











 text in
text in  English (pdf)
English (pdf)
 Article in xml format
Article in xml format Article references
Article references
 Send this article by e-mail
Send this article by e-mail Cited by SciELO
Cited by SciELO  Cited by Google
Cited by Google  Similars in
SciELO
Similars in
SciELO  Similars in Google
Similars in Google 
 Permalink
PermalinkIntroduction
The 3 most important causes of death in Colombia are coronary disease, trauma, and cerebrovascular diseases.1 When a patient with any of these conditions arrives to the emergency room, securing a peripheral vascular access for administering medication is crucial.1-4 However, of all the adult patients admitted to the emergency department in a critical condition, only in 60% a patent vascular peripheral access is secured in the first few minutes,5 and failure to establish a vascular access accounts for up to 92% mortality.4,6,7 Consequently, a rapid response system has been designed with the participation of staff trained in high complexity vascular accesses, including intraosseous and central venous accesses.7,8 This approach ensures better and more effective management to reduce morbidity and mortality of the critically ill patient.
Since intraosseous devices are not available in the emergency departments because of their high costs, other therapeutic options are needed for the administration of medicines to the critical patient, to reduce the mortality based on healthcare quality and using rapid response teams.9
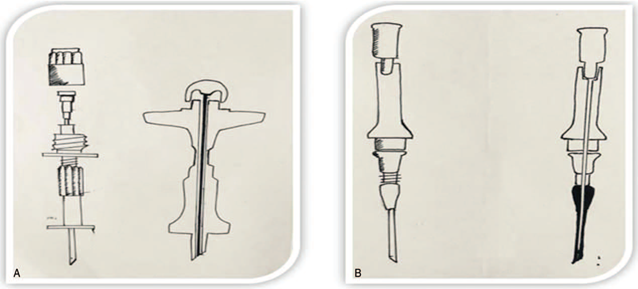
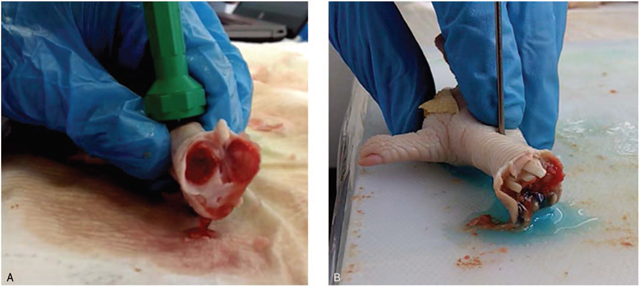
Recently, during the training program for undergraduate students at Universidad del Rosario, a conventional catheter has been used (Insyte 14) for interosseous access in a biological model with similar anatomic landmarks, resulting in a favorable efficacy. However, the comparison of the practicality of this conventional device versus a manual commercial device is yet to be made in clinical practice. Due to the clinical context of critical patients in the emergency department, the best initial method to do this comparison is a simulated environment. In addition, there is a need to use a biological model with similar anatomical-morphological characteristics to the human being. Thus, the purpose of this study is to compare the efficacy of the Insyte 14 catheter (Ci14, BD insyteTM, USA) versus the Din 1515x Illinois Desch, (Di15, jamshidi™, USA.) device, for a successful intraosseous access in a biological model (Fig. 1).
Materials and methods
A quantitative, experimental, randomized, head-to-head comparison trial was conducted of 2 devices in an avian tarsus-metatarsus model, using a factorial design with the following essential factors: number of procedures per session, number of professors, and number of procedures per professor. The research project was conducted at the simulation center of Universidad del Rosario (Bogotá, Colombia). The participants were professors of the simulation center, with at least 1-year experience in the emergency department and with no physical limitations to perform the procedures. None of them had any conflict of interests with the pharmaceutical industry. The biological models used were the chicken tarsus-metatarsus, which has been established a highly effective model for intraosseous access under simulated conditions.10
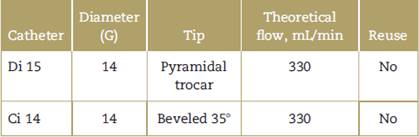
A standardization session was held with all the professor for the use of the 2 catheters and the safe management of biological models. Subsequently, the researchers responsible for data collection received training until a concordance index of more than 90% was achieved for the Ci 14 and the Di 15 (confidence interval [CI] 0.92:0.97-0.99; CI0.98:0.93-0.99), respectively (Table 1).
