











 text in
text in  English (pdf)
English (pdf)
 Article in xml format
Article in xml format Article references
Article references
 Send this article by e-mail
Send this article by e-mail Cited by SciELO
Cited by SciELO  Cited by Google
Cited by Google  Similars in
SciELO
Similars in
SciELO  Similars in Google
Similars in Google 
 Permalink
PermalinkIntroduction
Plastic surgery as a specialty performs procedures that create stress and tissue damage, frequently giving rise to postoperative pain. Pain intensity is determined by factors such as the extent of the surgery, the anatomical site, the surgical technique, existing comorbidities, and individual cultural and psychological perceptions.1
The majority of cosmetic surgical procedures require a short stay in the postanesthetic care unit, after which patients are discharged for ambulatory recovery on oral analgesic management. However, anesthetists have used parenteral techniques (intravenous or subcutaneous) to achieve adequate outpatient analgesic control in certain cases.2
Elastomeric devices have been used for dosing analgesic medications. They consist of infusion pumps for continuous administration and maintenance of relatively constant plasma concentrations. These light-weight pumps have a clear plastic container with an elastomeric balloon in which the medication is introduced. When fully inflated, the balloon exerts continuous constant pressure, pushing its content through a filter and a flow reducer.3
Most of the experience with elastomeric infusion devices comes from palliative care and oncology patients who have received infusions of chemotherapeutic agents, antibiotics, analgesics, sedatives and anti-emetic drugs with good results, and stability of the mixes.3-7
In plastic surgery specifically, there is evidence about the use of elastomeric infusion pumps in mammoplasty and abdominoplasty. However, the studies considered used continuous infusions of local anesthetics at the site of the surgical wound and did not analyze the use of these devices for intravenous analgesic management. Moreover, they were not based on comparisons between regional and intravenous analgesia that could help identify the best option for the patient.8
Consequently, the objective of this study was to assess the efficacy of acute postoperative pain control in patients undergoing liposuction, abdominoplasty, and/or mammoplasty, managed with multimodal intravenous analgesia using the elastomeric pump.
Overall patient satisfaction with the analgesic technique, the need for rescue boluses, the presence of adverse effects, the need for readmission due to poor pain control, and the need for additional analgesic medication are also described.
Materials and methods
Prospective case series of a total of 100 patients included in the study following the approval of the Ethics and Research Committees of Universidad de Antioquia, Colombia and Clinica NOVA, Colombia.
Patient data were collected between December 2015 and March 2016. All of the patients were over 18 years of age, American Society of Anesthesiologists (ASA) I-II, scheduled for elective mammoplasty, abdominoplasty, liposuction, or a combination of these procedures at the NOVA plastic surgery clinic in Envigado, Antioquia.
Upon admission to the surgery service, eligible patients were explained the procedure and given the informed consent before they were taken to the operating room. Anesthetic induction and intraoperative analgesic management were left to the discretion of the anesthetist.
Postoperative pain management was initiated in the post-anesthesia care unit using the elastomeric pump (AIPU MEDICAL) containing the following mix of medications: Tramadol 500 mg, Ketorolac 180 mg, Ondansetron 40 mg, Dexamethasone 8mg, in 275 cm3 of 0.9% saline solution for intravenous administration. The infusion rate was set at 3 cm3/hour, maximum 5 cm3/hour, for 5 days. In the event of pain exacerbation during that time period, the patient was instructed to administer a 0.5 cm3 bolus through the Pacient-Controlled Analgesia (PCA) mechanism in the pump, limited to a maximum 15-minute interval.
Patients and/or family members were instructed in the use of the pump and were given information about signs of alarm and contact information in case they had any questions or problems.
Table 1 Baseline characteristics of the patients included in the study (n=100)
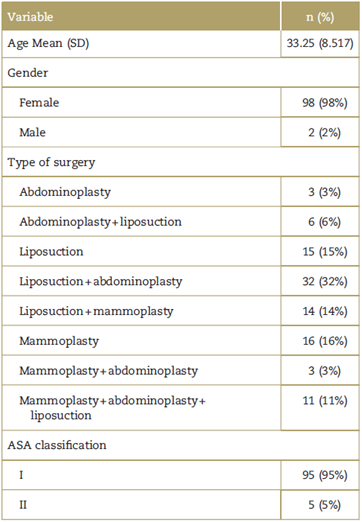
ASA: American Society of Anesthesiologists.
