











 texto en
texto en  Inglés (pdf)
Inglés (pdf)
 Articulo en XML
Articulo en XML Referencias del artículo
Referencias del artículo
 Enviar articulo por email
Enviar articulo por email Citado por SciELO
Citado por SciELO  Citado por Google
Citado por Google  Similares en
SciELO
Similares en
SciELO  Similares en Google
Similares en Google 
 Permalink
PermalinkThe contribution of video-laryngoscopy to improving the process of orotracheal intubation has been shown if various publications emphasizing an improved and better quality vision of the mouth and the larynx; it is extremely valuable for teaching purposes and is part of the algorithm for the intubation of a predicted difficult airway.1,2
This article discusses the case of a 54-year-old patient admitted to the emergency OR for surgery of an ascending colon neoplasm and secondary intestinal obstruction. The patient has a history of smoking 10 packs/year, criteria consistent with chronic bronchial disease, and hepatitis C.
In the light of the risk of bronchoaspiration, induction, and rapid sequence intubation were conducted uneventfully. During the laryngoscopy with a Macintosh, an epiglottic mass was identified. Following the intubation and the tracheal pneumo-tamponade, we conducted a second laryngoscopy using a video laryngoscope Glidescope Titanium (Verathon Medical Bothell, WA, USA), which clearly revealed an epiglottic tumor.
After obtaining the consent of a family member, the planned hemicolectomy was conducted, in addition to a resection through laryngeal microsurgery and a biopsy of the epiglottic tumor identified (0.75 cm) (Fig. 1A and B).
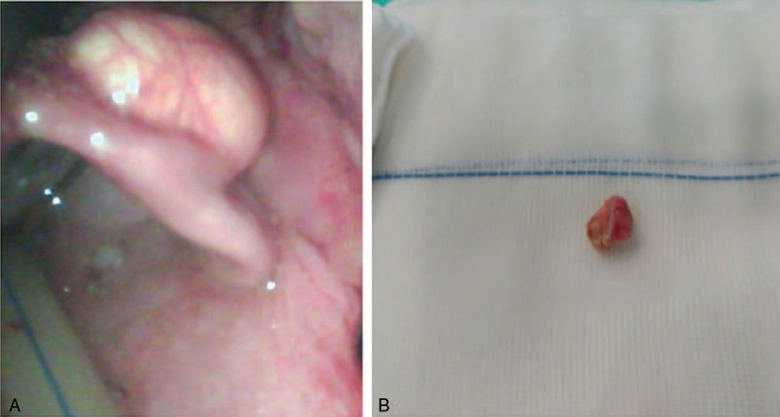
Source: Authors.
Figure 1 (A) Epiglottic mass seen through the video-lanryngoscope. (B) Epiglottic mass following the surgical resection.
Several papers argue that the total time elapsed during intubation and isolation of the airway is longer with the use of the video-laryngoscope versus the routine laryngoscopy, when the operator is still in the learning curve2; this is why the laryngoscope was used.
The use of video-laryngoscopes-Glidescope, King Vision-initially designed to facilitate orotracheal intubation, is very frequent in the algorithm for managing a difficult airway,3 in addition to a very exciting application in oropharyngeal surgery.4 Furthermore, we find that the device allows for an easy and minimally invasive exploration as compared against laryngoscopy using a rigid laryngoscope, as illustrated in our case in which the problem was solved in the same surgical-anesthetic procedure.
Ethical disclosures
Protection of persons and animals: The authors claim that no experiments in humans or animals were conducted for this research.
Confidentiality of the information: The authors declare that they followed the protocols of their workplace with regard to disclosure of patient data.
Right to privacy and informed consent: The authors declare that this article does not disclose any patient information.

