











 text in
text in  English (pdf)
English (pdf)
 Article in xml format
Article in xml format Article references
Article references
 Send this article by e-mail
Send this article by e-mail Cited by SciELO
Cited by SciELO  Cited by Google
Cited by Google  Similars in
SciELO
Similars in
SciELO  Similars in Google
Similars in Google 
 Permalink
PermalinkIntroduction
Medical malpractice claims are the mechanism afforded to citizens to resort to a jurisdiction or to the administrative authorities in case of feeling violated their rights in the context of a performance of a health professional. In Colombia, there are different types of medical malpractice claims: ethical, criminal, civil, administrative, and disciplinary.1
Ethical cases are brought before courts integrated by members of the profession of the defendant in accordance with Law 23 of 1981.2 Criminal and civil cases are brought before a judge. In criminal cases, there is a formal indictment by the Fiscalía General de la Nación against the physician on the grounds of a violation against a protected legal right. In civil cases, the lawsuit seeks to obtain monetary remedies from an individual or by an insurance company to cover the damage suffered by the victim. Administrative proceedings are those in which a lawsuit is brought against public healthcare institutions together with the physician directly; or where the physician is brought in as guarantor by the institution; or where the institution initiates a repetition action against the practitioner.3 Similar to civil proceedings, administrative proceedings also aim for monetary remedies but, additionally, the remedy must come from the State, because of the involvement of a public institution. Finally, disciplinary proceedings are initiated by the institution against the physician because of the breach of its functions.4
Medical malpractice claims have become a problem for health systems because of their increased frequency and cost, affecting all actors in the healthcare system over the past 3 decades in most countries in the world.1,5,6 This increase in medical malpractice claims has had an impact on physicians in many ways: higher medical practice insurance cost affecting their economic productivity;7 impact on the physical and mental health of the prosecuted practitioner, known as the "second victim phenomenon";8,9 and the practice of defensive medicine that results in paraclinical tests being ordered just for legal reasons, or failure to perform optional treatments for the same reason.7
Factors that have been associated with a higher risk of becoming involved in a lawsuit are: the medical special-ty,10 where obstetrics is described as one of the specialties with a highest risk of receiving malpractice suits1,11-14; the type of harm caused to the patient; and poor performance, among others.15 Regarding the source of the claim, Cohen and Schifrin16 states that most claim in obstetrics are related to labor. About the care provided, delays in diagnosis and communication issues between the medical team and the patient have been reported as the most frequent claims.17,18
Knowledge regarding the characteristics of medical malpractice claims, their causes and the consequences for the practitioner and the health system comes mainly from developed countries,16,19,20 where Common law prevails most often and where medical liability cases converge with malpractice proceedings,21 similar to what happens in civil proceedings in the Colombian context. A detailed characterization of the proceedings in accordance with the particular circumstances of the local context is considered relevant so that all stakeholders (practitioners, attorneys, and decision-makers) can have a more thorough knowledge of this problem. Consequently, the objective of this study is to give a detailed description of the characteristics of obstetric medical malpractice claims in Colombia from the perspectives of physicians, patients, institutions, medical care provided, and the legal proceedings.
Methodology
Design
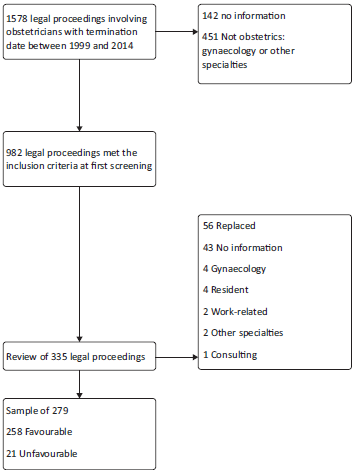
Descriptive historical cohort consisting of closed medical malpractice suits during the time period between 1999 and 2014, filed against obstetricians affiliated to the Fondo Especial para Auxilio Solidario de Demandas (FEPASDE), benefit provided by the Colombian Society of Anaesthesia and Resuscitation [Sociedad Colombiana de Anestesiología y Reanimación (S.C.A.R.E.)] nationwide. Lawsuits filed due to actions not related to direct care to a patient, cases related to gynecological care, or cases with no clinical information were excluded. A simple random sampling was made from a universe of 982 closed cases during the time period, based on an estimated 50% frequency for the type of ethical case, and a margin of error of 5%, for a required sample size of 279 lawsuits.
