











 texto en
texto en  Inglés (pdf)
Inglés (pdf)
 Articulo en XML
Articulo en XML Referencias del artículo
Referencias del artículo
 Enviar articulo por email
Enviar articulo por email Citado por SciELO
Citado por SciELO  Citado por Google
Citado por Google  Similares en
SciELO
Similares en
SciELO  Similares en Google
Similares en Google 
 Permalink
PermalinkIntroduction
Post-mastectomy pain syndrome (PMPS) is a disorder that develops after recent breast cancer surgery that affects the anterior chest wall and the medial and proximal segment of the upper limb, secondary to a potential lesion of the intercostal-brachial nerve and/or intercostal nerves during axillary level dissection that accounts for the neuropathic pain characteristics that may persist for years. 1-3. The incidence of the syndrome has been described in the literature, varying from 13% to 69%.3 Vilholm et al4 found in a survey administered to patients who underwent mastectomy for breast cancer, compared with a group of women with breast cancer receiving nonsurgical treatment, that 23% experienced chronic pain compatible with post-mastectomy pain syndrome. When patients were asked about the impact of pain on their daily activities, 6% said "too much" or "enough." Similar incidences were previously described in the cohorts studied by Smith et al (29%) and Carpenter et al (27%).5,6 Perkins and Kehlet7 found a 50% incidence of chronic pain in his study on mastectomy.
There are different risk factors associated with the development of chronic pain after breast cancer surgery, 8,9 where the perioperative anesthetic and analgesic techniques could be relevant, as shown by the findings of the Ibarra Martí group, comparing the incidence of post-mastectomy pain in patients with preincisional paravertebral analgesia and conventional parenteral analgesia, using an over-the-phone questionnaire administered to patients. 10 It has also been documented that between 5% and 10% of patients presenting with chronic postoperative pain (heart surgery, dental surgery, mastectomy) experience severe pain intensity with a negative impact on quality of life. 11-13
In Colombia, breast cancer is the major cancer pathology in women, accounting for up to 22.3% of the cancer-associated deaths among women. 14,15 Close to 50% of the patients diagnosed in Colombia undergo surgery (both quadrantectomy and mastectomy) as part of their cancer therapy; however, no national or regional statistics about the prevalence of PMPS are available.
Materials and methods
An observational, prospective, cohort-type study was conducted at the Santander University Hospital from January, 2014 through July, 2015. The inclusion criteria were patients diagnosed with breast cancer undergoing therapeutic cancer surgery over this period, and more than 3 months after surgery (range 4-22 months). The following were the exclusion criteria: patient's refusal to participate in the study and patients with prior breast surgeries. The data collection was done through a survey designed to identify chronic pain at 1 point in time during the follow-up visit by the Pain Clinic (see Fig. 1). To minimize errors, 2 different data entry operators entered the data collected in a database using an electronic Excel sheet. The accuracy of the data was then verified and transferred to the Stata 1 statistical software for processing and final analysis.
Statistical analysis
A univariate analysis was initially conducted describing the percentages and central trend measurements, evaluating the distribution of the variables corresponding to the analysis. A bivariate analysis was conducted according to the nature of the variables using chi-square and Fisher exact tests. Due to the nature of the variables, the bivariate analyses between dichotomous and quantitative variables were conducted with Mann-Whitney U test.
Results
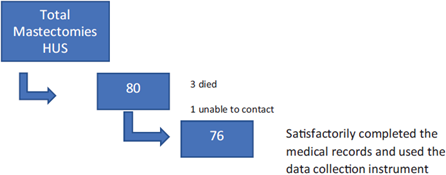
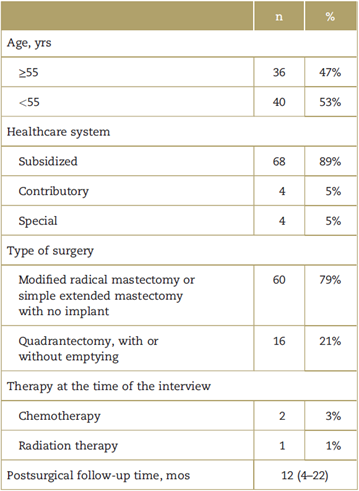
The procedure records and the medical records of the Santander University Hospital from January, 2014 through July, 2015 were reviewed, and 80 patients who underwent therapeutic breast cancer surgery were selected. Three of them had died at the time of the follow-up visit and in 1 case it was impossible to contact the patient because of missing information in the medical record. The final sample included 76 patients (Fig. 1), with an average age of 55 years. The rest of the demographic characteristics are shown in Table 1.
