











 text in
text in  English (pdf)
English (pdf)
 Article in xml format
Article in xml format Article references
Article references
 Send this article by e-mail
Send this article by e-mail Cited by SciELO
Cited by SciELO  Cited by Google
Cited by Google  Similars in
SciELO
Similars in
SciELO  Similars in Google
Similars in Google 
 Permalink
PermalinkIntroduction
Total knee arthroplasty (TKA) or total knee replacement is one of the most frequent procedures performed by orthopedic surgeons. The goal of this surgery is to eliminate pain, restore joint mobility and function of muscles, ligaments, and other soft tissues.1 Despite the excellent outcomes that can be achieved in patients taken to TKA, postoperative recovery continues to pose a significant challenge.2
A high percentage of patients experience intense pain following TKA, and this percentage is among the highest of all surgical procedures. A distinction must be made between pain at rest (independent of stimulus) which may be as high as 40% and the pain caused by motion (stimulus-dependent pain) which may be as high as 95% in the first 3 days after surgery, delaying early patient rehabilitation.3 Opioid analgesics have been an option for the control of postoperative pain; however, they do not have a significant effect on stimulus-dependent pain while they do increase adverse effects such as nausea, vomiting, urinary retention, pruritus, sedation, and drowsiness.4,5 It is in these cases that regional techniques are important, as they reduce the harmful effects of pain on functional recovery and, moreover, reduce the risk of developing chronic postoperative pain.5
Pain control after TKA has become a challenge for anesthetists because of the need to cover the sensory territory of the main lower limb nerves. The surgical procedure involves the region innervated by the femoral nerve, which comprises the anterior compartment and, to a lesser extent, the medial region of the knee; and, the sciatic nerve which innervates the posterior compartment and the lateral region of the knee.6
There are different option for regional analgesia during TKA. The standard femoral nerve block (FNB) provides effective analgesia for the anteromedial region of the knee.(5 However, FNB has been found to reduce quadriceps contractility required for early rehabilitation; other complications have also been described, associated with postoperative muscle weakness, including in-hospital periprosthetic fractures secondary to a fall.7 More recently, the adductor canal block has been described for distal FNB, theoretically reducing the possibility of inducing motor block. Together with FNB, the sciatic nerve is blocked at the level of the popliteal nerve to provide analgesia to the posterior region of the knee; however, this technique has been associated with distal muscle weakness and drop foot.8
A new regional analgesia technique known as IPACK (infiltration between popliteal artery and capsule of the knee) has been used in practice since 2014.9 In this technique, the superomedial and lateral genicular nerves, branches of the sciatic nerve and articular branches of the obturator nerve in the popliteal region are blocked, providing analgesia to the posterior capsule of the knee joint, without affecting motor function of the limb.10
The objective of this observational study was to assess the analgesic and motor characteristics of the IPACK block used together with the FNB, measuring variables such as postoperative pain, opioid use, patient satisfaction, and ease of ambulation in patients undergoing TKA.
Materials and methods
A cohort study was carried out in the San Jose de Buga hospital, a Level III institution located in Buga, Colombia, between June and December, 2018. The study was approved by the Human Ethics Committee of the School of Health of Universidad del Valle, as stated in Minutes 264-018 (2018), and by the University. The participants in the study were adult patients over 18 years of age undergoing primary unilateral TKA. Informed consents were obtained from all the patients who agreed to participate in the study of their own free will. Patients allergic to opioid analgesics, non-steroidal anti-inflammatory agents or local anesthetics, patients with contraindications for neuroaxial anesthesia or patients converted during the procedure from neuroaxial to general anesthesia were excluded.
Data collected perioperatively were age, gender, weight, height, ethnicity, and laterality of the procedure. The main endpoint was pain intensity at rest and in motion; secondary variables were postoperative use of opioids, nausea/vomiting, ambulation, and patient and surgeon satisfaction.