A descriptive analysis showed the central tendency measurements for the quantitative variables (puncture time and number of attempts), and frequency and percentage tables were developed for the qualitative variables. With regard to the quantitative variables- puncture time and number of attempts-Kolmogorov-Smirnov tests for normality were conducted to define their distribution. The result of these tests was a non-normal distribution, so the median central tendency measurements and interquartile indices were presented. Moreover, the analysis of related samples was conducted using the asymptotic Mc Nemar ji2 test for efficacy variables at the first attempt and final efficacy, whilst for the quantitative variables,-the number of attempts and puncture time- the asymptotic Wilcoxon rank test was performed.
Pursuant to Article 11 of Resolution 8430 of October 4, 1993 of the Colombian Ministry of Health, this research is considered a minimal risk project; consequently, the project was submitted for approval before the ethics Committee of the Colegio Mayor de Nuestra Señora del Rosario, and approved as recorded in the Minutes No. 320, of June 20, 2016. The professors participating in the research were fully insured for occupational risks, ensuring coverage for any healthcare services and payment of fringe benefits according to the law. There were no time limits for these services as they were intended to provide rehabilitation and ensure the recovery the workers from any adverse event. All of the participants signed the informed consent. The biological models were procured from an industrial vendor having the appropriate health license issued by the Health Secretariat and approved by the ethics committee.
Results
Primary outcomes
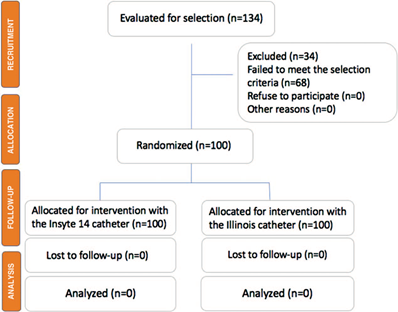
The informed consent of the 5 professors invited to participate was obtained for this research project. 134 biological models (avian tarsus-metatarsus) were received, of which 34 were excluded due to bone fractures. So 100 models were included and subject to puncture with both catheters, using both a distal and proximal approach. None of the models were excluded during the follow-up for a few minutes after the intraosseus procedure, so 100 procedures were analyzed with each catheter randomly allocated (Fig. 2).
Four of the 5 professors who did the procedures were males and most of them were between 30 and 39 years old, with over 2 years of clinical experience in the emergency department. Only 2 of them were clinical-surgical specialists, since they were professors of emergency medicine. All of the professors were right-handed (Table 2).
Table 2 Social and demographic characteristics based on the type of device used for the intraosseous procedure.
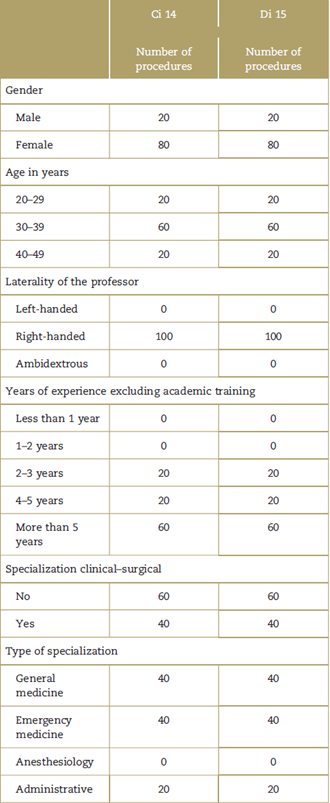
Source: Authors.