Source: Authors.
A telephone survey was given on postoperative day 1 to assess the following areas: pain control, using a numerical categorial scale from 1 to 10 where 1 to 3 was mild pain, 4 to 6 moderate pain, and >6 severe pain, and treatment was considered effective if pain was mild; need for, and number of, rescue boluses per day and need for oral analgesic medication; the degree of satisfaction with the intervention on the Likert scale (very satisfied, somewhat satisfied, not satisfied or dissatisfied, somewhat dissatisfied, and very dissatisfied); hospital readmission for pain management; side effects of the medication and their incidence (nausea and/or vomiting, constipation, drowsiness, dyspepsia, and gastrointestinal bleeding). The survey was repeated on postoperative days 3 and 5.
Results were analyzed using the SPSS 22 (IBM Corporation. Released 2013. IBM SPSS Statistics for Windows, Version 21.0. Armonk, New York) statistical software package. Qualitative variables were analyzed in terms of frequency and proportion, whereas quantitative variables were analyzed as means and standard deviations.
Results
Overall, data for 100 patients undergoing cosmetic plastic surgery were collected between December 2015 and March 2016. Table 1 shows the baseline sociodemographic characteristics of these patients.
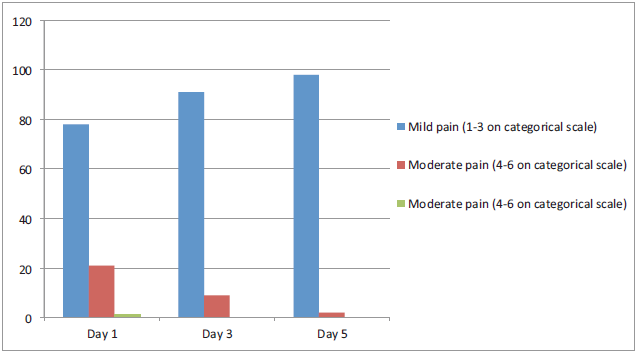
In general terms, the vast majority of patients had mild-to-moderate pain with the analgesic strategy studied and only 1 patient reported severe pain on the first day of assessment, with a score of 7 on the numerical analogue scale. Figure 1 shows analgesic efficacy results.
Patients did not report dissatisfaction with the analgesic strategy during the study period. In fact, during follow-up, the percentage of patients who were totally satisfied increased between day 1 and day 5 (from 91% to 98%). Figure 2 shows satisfaction results.
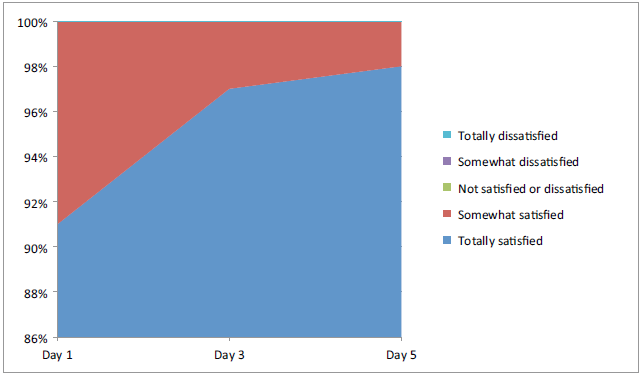
Source: Authors.
Figure 2 Degree of satisfaction of the patients included in the study according to the day of assessment.
Mean rescue boluses on days 1, 3, and 5 were 1.17 (Standard Deviation (SD) 1.627), 0.79 (SD 1.140), and 0.22 (SD 0.660), respectively. Only 5 patients needed additional oral analgesics on top of the strategy under study: 3 used acetaminophen, 1 used naproxen, and 1 use acetaminophen + codeine. None of the patients required hospital readmission for pain control.
Finally, 13% of the patients reported nausea during the follow-up period, 16% reported constipation, 8% experienced drowsiness, 6% reported dyspepsia, and there were no reports of gastrointestinal bleeding.
