trauma. S Afr J Surg. 2013;51:88-90. [ Links ]
23. Martin MJ, FitzSullivan E, Salim A, Brown CVR, Demetriades D, Long W.Discordance between lactate and base deficit in the surgical intensive care unit: which one do you trust? Am J Surg. 2006;191:625-30. [ Links ]
24. Polderman KH, Varon J. Do not drown the patient: appropriate fluid management in critical illness. Am J Emerg Med. 2015;33:448-50. [ Links ]
25. Dutton RP. Management of traumatic haemorrhage-the US perspective. Anaesthesia. 2015;70 Suppl 1:108-11, e38. [ Links ]
26. Levy JH, Goodnough LT. How I use fibrinogen replacement therapy in acquired bleeding. Blood. 2015;125:1387-93. [ Links ]
27. Moore HB, Moore EE, Gonzalez E, Chapman MP, Chin TL, Silliman CC, et al. Hyperfibrinolysis, physiologic fibrinolysis, and fibrinolysis shutdown: the spectrum of postinjury fibrinolysis and relevance to antifibrinolytic therapy. J Trauma Acute Care Surg. 2014;77:811-7, discussion 817. [ Links ]
28. González Cárdenas VH. Transfusión en trauma. Rev Colomb Anestesiol. 2012;40:287-92. [ Links ]
29. Müller MCA, Balvers K, Binnekade JM, Curry N, Stanworth S, Gaarder C, et al. Thromboelastometry an organ failure in trauma patients: a prospective cohort study. Crit Care. 2014;18:687. [ Links ]
30. Hunt H, Stanworth S, Curry N, Woolley T, Cooper C, Ukoumunne O, et al. Thromboelastography (TEG) and rotational thromboelastometry (ROTEM) for trauma induced coagulopathy in adult trauma patients with bleeding. Cochrane Database Syst Rev. 2015:CD010438. [ Links ]
31. Da Luz LT, Nascimento B, Shankarakutty AK, Rizoli S, Adhikari NK. Effect of thromboelastography (TEG ) and rotational thromboelastometry (ROTEM ) on diagnosis of coagulopathy, transfusion guidance and mortality in trauma: descriptive systematic review. Crit Care. 2014;18:518. [ Links ]
32. Schlimp CJ, Khadem A, Klotz A, Solomon C, Hochleitner G, Ponschab M, et al. Rapid measurement of fibrinogen concentration in whole blood using a steel ball coagulometer. J Trauma Acute Care Surg. 2015;78:830-6. [ Links ]
33. Ogawa S, Tanaka KA, Nakajima Y, Nakayama Y, Takeshita J, Arai M, et al. Fibrinogen measurements in plasma and whole blood: a performance evaluation study of the dry-hematology system. Anesth Analg. 2015;120:18-25. [ Links ]
34. Rossaint R, Bouillon B, Cerny V, Coats TJ, Duranteau J, Fernández-Mondéjar E, et al. The European guideline on management of major bleeding and coagulopathy following trauma: fourth edition. Crit Care. 2016;20:100. [ Links ]
35. Holcomb JB, del Junco DJ, Fox EE, Wade CE, Cohen MJ, Schreiber MA, et al. The prospective, observational, multicenter, major trauma transfusion (PROMMTT) study: comparative effectiveness of a time-varying treatment with competing risks. JAMA Surg. 2013;148:127-36. [ Links ]