In the operating room, with the patient under vital sign monitoring and in the sitting position, asepsis, and antisepsis of the lumbar region was performed, followed by subaracnoid neuroaxial anesthesia using a Quincke 27 spinal needle, with 0.5% hyperbaric bupivacaine 15 mg, and no intrathecal opioids. Then, with the patient in supine position and following asepsis and antisepsis with 2% chlorhexidine, ultrasound (US) guided FNB was performed using a 100 mm Echogenic Needle Stimuplex® Manufacturer, B Braun. Bethlehem, 18018 Pennsylvania USA A echogenic needle (BRAUN) and a linear high-frequency transducer at an approximate depth of 1.5 to 2.5 cm. Plain 0.375% levobupivacaine 15 mL (56.25 mg) were administered, always with aspiration before giving the local anesthetic. Then, with the patient in supine position and in 45° of knee flexion, after 2% chlorhexidine asepsis and antisepsis, the IPACK block was applied scanning the popliteal fossa with a curved low-frequency transducer until femoral condyles were visualized at a depth of approximately 3.5 to 4.5 cm; the transducer was advanced cephalad until the condyles were out of view and the femoral axis came into view. At this point, a Stimuplex A, 100mm echogenic needle (BRAUN) was inserted in plane from anteromedial to posteromedial between the popliteal artery and the femur, until the tip of the needle was 1 to 2 cm from the lateral edge of the popliteal artery (Figs. 1 and 2). Plain 0.375% levobupivacaine 15 mL (56.25 mg) was injected under direct US visualization, always applying aspiration before administering the local anesthetic. The curved transducer was preferred not only because of depth penetration but also because it allows to visualize all the structures of the knee in a single window without having to slide the probe. All the procedures were performed by an experienced anesthetist. No issues with the femoral block were reported. Problems viewing the needle while performing the IPACK block were reported due to abundant adipose tissue in some patients, but they were solved adjusting US gain and depth.
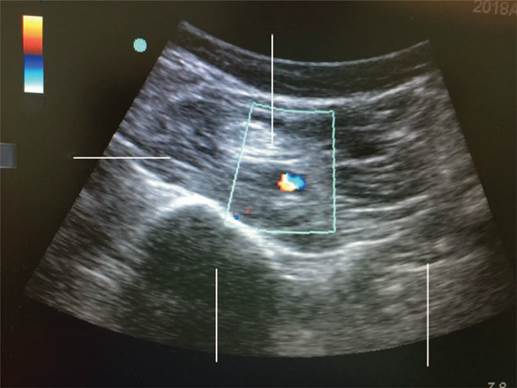
Source: Authors.
Figure 1 IPACK block ultrasound. Ultrasound image of in-plane needle insertion between the popliteal artery and the femur. FB = femoral biceps, NC = neurovascular component, IPACK=infiltration between popliteal artery and capsule of the knee, AS = acoustic shadow of the intercondylar line of the femur, SM=semimembranous.
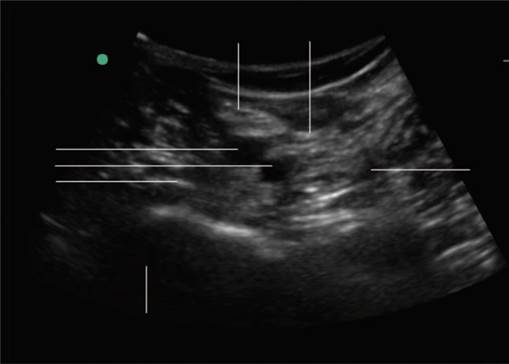
Source: Authors.
Figure 2 IPACK block ultrasound. A = artery, FB = femoral biceps, PN = peroneal nerve, TN=tibial nerve, AS = acoustic shadow of the intercondylar line of the femur, MS =semimembranous, V=vein.
Multimodal intravenous analgesia was given intra-operatively, consisting of dipyrone 1g, diclofenac 75 mg and dexamethasone 8 mg. All opioid administrations were documented at 6,12, 24, and 48hours and were converted into oral morphine equivalents for this study. Serial pain intensity assessments were made postoperatively at rest and with motion at 2, 4, 12, 24, and 48hours, using the verbal numerical scale. On this scale from 0 (no pain) to 10 (worst imaginable pain), patients reported their pain intensity verbally. At the time of the last assessment, a patient and surgeon satisfaction survey was conducted using the Likert scale from 0 to 5, where 5 is very satisfied and 0 is very dissatisfied. Ambulation within the first 24 hours and the presence of nausea/vomiting were also documented. Categorical variables are presented as counts and percentages, and continuous variables as medians and standard deviation.
