











 text in
text in  English (pdf)
English (pdf)
 Article in xml format
Article in xml format Article references
Article references
 Send this article by e-mail
Send this article by e-mail Cited by SciELO
Cited by SciELO  Cited by Google
Cited by Google  Similars in
SciELO
Similars in
SciELO  Similars in Google
Similars in Google 
 Permalink
PermalinkIntroduction
Malpractice claims are filed when there is the perception that the performance of the medical practitioner was inappropriate, unskilled, or negligent.1 There has been a growing number of claims in most countries between 1980 and 2010. 2,3 In response to this situation, the surveillance systems of poor outcomes in healthcare have been improved. 4 Nevertheless, there also has been a negative impact on healthcare costs, the practice of defensive medicine, and on the wellbeing of healthcare providers, 5-7 the specialties with higher risk of being the target of malpractice claims are: emergency medicine, gynecology and obstetrics, anesthesiology and the surgical specialties. 3,8
One of the potential causes of malpractice claims are the poor outcomes in healthcare identified as reportable events (REs), 9,10 or adverse events (AEs). 11 REs occur in 5% to 17% of hospitalized patients and 38% to 58% are preventable. 11,12 In obstetrics, the frequency ranges from 3% to 12%, and 54% to 70% are preventable. 13,14 REs exhibit a mortality around 2.8% to 4% per 1000 admissions. 15,16 The methodology to study the frequency and classification of REs is clearly described, 11 as well as the research and analysis of associated factors. 17
It is important to assess the factors associated with the judicial decisions in malpractice claims, particularly when the presence of preventable REs increases the risk of an unfavorable decision. Furthermore, there is a need to identified issues to be tackled through strategies aimed at reducing the risk of patients to experience a RE and the risk of doctors to be the target of a malpractice claims. Therefore, the purpose of this study is to assess whether there is an association between the occurrence of a reportable preventable event and an unfavorable legal or ethical decision.
Materials and methods
Design and population
Case-control study based on a cohort of legal or ethical processes between 1999 and 2014, against obstetricians affiliated to FEPASDE (Special Fund for Solidary Assistance during legal claims) associated with the Colombian society of Anesthesiology and Resuscitation (S.C.A.R.E.) in Colombia. Obstetricians with processes unrelated to healthcare services, associated with gynecological care, or with insufficient information were excluded. Cases were those proceedings which ended up in an unfavorable legal or ethical decision, including guilty verdict, admonishment, fine, conciliation, compensation, settlement, indemnity payment or disciplinary measure. The controls were litigations with a favorable ruling, including not guilty verdict, judgment for the defendant, lawsuit inadmissibility, revocation of guarantor inclusion, impleader repeal, falls under the statute of limitations or filed close.
Sampling and sample size
The cases were selected based on an unfavorable legal or ethical ruling. If an obstetrician had more than 1 malpractice claims, one of the processes was selected randomly. Controls were selected from the cohort using a simple random sampling. The size of the sample was estimated using OpenEpi, with an expected percentage of cases exposed to reportable preventable cases of 70% in the group of cases and of 50% among the control group, based on reported incidents of preventable REs in obstetric services. 12,18,19 In addition, a case-control ratio of 1:4 was established, with a 95% confidence level and 80% power, for a total sample of 325 (65 cases and 260 controls).