Description of the procedure
Cases that met the inclusion criteria were identified in the FEPASDE database. Sampling was performed using the negative coordinated method,22 replacing the cases that did not meet the selection criteria on physical document review. An information collection form was designed for gathering information about the institution, the practitioner, the proceeding, and the patient. Two trained medical professionals gathered the data from the different sources of information.
Variables
Procedures. Type of medical malpractice claims, duration, plaintiff, or person filing the suit; judicial decision, defined as favorable if it favored the practitioner (judgment for the defendant, file closed, judgment decline unlinking action, lawsuit inadmissibility, revocation of guarantor inclusion, or falls under the statute of limitations); or defined as unfavorable if the final judicial decision included any of the following: default judgment, admonishment, sanction with fine, settlement, indemnity payment, or sanction.
Institution-related. Type (public or private); geographic location defined as big city (more than 1 million inhabitants), intermediate city (more than 200,000 inhabitants); and rural location (less than 200,000 inhabitants).
Obstetrician-related. Age, gender, additional cases under FEPASDE coverage.
Patient-related and care-related. Age of the patient, place of origin, affiliation to the general social security system, date and time of admission, delivery route, gestational age, weight of the neonate, final diagnosis, and grounds for legal action.
Statistical analysis
The final database was consolidated using the STATA 13.1 License 301306295291 software package. A descriptive analysis of the information was performed. Categorical variables were described as absolute and relative frequencies, and quantitative variables as central trend and scatter, depending on data distribution assessed using the Shapiro-Wilk test (P <0.05). A bivariate analysis was performed by type of case for total frequency, frequency of judicial decisions, type of institution, and duration of the proceedings.
Results
Overall, 1578 candidate legal proceedings were reviewed and, of those, 982 met the inclusion criteria. Among these, 907 favorable cases and 75 unfavorable cases (7.7%) were identified. Of the initial sample of 279 cases, 56 did not meet the criteria and were replaced (Fig. 1).
The most frequent legal proceedings were ethical (44.4%) and criminal (36.6%). Legal proceedings were more frequent in intermediate cities (47.1%) and in private institutions (60.1%). In 77 cases (27.6%), there was involvement of more than 1 obstetrician. In 12.1% of the cases, association was found with a different lawsuit against the same obstetrician, more frequently ethical cases associated with criminal cases. Male sex was predominant (76%). Median age of male obstetricians at the time of the clinical event was 42 years (IQR: 28-64, minimum 23 years, maximum 72); and the median age of female obstetricians was 37 (IQR: 30-52, minimum 25 years, maximum 60). Among obstetricians, 42.4% had more than 1 lawsuit due to clinical events affecting other patients; 40.3% for female obstetricians, and 43.2% for male obstetricians (Tables 1 and 2).
Table 1 Characteristics of the lawsuits represented by FEPASDE (S.C.A.R.E.) Colombia, 1999-2014.
| Characteristics | Total cohort n (%) | Male obstetricians (n = 212) | Female obstetricians (n=67) |
| Of the procedures (n = 279) | |||
| Duration of the legal proceeding (IQR) years | 3.0 (1.5-5.0) | 3.0 (2.0-5.0) | 3.0 (1.5-1.0) |
| Type of case | |||
| Ethics | 124 (44.4) | 89 (42.0) | 35 (52.2) |
| Criminal | 102 (36.6) | 85 (40.1) | 17 (25.4) |
| Civil | 22 (7.9) | 15 (7.1) | 7 (10.5) |
| Administrative | 19 (6.8) | 15 (7.1) | 4 (6.0) |
| Disciplinary | 12 (4.3) | 8 (3.8) | 4 (6.0) |
| Plaintiff | |||
| Patient | 151 (55.9) | 108 (52.7) | 43 (66.2) |
| Partner | 65 (24.0) | 53 (25.9) | 12 (18.5) |
| Relative | 25 (9.3) | 22 (10.7) | 3 (4.6) |
| Official | 27 (10.1) | 21 (10.2) | 6 (9.2) |
| More than 1 obstetrician involved | 77 (27.6) | 57 (26.9) | 20 (29.9) |
| Institution (n = 278) | |||
| Location | |||
| Big city | 119 (42.8) | 84 (39.8) | 35 (52.2) |
| Intermediate city | 131 (47.1) | 102 (48.3) | 29 (43.3) |
| Rural township | 28 (10.1) | 3 (4.5) | 25 (11.9) |
| Type of institution (private) | 167 (60.1) | 128 (60.7) | 39 (58.3) |
| Obstetrician (n=279) | |||
| Obstetrician age Median (IQR) years | 41 (36-8) | 42 (28-64) | 37 (30-52) |
S.C.A.R.E. = Sociedad Colombiana de Anestesiología y Reanimación. IQR=Interquartile Range.