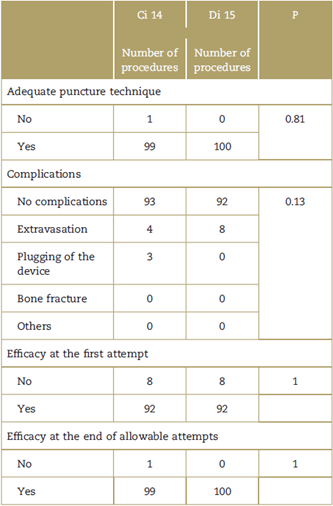
A total of 92% of the cases had a successful intraosseous access at the first attempt with both catheters, while the final efficacy allowed (<3 attempts) was achieved in almost every case with both catheters. Only in one of the procedures performed by the professors the technique was inadequate and failed at more than 3 puncture attempts (Table 3). The success of intraosseus access was identical with both catheters, both in the first attempt and in the final number of attempts allowed (<3) (P = 1, P = 1, respectively) (Fig. 3). Moreover, the laterality of the professor, experience and complications, show a relationship with the efficacy of the procedure (P = 0.16); in other words, achieving a successful intraosseous access in the chicken's tarsus-metatarsus is not dependent on the type of specialization of the professor, or the number of years of experience, provided an adequate technique is used. In terms of the gender, age, and clinical-surgical specialty variables, none of them were associated with the efficacy of the procedure (P = 0.18); that means that the success in obtaining an intraosseous access is not dependent on the sex, the age, or the clinical-surgical specialty of the professor, but on having at least 2 years of clinical experience in the emergency department.
Secondary outcomes
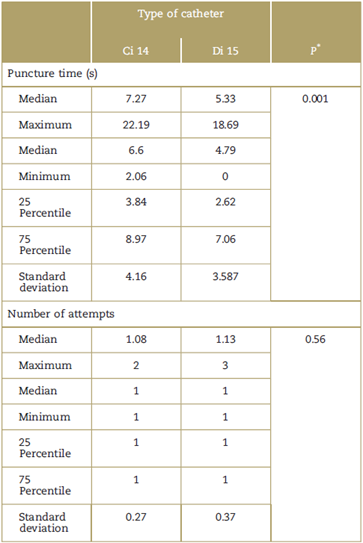
Time to intraosseous access and number of attempts based on the puncture device. The average time to secure a successful intraosseous access with Di 15 was 4.7 seconds, and with Ci 14 was 6.6 seconds, with a significant reduction of around 2seconds using the Di 15 device (P=0.001). With regard to the number of attempts, the average for the 2 catheters was 1 puncture attempt to secure the intra-osseous access, so the number of attempts required to secure access in the chicken tarsus-metatarsus was identical with both devices (P=0.56) (Table 4).
Table 4 Puncture times and number of attempts with each device.
* Wilcoxon rank test.
Source: Authors.
Complications. In over 90% of the cases, there were complications in securing intraosseous access in the biological models (avian tarsus-metatarsus) by the professor at the simulation center. When a complication developed, it was mostly due to extravasation in 8 procedures with the Di 15 device and in 4 procedures with the Ci 14 device. This difference is not significant (P = 0.13). Plugging of the device only occurred in 1% of the procedures, and only with Ci 14 (Table 3).
Discussion
Most of the procedures in this research project were conducted by males, professors with no clinical-surgical specialization and all of them were right-handed, with no physical limitations to do the procedure. In terms of the primary outcome, there was no significant difference between the 2 devices with regard to efficacy of intra-osseous access in the biological model.