Procedure
Based on FEPASDE's database, the malpractice claims involving obstetricians in the study period were identified, and the inclusion and exclusion criteria were verified. Data were collected regarding: Patient's baseline, healthcare management in each particular claim, the legal or ethical process, the obstetrician and the healthcare institution. The information was entered into a data collection form by 2 general practitioners previously trained in the management of the data base and medical records. Subsequently, the methodology validated in Colombia and developed by Baker et al for the identification and assessment of RE was followed. 11,12 It was identified processes with screening events-defined as situations where unexpected events happened while providing patient care-that require further analysis or investigation11 to determine whether a RE actually occurred with the mother or the fetus or neonate. Those processes with an identified screening event were evaluated by an expert committee comprising 2 obstetric consultants from FEPASDE and 1 anesthesiologist with expertise in obstetric critical care, in order to decide whether there was a RE or not. The committee qualified a RE based on a numeric scale from 1 to 6. A rating of 1 to 3 associate the result with the underlying condition rather than with the health care management, while 4 to 6 associate the outcome with the health care management, rather than with the underlying condition. In terms of whether the outcomes were preventable, 1 to 3 rate the undesired result as non-preventable, while 4 to 6 is preventable. A cut point of 3 was used to rate the RE and to consider it preventable. The committee was not aware of the final litigation ruling and their opinion was based on the medical record and the information in the file. In addition, an analysis was conducted of the potential shortcomings in the health care management that led to reportable preventable events.
Variables
Obstetrician: age, gender, other ongoing malpractice claims. Institution where care was delivered: type of institution, location. Process: type of process (criminal, civil, ethical, administrative, and/or disciplinary). Patient: age, type of admission, gestational age, and time of occurrence of the event that led to the claim, newborn weight, diagnosis of the poor fetal outcome, neonatal demise, mode of delivery, type of discharge, type of health insurance (contributory, subsidized), presence of a reportable preventable or non-preventable event20 and whether the RE occurred during delivery or was directly associated to it. The exposure was the presence of a reportable preventable event-defined as injuries inflicted as a result of health care management, which could have been prevented by following the best available management recommendations. The non-exposure group was defined as the absence of injury resulting from health care or the presence of a reportable unavoidable event, meaning that even if the best available management recommendations had been followed, the event could not have been prevented. 11
Analysis
The qualitative variables were expressed as absolute and relative frequencies, while the quantitative variables were expressed through means and standard deviation for the normal distribution variables, and medians and interquartile ranges for the non-normal distribution variables. The normality of the variables was evaluated using the Shapiro-Wilk test. The baseline characteristics of the cases and controls were compared using Mann-Whitney or Chi-square and Fisher exact tests, based on the type of variable. The association between reportable preventable event and an unfavorable legal or ethical decision was evaluated in the bi-varied analysis through crude Odds Ratio (OR) and its corresponding 95% confidence interval (CI). Finally, to assess the association between reportable preventable event and an unfavorable legal or ethical decision, adjusted for other variables, a multivariate analysis was conducted using a non-conditional logistic regression model that included the use of a propensity score, which strengthens the validity of the study by providing even more robust estimates, allowing for the control of unknown confounding variables, considering that this is an observational study with an important risk of confounding bias. 21,22 The propensity score was estimated for each one of the malpractice claims, including the following covariables: the type of institution, type of admission, type of lawsuit, diagnosis of the fetus, whether the event was associated with the surgical procedure, the age of the patient, and whether the doctor had a history of additional claims given that these variable were considered relevant from the clinical point of view.
These same variables were included in the logistic regression model, together with the weights of the propensity score. Since the 2 groups (cases and controls) were not matched based on the propensity score result, a non-conditional logistic regression model was used. The backward strategy was implemented for the selection of the variables in the final model. In every case a p value of less than 0.05 was considered statistically significant. The analyses were conducted using Stata 13 (StataCorp. 2013. Stata Statistical Software: Release 13. College Station, TX: StataCorp LP).
Ethical considerations
The study was evaluated by the Ethics Committee of S.C.A. R.E with minutes' number CE 201509 dated September 1, 2016. The confidentiality and privacy of the obstetricians, the institutions, the patients and persons involved in the process was insured. Being a retrospective study, informed consents were not required.
Results
A total of 64 cases and 258 controls were included. Reportable preventable events were identified in 268 of the 322 lawsuits included (83.2%). When comparing the cases against the controls, the former had a significantly higher frequency of: reportable preventable event, private institution, contributory regimen, civil lawsuits and fetal demise. (Table 1).