Discussion
Pain control is one of the most important problems following any type of surgical procedure; for this reason, objective assessment and the use of prophylactic and therapeutic strategies are part of the anesthetist's everyday job in achieving this objective.
ln cosmetic plastic surgery, a study conducted in a hospital in Sao Paulo with 200 patients who underwent procedures such as liposuction, dermolipectomy, mammary implants, and combinations of these procedures under different anesthetic techniques (conductive epidural or spinal anesthesia, general anesthesia, or combinations of these techniques) showed that although the majority of patients had no pain or mild pain, 4% of the patients taken to liposuction, 1.7% of the patients receiving mammary implants and 10.9% of the patients taken to liposuction+ mammary implants had strong or severe pain, highlighting the importance of the management of acute postoperative pain following these types of procedures.1
Support of analgesia based on continuous infusions using elastomeric pumps in plastic surgery is given with regional analgesia. For breast surgery, Lu and Fine9 reported a case-control study comparing bupivacaine in continuous infusion with conventional analgesic management, with a significant improvement in pain scores, narcotic use and length of stay, and no difference in terms of complications. Kryger et al10 published 2 randomized studies, the first comparing the use of 0.25% bupivacaine in infusion pump versus absence of use, and the other comparing the use of continuous infusion of 0.25% bupivacaine versus the use of saline solution in the infusion pump. The 2 studies showed improved pain control, less use of narcotics and less postoperative nausea and vomiting. There are also reports of its use in abdominoplasty with ambiguous results.11,12 Our work was designed to assess pain control efficacy using the intravenous route, but studies comparing the 2 routes are required to determine which is the most effective analgesic strategy.
Few studies have examined the efficacy of analgesic mixes in continuous infusion with elastomeric pumps in the surgical setting. In 2002, Pieri et al published a prospective descriptive study of 585 patients taken to major abdominal surgery who were managed with a mix of ketorolac + tramadol in continuous intravenous infusion with elastomeric pump. These authors found that pain was always mild (less than 3 on the verbal numerical scale) and that 22.6% of the patients reported nausea and 8.5% reported vomiting, but there was no respiratory of hemodynamic compromise.12 In a retrospective study, Rodríguez de la Torre et al evaluated pain intensity, the need for rescue analgesia, side effects, sleep disorders, and degree of satisfaction in 463 patients undergoing different outpatient procedures such as hallux valgus correction, shoulder arthroscopy, hemorrhoidectomy, and tonsillec-tomy. They were given intravenous analgesia using elastomeric pumps with dexketoprofen + tramadol + ondansetron or metamizole +tramadol + ondansetron as the postoperative analgesic strategy, and the study showed that 69% of patients had mild or no pain, only 16 patients had severe pain, 27% required rescue analgesia, 4% reported vomiting, 2% had dizziness, 2.5% reported drowsiness, and 0.5% had insomnia. Moreover, 83% of the patients reported high satisfaction with the analgesic strategy and 16% reported moderate satisfaction.2 A comparison of the results of these 2 studies with our own results found that the percentage of patients who reported mild pain are the majority in the study samples, suggesting good analgesic efficacy (in this study, mild pain was reported by 78%, 91% and 98% of the patients on days 1, 3, and 5, respectively, and only 1 patient reported severe pain on day 5). Another finding was that although side effects associated with the use of opioids in the analgesic sample (especially nausea, vomiting, and drowsiness) are somewhat frequent, they did not result in significant complications or the need for hospital readmissions, and did not affect satisfaction, which was more than 80% in all the cited reports. In our study, 100% of the patients were satisfied and the percentage of total satisfaction increased between day 1 and 5 of follow-up.
The present study is the first of its kind in assessing an intravenous analgesic strategy with elastomeric pump in patients taken to plastic surgery in an outpatient setting. Based on these results, this approach can be considered as an option that is well accepted by the patients and is associated with few side effects.
Being a case series and not a comparative study, data correspond to patient experiences and measures of association, and specific outcomes cannot be evaluated. Consequently, further studies are needed to determine the analgesic efficacy of this strategy compared with standard analgesic treatment (oral treatment in our setting) or regional analgesia, among other options.
Conclusion
Ambulatory intravenous analgesia using elastomeric pumps is an effective alternative for postoperative pain control in patients undergoing plastic surgery. Our results suggest few side effects, a good level of satisfaction, little need for additional oral analgesic, and no hospital readmissions.
Ethical disclosures
Protection of human and animal subjects. The authors declare that the procedures followed were in accordance with the regulations of the relevant clinical research ethics commit-tee and with those of the Code of Ethics of the World Medical Association (Declaration of Helsinki).
Confidentiality of data. The authors declare that they have followed the protocols of their work center on the publication of patient data.
Right to privacy and informed consent. The authors have obtained the written informed consent of the patients or subjects mentioned in the article. The corresponding author is in possession of this document.