The systematic literature review did not find a comparison between the 2 devices. However, there is a comparison between the commercial manual device and the mechanical, evidencing that the latter is better than the former.5,11,12 Notwithstanding this fact, due to cost reasons, most hospitals have mostly available the manual device.13 This is why our research project compared against a manual instead of an automatic device. This means that the Ci 14 device is equivalent to the manual devices available in the market, but we have no information about the results with mechanical devices. Moreover, this research project was conducted with biological models rather than with simulation models, as initially mentioned. Furthermore, the technique used did not include suction of the device, which could modify the results.
The research showed that there is no relationship between gender and a successful intraosseous access. Similarly, there is no difference between the professors with a clinical-surgical specialization versus those with no specialization, as long as they had at least 1-year experience in the clinical emergency setting.
An important consideration is the rate of complications with the devices. The frequency of complications was very low, with no significant difference between the 2 devices. However, the Ci 14 device was the only one that presented plugging in 3 procedures; this is because this catheter, in contrast to the Di 15 device, always has a patent lumen and so throughout the access procedure, the device is exposed to clogging from any type of tissue (Fig. 1). While there was no significant difference in the number of extravasations with the Di 15 device, the number was twice the number of extravasations with the other device. Since this is a commercial device specially designed for this purpose, the professors used more force, which lead to an increased number of cortical extravasations. Likewise, the Ci 14 device is more difficult to manipulate because it lacks a screw structure, which results in a more careful manipulation by the doctor.
In terms of time analysis, the literature says that as minutes elapse without succeeding in securing access, mortality of patients increases dramatically.14,15 This study evidenced that there is a significant difference in terms of time to intraossesous access between the 2 catheters, with a much better time for the Di 15 device. However, the investigators concluded that this statistical difference of 2 seconds in average is not clinically significant for a successful intraosseous access and the administration of medicines. Nevertheless, in contrast to the findings in previous trials, the study showed that trained staff is able to secure the access in just a few seconds, to administer fluids into the bone marrow.5,16,17
The number of attempts is a very important factor to secure an intraosseous access, since it affects not just the timeliness of administration of medications which is critical to the survival of critically ill patients, but also because of the contraindication of further attempts on the same anatomical site and the higher number of complications.6,18 This study showed that there is no statistical or clinically significant difference in the number of attempts between both devices; intraosseous access can be secured at the first attempt with any of the 2 devices in the biological models used.
Limitations of the study
The research project was conducted with the biological model of the tarsus-metatarsus of the chicken, by professor with clinical experience in simulation, so the difference in the results is only applicable to this type of population. Consequently, the investigators should not extrapolate the results to the clinical setting of critically ill patients in the emergency department. Moreover, the technique used failed to suction bone marrow at the beginning of the procedure, which may interfere with the occurrence of complications. Consequently, this type of studies should be conducted in critically ill patients to establish the efficacy of these low-cost devices for intraosseous access. It would also be interesting to carry out trials in simulated environments, comparing the need to suction bone marrow at the beginning of the procedure, since this fact may significantly change the technique for this vascular access.
Conclusion
The conclusion of the study is that in a simulated environment, using avian tarsus-metatarsus biological models, the efficacy of a low-cost device Ci 14 is identical to that of a commercial device-Di 15. Likewise, the number of attempts to secure the intraosseous access is the same with both devices. In addition, the conclusion is that the time required to secure the intraosseous access is less with the Di 15 device. Nonetheless, this 2-second difference is not statically significant.
Based on this research project, it is safe to recommend the use of low-cost devices such as the Ci 14 in simulated environments for the training of clinical skills in intra-osseous access with biological models. However, there is a need to extrapolate this type of studies to a clinical setting and determine the practicality of these devices in critically ill patients.
Ethical responsibilities
Protection of persons and animals: The authors declare that no experiments in humans or animals were conducted for this research project.
Confidentiality of the information: The authors declare that they have followed the protocols of their institution on the publication of participant’s information.
Right to privacy and informed consent: The authors obtained the informed consent of all participants mentioned in the article. This document is in the possession of the corresponding author.