Table 1 Baseline characteristics of cases and controls undergoing malpractice claims covered by FEPASDE (S.C.A.R.E.) Colombia 1999 to 2014.
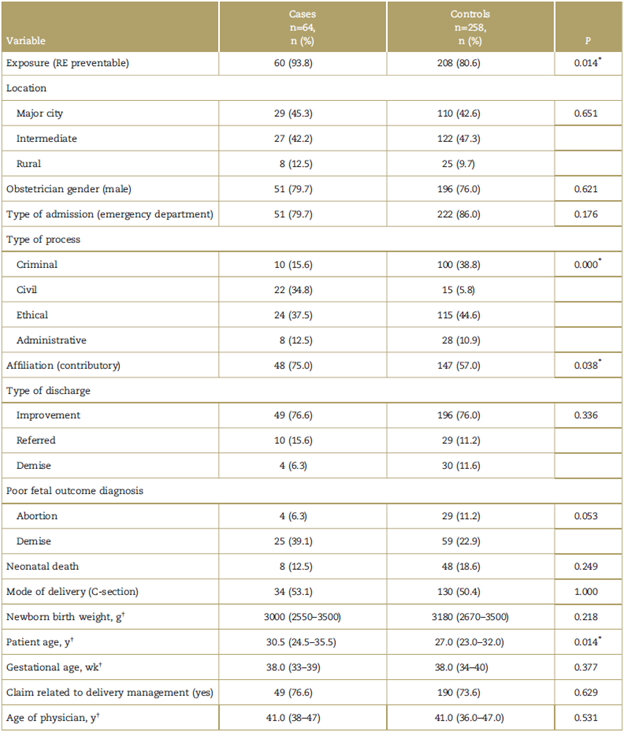
RE = reportable event.
*Statistical significance (P<0.05).
†Mann-Whitney test.
Source: Authors.
When comparing the groups of patients with a reportable preventable event versus patients with reportable non-preventable events or without RE, there were differences in terms of rural located institution, and pre-term gestational age. No differences were found in terms of the other characteristics between the 2 groups (Table 2).
Table 2 Baseline characteristics of patients presenting with reportable preventable and non-preventable events, in processes represented by FEPASDE (S.C.A.R.E.) Colombia 1999 to 2014.
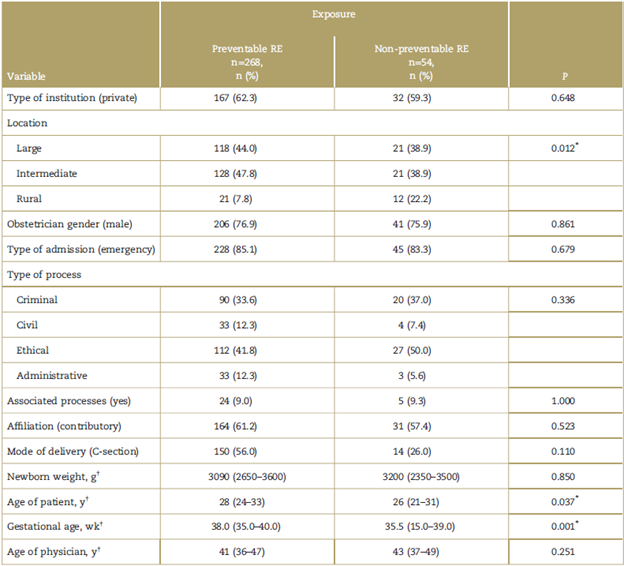
RE = reportable event.
Source: Authors.
*Statistical significance (P<0.05).
†Mann-Whitney test.
In terms of health care-associated deficiencies, all except for those associated with the administration of medications, were related to the reportable preventable event (Table 3) and failures in prevention and medication treatment were associated with an unfavorable legal or ethical decision (Table 4). The most frequent health care-associated failures were treatment delays (52%) or diagnostic delays (55%); and in terms of system deficiencies, the most frequent were delays associated with the management plan and communication issues (Table 5).