Source: Authors.
Table 2 Characterization by type of lawsuit, of cases represented by (S.C.A.R.E.) Colombia, 1999-2014.
| Ethics (n = 124) | Criminal (n = 102) | Civil (n = 22) | Administrative/disciplinary (n = 31) | |
| Characteristic | n (%) | n (%) | n (%) | n (%) |
| Unfavorable judicial decision | 9 (7.3) | 2 (1.9) | 7 (31.8) | 3 (9.6) |
| Location | ||||
| Big city | 57 (46.0) | 40 (39.2) | 12 (54.5) | 10 (32.3) |
| Intermediate city | 52 (41.9) | 53 (52.0) | 10 (45.5) | 16 (51.6) |
| Type of institution (public) | 51 (41.1) | 35 (34.3) | 2 (9.1) | 23 (74.2) |
| Duration Median (IQR) years | 2.6 (1.5-4.0) | 4.0 (2.0-6.0) | 3.5 (1.5-4.0) | 4.0 (2.0-7.0) |
| Falls under the statute of limitations | 37 (29.8) | 61 (59.8) | 0 (0) | 0(0) |
| Compensation | 0 (0.0) | 2 (2.0) | 8 (36.4) | 4 (12.9) |
| More than 1 gynecologist involved | 35 (28.2) | 22 (21.6) | 7 (31.8) | 13 (41.9) |
| Regime (contributive) | 72 (58.1) | 63 (61.8) | 17 (77.3) | 13 (41.9) |
S.C.A.R.E. = Sociedad Colombiana de Anestesiología y Reanimación.
IQR = Interquartile Range.
Source: Authors.
Patient characteristics
Overall, 264 patients were identified, resulting in 279 lawsuits; 15 patients were involved in 2 legal proceedings and 2 were involved in 3 legal proceedings. Mean age of the patients was 27 years and the majority belonged to the contributive health regime (63.7%) (Table 3).
Table 3 Characteristics of the patients and of the care provided in cases represented by FEPASDE (S.C.A.R.E.), Colombia, 1999-2014.
| Total | Male obstetricians (n = 212) | Female obstetricians (n = 67) | |
| Characteristic | n (%) | n (%) | n (%) |
| Age Median (IQR) | 27 (23-32) | 27 (23-32) | 28.5 (23.5-33) |
| Gestational age Median (IQR) weeks | 38 (34^0) | 38 (33-10) | 39 (36-39) |
| Social security | |||
| Contributive | 165 (63.7) | 127 (64.5) | 38 (61.3) |
| Subsidized | 58 (22.4) | 47 (23.9) | 11 (17.7) |
| Affiliated individual | 24 (9.3) | 15 (7.6) | 9 (14.5) |
| Private or other | 12 (4.6) | 8 (4.1) | 4 (4.5) |
| Neonatal diagnosis | |||
| Miscarriage | 30 (10.8) | 26 (12.3) | 4 (6.1) |
| Demise | 69 (24.9) | 47 (22.2) | 22 (33.3) |
| Live birth | 165 (59.6) | 130 (61.6) | 35 (53.0) |
| Not applicable | 13 (4.7) | 8 (3.8) | 5 (7.6) |
| Neonatal weight Median (IQR) gm | 3115 (2660-3500) | 3115 (2670-3500) | 3090 (2620-3570) |
| Cesarean delivery | 139 (60.4) | 106 (61.3) | 33 (57.9) |
| Readmission to delivery room after partum | 18 (19.8) | 13 (19.4) | 5 (20.8) |
| Readmission to delivery room after cesarean | 37 (26.6) | 30 (28.3) | 7 (21.2) |
| Length of stay Median (IQR) days | 2 (1^) | 2 (1-4) | 1 (0-3) |
| Maternal diagnosis at discharge | |||
| Improvement | 215 (77.1) | 161 (77.0) | 54 (80.6) |
| Referral | 31 (11.1) | 24 (11.5) | 7 (10.5) |
| Death | 30 (10.8) | 24 (11.5) | 6 (9.0) |
S.C.A.R.E. = Sociedad Colombiana de Anestesiología y Reanimación.
IQR = Interquartile Range.
Source: Authors.
In terms of comorbidities, 4.2% of the patients had a multiple gestation, 7 had pregnancy-related hypertensive disorders and 3 more had carbohydrate metabolism disorders; a total of 26 patients (10%) were older than 35.