Results
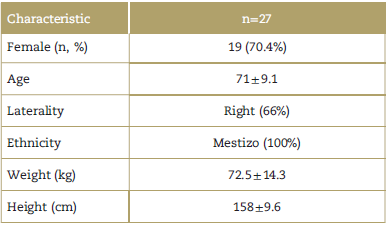
All patients (n = 27) who underwent primary unilateral TKA received subarachnoid neuroaxial anesthesia plus FNB combined with IPACK. Of the patients included in the study, 70% were women between 62 and 80 years of age. It was found that the majority of the TKA procedures were performed in the right knee. The demographic characteristics of the patients are shown in Table 1.
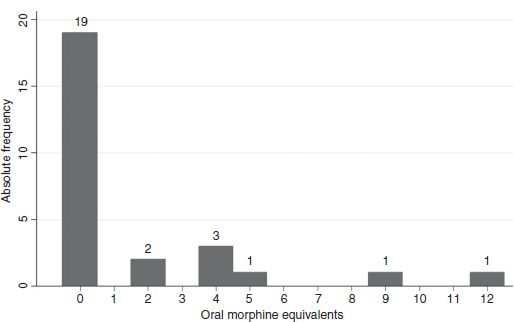
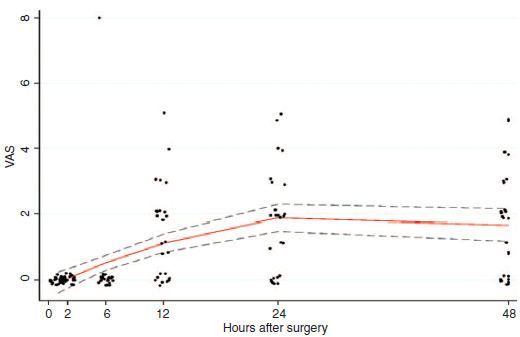
It was determined that 73% of patients did not require rescue opioids (95% confidence interval [CI] 52-88%). Opioid use remained low, at an average of 15.7 oral morphine equivalents during the 48-hour assessment period (minimum 6, maximum 36 OME) (Fig. 3). Table 2 shows pain intensity scores at rest and in motion, with mean values between 0 and 1; both at rest and in motion, the 2-hour pain score is 0, and maximum values are found at 48hours, with 0.78 ± 1.25 and 0.76 ± 1.61, respectively. Figure 4 shows postoperative scores on the visual numerical scale for pain in motion. Postoperative outcomes revealed that 100% of patients were satisfied with the surgery (95% CI 86-100). After the first 24hours, 81% (95% CI 60-93) were able to stand and walk with assistance. None of the patients experienced side effects from the anesthesia (nausea/vomiting).
Table 2 Postoperative pain scores on the visual numerical scale at rest and in motion after total knee arthroplasty.
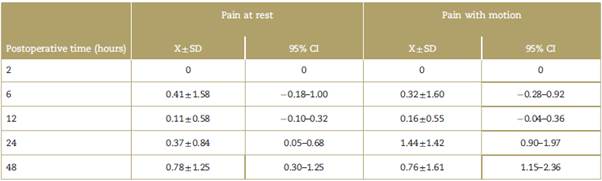
CI=confidence interval, SD = standard deviation, X=mean.
Source: Authors.
Discussion
TKA is a surgery associated with intense postoperative pain and up to 50% of patients need opioids or analgesics for adequate pain control to allow early ambulation and rehabilitation.6,11 In TKA, femoral and sciatic nerve blocks have been considered the gold standard for pain manage ment after the procedure; however, the sciatic nerve block may potentially result in drop foot and may also mask a surgically induced peroneal nerve injury in patients undergoing TKA.13 The IPACK block is a new technique for pain control in the posterior compartment of the knee, without the motor blockade associated with the sciatic nerve block, thus reducing length of stay and promoting faster recovery and postoperative patient rehabilitation.9,14
The results of this observational study showed that subarachnoid neuroaxial anesthesia combined with re gional analgesia in the form of a femoral block and IPACK, provided adequate analgesia during the first 48 hours following TKA. It was also shown to improve physical therapy yield, considering that mobility was achieved within 24hours in 81% of patients. None of the patients experienced anesthesia-related side effects. There were no episodes of nausea or vomiting possibly due to low opioid use.15 Patient and surgeon satisfaction was 100%.