Table 3 Association between care deficiencies and the occurrence of a reportable preventable event in processes represented by FEPASDE (S.C.A.R.E.) Colombia 1999 to 2014.
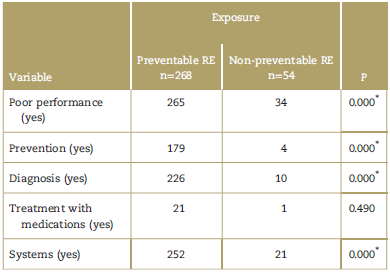
RE = reportable event.
*Statistical significance (P < 0.05)
Source: Authors.
Table 4 Association between deficient care and unfavorable ruling in processes represented by FEPASDE (S.C.A.R.E.) Colombia 1999 to 2014.
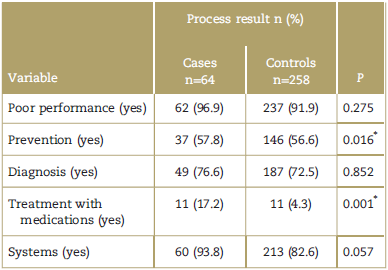
*Statistical significance (P < 0.05)
Source: Authors.
Table 5 Care deficiencies identified in processes represented by FEPASDE (S.C.A.R.E.) Colombia 1999 to 2014.
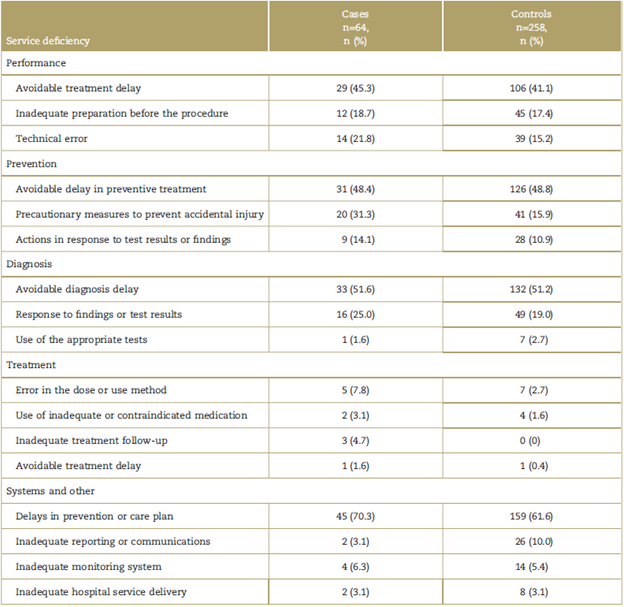
Source: Authors.
The bivariate analysis to assess the association between preventable RE and the unfavorable legal or ethical decision showed a crude OR of 3.6 (95% CI: 1.310.4). Other factors associated with an unfavorable legal or ethical decision were being affiliated to the contributory regimen OR: 2.22 (95% CI 122-419) and management in a private institution. The multivariate analysis including 92% of the data contained in the propensity score model resulted in an OR of 4.42 (95% CI: 2.23-8.76) between the preventable RE and an unfavorable decision about the process. An important association was also identified between an unfavorable ruling and care delivered at a private institution, with civil, ethical, or administrative processes, a final diagnosis of fetal demise, and obstetrician with a history of additional claims (Table 6). Since health care-associated failures are highly aligned with the occurrence of preventable REs (exposure to be assessed), these were not included in the final model. The goodness of fit of the logistic model was assessed using the Hosmer-Lemeshow test, indicating a good adjustment (P =0.32).
Table 6 Raw and adjusted OR estimate using logistic regression for the association between the occurrence of a preventable and non-preventable reportable event and favorable and unfavorable decisions in processes represented by FEPASDE (S.C.A.R.E.) Colombia 1999 to 2014.
