











 text in
text in  English (pdf)
English (pdf)
 Article in xml format
Article in xml format Article references
Article references
 Send this article by e-mail
Send this article by e-mail Cited by SciELO
Cited by SciELO  Cited by Google
Cited by Google  Similars in
SciELO
Similars in
SciELO  Similars in Google
Similars in Google 
 Permalink
PermalinkIntroduction
Pain is the most frequent symptom in cancer patients, presenting in 70% to 90% during advanced stages or end-stage of the disease. The pain has a mixed etiology: somatic, visceral, and neuropathic. Eighty percent of the pain is caused directly by the tumor and 20% is the result of anti-cancer therapy.1 Some patients, despite multimodal pain management, exhibit a refractory response. Following is a case description in which the erector spinae plane (ESP) block in a patient with chronic cancer pain, provided effective and extended analgesia for some time.
Case description
This is a 69-year-old male with a primary tumor of unknown origin and metastasis in the lumbar region. The patient said that his pain had 1 year of evolution; initially the pain intensity was 3/10 according to Visual Analogue Scale (VAS), and responded to conventional analgesia management (acetaminophen and ibuprofen), but then the pain extended into the entire back, including the cervical region and the lower limbs; the pain intensity raised to 9/10 at rest and to 10/10 during movement based on VAS. The patient did not tolerate the prone decubitus position, or raising his arms above the horizontal, and his gait was limited due to the pain intensity. The patient was treated with acetaminophen with codeine, pregabaline, and ibuprofen, but the pain did not improve. A thoraco-lumbar spinal magnetic resonance image (MRI) with contrast was ordered as an additional test. Radiology asked for the participation of the anesthesiologist to administer sedation or anesthesia to the patient, since immobility and prone position were required. During questioning, the patient mentioned a history of high blood pressure and chronic obstructive pulmonary disease due to smoking, in addition to frequent use of inhalers. The physical examination identified back muscle contracture, limitation to raise his upper extremities because of pain, and the lung auscultation revealed basal rhonchi and mobilization of secretions along the upper airway. His classification was American Society of Anesthesiologists (ASA)-Physical Status Classification System III. Being a patient at risk for respiratory and cardiovascular complications, a regional technique was considered the best option to general anesthesia. The bilateral ESP block at the level of T7, in accordance with the technique described by Forero et al, deliver analgesia to the chest, the abdomen, and the lumbar region. The treating anesthesiologist was experienced to do the procedure (Fig. 1).

After signing the informed consent, authorizing the procedure, insertion of the peripheral venous access # 18 in the right upper limb, and use of basic monitoring, the patient received sedation with 100 mg of fentanyl and 1mg of midazolam. The patient adopted the prone decubitus position with some difficulty. Asepsis and antisepsis was done. The transverse process corresponding to level T7/T8 was identified through echography (General Electric machine) with a lineal 10MHz transducer; the skin was infiltrated with 1% lidocaine, 3 cm on each puncture site and a 20 mL dilution for the hemithorax in the deep interfacial plane of the erector muscle of the spine was administered with a 100 mm BRAUN block needle (l-bupivacaine 0.5%: 10 mL +lidocaine 1%: 9mL + dexamethasone 4mg: 1mL) (Figs. 2 and 3).

Source: Authors.
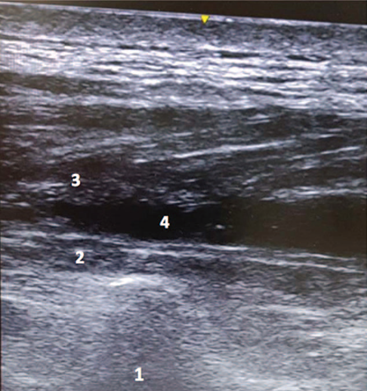
Figure 3 Dissection of the fascia between the rhomboid major muscle and the erector spinae. 1. Transverse process. 2. Erector spinae. 3. Rhomboid major. 4. Local anesthetic.
Five minutes after the administration of the bilateral erector spinae block (ESP), the VAS scale was 6/10, and after 10minutes, 2/10. This enabled the patient to comfortably adopt a decubitus prone position and raise the upper extremities to perform the MRI. The study was conducted uneventfully. At the end of the procedure, the patient expressed absence of pain. Two hours after the end of the procedure, the patient was discharged to the postanesthesia care unit. The case was followed and the patient submitted his informed consent to report his case. Two weeks later, during a personal interview, the patient-rated VAS score was 3 to 4/10 at rest and as 5/10 during movement, and expressed his gratitude for his remarkable improvement.
Discussion
The first reference to ESP block was in 2016 by the Colombian anesthesiologist Forero et al2, at McMaster University. An intrafascial US-guided block was administered between the major rhomboid muscle and the erector spinae, 3 cm lateral to the mid-line, at the level of the T5 transverse process in 4 patients (2 with refractory neuropathic pain receiving conventional therapy and 2 as postoperative chest surgery analgesia). A total volume of 20 mL of local anesthetic was used, with a cephalocaudal distribution through the anterior and posterior hemi-thorax. The block was highly effective for pain control. The suggestion by Forero et al2 is to administer the profound ESP block to the spinal erector muscle, using the transverse process of the vertebra as sonography marker; the proximity to the intervertebral foramen allows for irrigation of the dorsal and the ventral branches of the thoracic nerves. The ESP block has been reported as rescue therapy in case of failed epidural analgesia in chest surgery and analgesia in breast surgery3,4; as multimodal postoperative analgesia in pediatric patients,5,6 and in chronic shoulder pain using a mixture of local anesthetic and methylprednisolone.7 ESP block administered to the lumbar spine has been useful as an anesthetic strategy in hip and proximal femur surgery,8 in abdominal surgery,9) and in cesarean section.10
Is ESP block an alternative technique to the epidural and paravertebral approach? There are no comparative trials to date between this fascial block and the so-called standard techniques. The clinical evidence was initially limited to thoracic surgery and morphological analysis in cadavers. However, the future looks promising since a growing number of success cases are being documented with this new procedure which may be considered a basic, easy to learn block, with identification of structures, and low risk of complications because it is "distant" from the pleura, blood vessels, and the neuraxis.11-14
There have been several case reports on the use of ESP block in patients with oncological neuropathic pain, and case series of post thoracotomy pain syndrome-which is difficult to manage and responds poorly to analgesic agents-showing that ESP block provides palliative pain control and improves the patient's quality of life.15-19 A national, retrospective study described the use of ESP block in a population of 22 patients with chronic pain (38.1% of cancer etiology). There are quite advanced studies showing that the administration of local anesthetic agents and steroids results in lower VAS scores.
Further information is needed on the use of ESP block as palliative chronic pain treatment, as well as on the use of adjuvant therapies, the duration of the block, and repeated blocks, to consider this option in management protocols.
Ethical responsibilities
Protection of persons and animals. The authors hereby declare that no experiments in human beings or in animals were conducted for this research.
Confidentiality of information. The authors declare that all the protocols applicable at their worksite on the publication of patient information have been followed.
Right to privacy and informed consent. The authors declare that they have the informed consents for the use of the data, pictures, and clinical images of the patients involved.