Care characteristics
In 12 of the cases (4.3%), there was no underlying compromise to the mother or the neonate, and the main complaint was dissatisfaction with the care provided. In 39 of the pregnant women (14.8%), the triggering event of the legal proceedings took place before 24 weeks of gestation, and 30 (81%) were miscarriage cases. In 21 of the women (56.4%), the event was maternal compromise: 7 maternal deaths and 14 events that created some form of compromise (permanent or transient disability, traumatic injury, infection, readmission to the operating room, or admission to the intensive care unit).
A total of 225 patients (85.2%) had 24 weeks of gestation or more; in 60.4% of these patients, the route of delivery was cesarean section and, of these, 28.1% required readmission to the operating room, versus 19.8% readmission in the cases of vaginal deliveries. In 209 patients (74.7%), the legal proceedings were related to events occurring during delivery. Fetal/neonatal compromise was found in 158 of the lawsuits (56.6%): 69 fetal demises, 34 neonatal deaths and 55 neonates with some form of compromise (permanent or transient disability, traumatic injury, or hypoxic-ischemic injury, infection, or need for advanced vital support in the intensive care unit) (Table 3).
Discussion
The present study found a 7.7% frequency of unfavorable judicial decisions for the obstetrics specialty. The findings highlight that the most frequent actions filed in Colombia are of an ethical nature, followed by criminal actions. The highest proportion of unfavorable judicial decisions was found in civil proceedings. Legal proceedings were brought more frequently against private institutions, and the most frequent cause of the claims is neonatal compromise. Finally, the majority of the lawsuits are associated with patients in the third trimester with no risk factors or comorbidities.
The proportion of ethical cases found in our study (44%) was higher than the 20% described by López Ordoñez et al1 in cases related to all the specialties. These data emphasize a slow increase in the proportion of ethical cases over the past 2 decades.
In the Common law system, the percentage of unfavorable judicial decision ranges between 25% and 60%,19,20,23 similar to our findings for civil proceedings (31.8%), the only type of action comparable with the common law system.
The high frequency of legal actions against private institutions and patients affiliated to the contributive regime suggest that lawsuits are mainly filed by patients of a higher income level. This is so because of the relationship between the contributive regime and higher socioeconomic brackets;24 this in turn could be related to a higher degree of empowerment in terms of health rights and a higher degree of dissatisfaction when medical care leads to unfavorable judicial decision.7
Our results showing 74.7% of lawsuits related to care during childbirth are consistent with the postulate by Cohen and Schifrin16 who state that the majority of legal actions in obstetrics are directly or indirectly related to care during childbirth and report, for the United States, 60% of lawsuits associated with delivery care. Other authors like Gomez-Duran et al23 report a similar percentage (53.5%) for Spain.
Along the same lines, our study found a high frequency of lawsuits involving fetal (24.7%) or neonatal (38.9%) compromise, similar to what was reported by authors like Hale13, who describes that the 3 primary causes of lawsuits in obstetrics in the United States are neonatal injuries: neurological damage, death, and other types of injuries; and Domingues et al25 who reports that the 2 primary causes of obstetric lawsuits in Portugal are perinatal asphyxia and traumatic injuries to the neonate.
The limitations of the study relate to the quality of the information considering that data were collected retrospectively, and considering also that 16% of data had to be replaced in the sampling because of quality issues, which could have resulted in a selection bias. However, when comparing the results for gender and unfavorable judicial decisions in the total cohort in relation to the sample, the deviation was minimal (77% of male obstetricians in the cohort versus 76% in the sample); and the proportion of unfavorable judicial decisions between the cohort and the sample was also equal (7%). Additionally, the observer was not blinded to the favorable or unfavorable judicial decisions of the case, which could have created a measurement bias.
Strengths of the study include the high number of cases included in the cohort, which were reviewed in detail, long-term follow-up to the cases, and the geographic heterogeneity of the cases coming from all the regions of the country.
Conclusion
For the obstetrics specialty, the frequency of unfavorable judicial decisions is 7.7%. Ethical lawsuits are the most frequent, and unfavorable judicial decisions are most frequent in civil proceedings. Legal claims are brought most frequently against private institutions. Lawsuits occur mainly in association with patients in the third trimester of gestation who have no risk factors or comorbidities. Care during childbirth, and fetal and neonatal mortality are critical areas in medical malpractice claims, and they should be the focus of future research into care deficiencies and interventions aimed at minimizing the impact of legal action on the practitioners and the health system.
Ethical disclosures
Protection of human and animal subjects. The authors declare that no experiments were performed on humans or animals for this study.
Confidentiality of data. The authors declare that they have followed the protocols of their work center on the publication of patient data.
Right to privacy and informed consent. The authors declare that no patient data appear in this article.