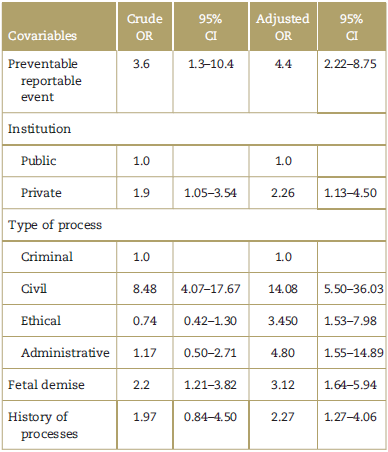
CI=confidence interval, OR=Odds ratio.
Source: Authors.
Discussion
The results of this study indicate that the occurrence of a preventable RE is an independent risk factor for unfavorable legal or ethical decisions in obstetric malpractice claims in Colombia. Other factors associated with unfavorable decisions is the type of process (civil, ethical, or administrative), health care delivered at a private institution, fetal demise, and obstetrician with a history of additional claims by other patients.
With regard to the presence ofRE's in malpractice claims, the results of the study are similar to those reported by Studdert et al23, who describe errors in the delivery of care in 72% of the claims leading to economic compensation in all specialties. This number is higher than the reported by Bishop et al, 24 with 47% of AE's in malpractice claims in inpatients, both studies from the United States.
The association between preventable RE and unfavorable litigation rulings has been reported by Phillips et al25. They found in a study on malpractice claims in primary care, an association between the occurrence of preventable REs and economic compensation. In obstetrics, Pettker et al26 conducted a before-after study, reporting that the implementation of a broad strategy to prevent AEs in obstetrics in an institution, achieved a reduction from 30 to 14 claims between 2003 and 2007 as compared against 1998 to 2002; Ransom et al27 in a case (deliveries ended up in legal claims) study and controls (deliveries that did not end up in claims with the same diagnoses as the cases) found that non-compliance with the clinical management protocols was significantly associated with malpractice claims (47% vs 11%) OR: 5.76 (95% CI 3.59, 9.2).
Regarding to fetal or newborn compromise as a risk factor for an unfavorable litigation decision, Kurki28 in 1997 reported in Finland a study on 801 claims nationwide, where 85% of the claims were filed as a result of events happened during labor; the cause that led to higher economic compensation was fetal asphyxia; Hale reports that neonatal injuries are among the primary causes of obstetric claims in the United States29; similar reports have been made by Domingues30 (2014) in Portugal.
With regard to deficiencies in the health care management, the findings are similar to those reported by Morris et al31 in general surgery malpractice claims, where they find diagnostic failures, treatment delays, surveillance issues, as well as by systems failures in communication and patient management plan. Furthermore, Clark evaluated 189 claims against obstetricians in the United States and found that 75% of those that lead to an economic compensation, showed deficiencies in the health care management. 32
Some of the strengths of this study are that both cases and controls belong to the same population; the analytical approach to this phenomenon is an additional contribution to the prevailing descriptive approach in most of the literature on the topic; the use of the propensity score who strengthens the results and reaches additional control of any confounding factors. Furthermore, the use of a validated methodology to assess REs.
Some of the limitations include the retrospective nature of the study that affects the quality of the information and could be a source of measurement and selection biases; the inability to conduct a subgroup analysis per type of litigation under the Colombian legal system. Finally, it should be highlighted that in case of claims with a high probability of an unfavorable result, occasionally the claim is settled before the court hearing in the Colombian system and therefore these situations could not be captured in this study; however, this potential bias leans the association found towards the null hypothesis.
Conclusion
The occurrence of preventable REs is associated with unfavorable legal or ethical decisions in civil, ethical, and administrative malpractice claims in Colombia. The outcome of a fetal demise is also associated with unfavorable rulings. Failures in patient management and in the operation of the hospital care system provide opportunities for intervention in order to reduce the risk of being subject to medical malpractice liability.
Ethical responsibilities
Protection of persons and animals: The authors declare that no experiments in humans or animals were conducted in this research.
Confidentiality of information: The authors declare that they have followed the protocols established in their workplace on the disclosure of patient information.
Right to privacy and informed consent: The authors declare that no patient data are included in this study.