At the time of the interview in the follow-up visit, 55.3% of the patients registered some type of chest wall, arm, or back pain after surgery. Furthermore, pain was characterized as somatic (myosfascial), neuropathic, and phantom breast pain. Also, 23% of the patients reported experiencing more than 1 type of pain.
Among the patients, 54.8% presenting with some type of pain after surgery said it was a mild intensity pain (visual analog scale [VAS] ≤4) and 42.9% rated the pain as moderate intensity (VAS 5-7). Only 1 of the patients interviewed (2.4%) reported severe intensity pain.
With regards to the pain with neuropathic characteristics, 26 patients (34.2%) of the total sample said they experienced surgical site burning pain or allodynia after the procedure.
The prevalence for surgery-associated myofascial pain was 42.1%. Among the patients who reported experiencing pain and muscle contractures, 56.3% rated the pain as mild intensity (VAS ≤ 4) and 43.7% rated the pain as moderate intensity (VAS 5-7).
In our study, 19.7% of the patients said they still feel or had felt the breast surgically removed (phantom breast) and 66.7% of them described the sensation as painful, with 90% of the cases being mild-intensity pain and the remaining 10% severe.
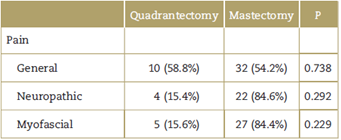
Although our study found that the patients undergoing radical mastectomy versus patients undergoing quadrantectomy present a higher prevalence of neuropathic and myofascial pain, this difference is not statistically significant and may be accounted for based on the size of the sample (Table 2).
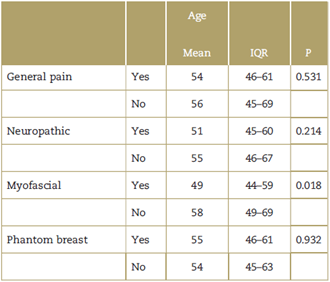
Pain presentation among the study patients was also compared based on age (Table 3), and, in general, we found that the patients experiencing pain were younger in contrast to the asymptomatic patients, with statistical significance for patients with myofascial pain, in whom the mean age was 49 years versus 58 years for the pain-free patients (P = 0.018).
Discussion
The cure and survival rates of cancer patients has been rising over the past few years as a result of the progress made in the various early-detection strategies and medical-surgical treatment. The objective with these patients, in addition to their recovery from their oncological condition, is to ensure adequate quality of life to conduct their daily life activities and play their social role with no limitations. Pain is 1 of the key symptoms in cancer patients, presenting in up to 20% of the patients who survive the disease. Of these, approximately 50% experience moderate to severe pain that limits the performance of their everyday activities. Part of this pain is associated with the occurrence of chronic postoperative pain, secondary to surgical interventions for cancer treatment. At the national level, there are no statistics available on PMPS to assess the scope and consider the possibility of timely and even preventive interventions to lower the incidence of the disease. Our perception about PMPS before the study in our setting was around 30%, but we found an incidence above 50%. The predictive factors described by Krøner9 are: severity of acute postoperative pain, pain before surgery, the type of surgery, the nervous lesion, the adjuvant radiation therapy used, and psychological factors before the intervention. Although our study was not designed to identify any risk factors, a higher incidence can be seen among the mastectomy versus the quadrantectomy group; another relevant finding of this study is that age performs as a protective factor against the development of myofascial type of PMPS.
Conclusions
Post-mastectomy pain syndrome is a frequent entity in our population, with figures comparable with those of other studies conducted in other countries, affecting the quality of life of our patients. Though our study was designed to identify the incidence of PMPS, we found that younger patients were more prone to develop myofascial pain.
Ethical responsibilities
Protection of persons and animals: The authors hereby declare that no experiments in humans or in animals have been made for this research.
Confidentiality of the information: The authors hereby declare that no patient data have been published in this article. All personal data of patients were managed according to Law 1581 of 2012, ensuring secrecy and confidentiality of all personal information.
Right to privacy and informed consent: The authors hereby declare that this article does not include any patient data.

