











 text in
text in  English (pdf)
English (pdf)
 Article in xml format
Article in xml format Article references
Article references
 Send this article by e-mail
Send this article by e-mail Cited by SciELO
Cited by SciELO  Cited by Google
Cited by Google  Similars in
SciELO
Similars in
SciELO  Similars in Google
Similars in Google 
 Permalink
PermalinkIntroduction
Density spectral array (DSA) is a parameter obtained from bispectral index (BIS) VISTA Monitoring System Bilateral (BVMS) (Aspect Medical Systems INC, Norwood, MA). The spectral analysis consists in analyzing small fragments of the electroencephalogram (EEG) and discomposing them into wave trains with specific frequency and amplitude to determine the spectral power. Through a Fourier analysis, it converts an unprocessed EEG trace into a spectrogram, and the EEG power is obtained in real time for each frequency. DSA shows the distribution of EEG strength in relation to frequency over the time.1 Clinical applications include monitoring of sedation, detection of cerebral ischemia, and identification of seizures.2
Asymmetry (ASYM) is a processed variable that indicates the percentage of EEG power present in the left or right hemispheres respect to the total EEG power. In a situation of clear difference between hemispheres, the ASYM indicates toward the hemisphere with higher force.
We describe a patient in whom the BVMS was used to detect changes in DSA during a left craniotomy for a frontal meningioma. The patient gave written permission for the authors to publish the report.
Case description
A 82-year-old man, Glasgow Coma Score 12, American Society of Anesthesiologists (ASA) grade II, with hypertension and a left frontal meningioma diagnosed as a result of difficulty in deambulation with left lateropulsion and seizures. He was scheduled for pre-surgical embolization of the frontal branch of the superficial temporal artery. It results partial because the artery was very tortuous and the skin was on risk of necrosis. The next day he was scheduled for a left frontal craniotomy. On entering the operating room, the electrocardiogram, non-invasive blood pressure, and the percentage oxygen saturation were monitored. BVMS electrode strip was placed on the front temporal position according to the International 10 to 20 system of electrode placement, and a BIS Vista was used to record BIS values. Anaesthesia was induced with fentanyl (200 μg), target-controlled infusion (TCI) of propofol (5 μg/ml) and rocuronium (40 mg) to facilitate endotracheal intubation. We monitored invasive blood pressure by femoral artery placed by the Neuroradiologist the day before. A right internal jugular vein was selected under ultrasound vision for monitoring the central venous pressure. Anaesthesia was maintained with TCI of propofol (2 μg/ml) and an infusion of remifentanyl (0.1 μg/kg/minutes) to keep BIS values within 54 to 50 range. An infusion of rocuronium was also administered (0.3mg/kg/hour). During the procedure the patient was unstable with hypotension, so an infusion of noradrenaline (0.4mg/kg/minutes) was initiated to maintain a correct cerebral perfusion pressure.
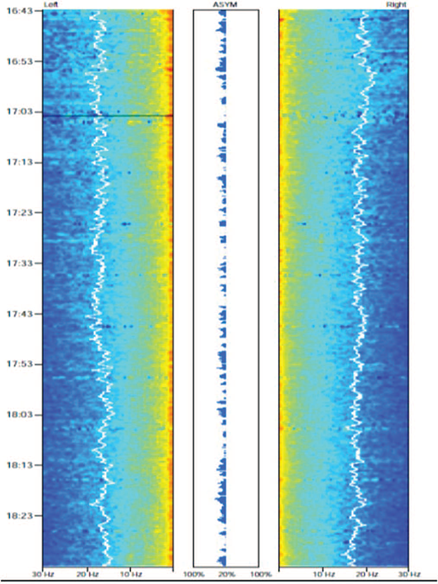
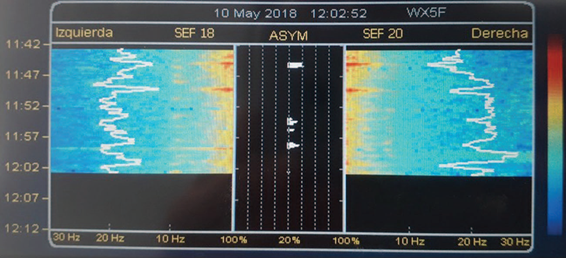
During the surgery he presented an ASYM to the left hemisphere, where the meningioma was. It was as a result of an increase in delta (0.1-4 Hz) and alpha (8-12 Hz) waves in this hemisphere (Fig. 1). The surgery elapsed without incident and the resection was almost complete. The patient was extubated in the operating room and transferred to the recovery room. The postoperative cranial tomography informed of complete removal. He was discharged from hospital 7 days later with Glasgow Coma Score 15. Fifteen days after, in a follow-up consultation with the neurosurgeon, a BVMS electrode strip was placed during 30minutes on the front temporal position again and we observed that the ASYM was gone and DSA was similar in both hemispheres (Fig. 2). Patient was satisfied with the surgery and its results.
Discussion
The bilateral BIS is a non-invasive system that allows the anesthesiologist to monitor and record continuously 4 EEG channels, 2 in each hemisphere of the brain.3 DSA applies fast-Fourier transformation to convert raw EEG into a time-compressed and color-coded display, also termed a color spectrogram.1,4 Clinical applications of DSA were demonstrated in various case reports described in the literature and include monitoring depth of sedation, detecting cerebral ischemia, and identifying seizures focus.2
During propofol and remifentanyl anaesthesia, bilateral monitoring of DSA allowed us to detect regional differences in the power spectrum between both hemi-spheres.1,5,6 Purdon et al stated that at loss of consciousness (LOC), both alpha (8-12Hz) and low-frequency (0.14 Hz) power increased significantly. Fifteen minutes after LOC, the increases in alpha power were concentrated in frontal channels, whereas those for low-frequency power were distributed broadly across temporal and parietal channels.6 In our case, DSA was observed to differentially display higher alpha and lower frequency power in the affected side (left), suggesting the location of the epileptogenic lesion. These hemispheric differences were easily observable through ASYM, persistent and maintained during the anaesthesia and surgical procedure, and disappeared when the lesion was removed. However, our case reveals that a complex algorithm such as BIS trend failed to detect interhemispheric differences, while DSA and ASYM were able to efficiently provide this information. The ASYM is a simplified way of viewing power differences noted in the DSA display between the left and right hemispheres and indicates the side with relative greater power like in this case.1 With more experience, DSA may, in fact, prove to be a very useful intraoperative neuromonitoring adjunctive tool.
One potential limitation of DSA is the lack of ability to detect changes in distant foci.5 For example, in patients with focal parieto-occipital disorders, there would be a lack of information regarding the epileptogenic lesion. In our case, we didn't have this limitation. We could observe differences because the epileptogenic lesion was in the frontal area.
In conclusion, we think that the use of DSA appears to be a further tool in monitoring brain state in neurosurgical patients and it could help in the monitoring of the surgery's effectiveness.
Ethical disclosures
Protection of human and animal subjects. The authors declare that no experiments were performed on humans or animals for this study.
Confidentiality of data. The authors declare that they have followed the protocols of their work center on the publication of patient data.
Right to privacy and informed consent. The authors declare that no patient data appear in this article.