The IPACK block is a technique described in 2014 which involves the infiltration of local anesthetic in the space between the popliteal artery and the posterior capsule of the knee,16 and offers an excellent alternative for pain control in the posterior compartment of the knee after arthroplasty; however, there is little evidence in the literature describing and comparing this novel regional block, and there are no publications in Colombia.
At present, the FNB is considered the gold standard for postoperative pain in TKA because of its efficacy and safety when used in association with intravenous analgesics such as opioids, non-steroidal anti-inflammatory agents, selective cyclooxygenase-2 inhibitors, and paracetamol in the context of multimodal postoperative pain management.17 The IPACK technique consists of US-guided administration of a local anesthetic to the space between the posterior capsule of the knee joint and the popliteal artery in order to block the genicular nerves (sciatic nerve branches), thus preventing distal motor deficit and drop foot, with no proximal sciatic nerve effect.18
The combination of different techniques (e.g., FNB+ IPACK, adductor canal + IPACK) in association with a multimodal analgesia regimen, often using opioids,19 appears to be the most promising option for pain management in patients taken to elective TKA, although there is little evidence supporting its systematic use.6,20 Selection of one or the other method must be based on the hospital context where anesthetists work, following the principles described above.
Drop foot and motor deficit in the affected limb have been reported with conventional regional analgesia techniques, resulting in difficult rehabilitation.19 This prompted the description in this research of a new regional analgesia technique for pain management in patients undergoing elective TKA. This technique was based on the combination of 2 types of blocks, namely, IPACK plus FNB, and subarachnoid neuroaxial anesthesia with 0.5% hyperbaric bupivacaine.
In a study of 106 patients taken to TKA using 3 different techniques (femoral block alone, FNB with IPACK and abductor canal block with IPACK and local infiltration), Thobhani et al10 found that the use of opioids was lower in patients in whom IPACK was performed, as a result of effective supplemental analgesia after TKA, as compared to the patients in the other groups.
Several studies have shown that IPACK in combination with another type of block provides better postoperative pain control in patients undergoing TKA.21-23 It has also been shown that in patients in whom a combination of blocks including IPACK was used, ambulation immediately after TKA was significantly better than in those in whom IPACK was not included.10,18,21
Considering the various mechanisms that influence increased postoperative pain in TKA, multimodal analge sia is found to be the ideal strategy-which reflects a multidisciplinary approach to the treatment of pain- designed to maximize the positive effects of the treatment while limiting adverse effects. This management must include subarachnoid neuroaxial anesthesia, FNB combined with IPACK, and intravenous analgesia with the use of opioids as needed.1,19,24 The addition of peripheral nerve blocks to the landscape of multimodal analgesia results in improved pain control, reduced stress response, and lower need for opioids,24 with the benefit of prolonged postoperative analgesia, less adverse effects, greater patient satisfaction, and faster functional recovery following TKA.25
Femoral and obturator nerve blocks do not cover the posterior capsule of the knee, while IPACK does so with lower motor impact during postoperative recovery; however, there is still no consensus regarding any anesthesia modality that may be considered better than the rest. On the other hand, the FNB has been associated with diminished quadriceps muscle strength, bringing its usefulness into question. The decision of using 1 type of anesthesia alone or in combination must be made based on the resources available in each health institution, with the aim of achieving adequate pain management, early rehabilitation and ambulation. The results of this study must be analyzed bearing in mind estimation uncertainties. However, the findings open the door to the perfor mance of controlled clinical trials to compare novel regional analgesia techniques such as the adductor canal block which, in theory, causes less quadriceps weakness associated with the IPACK bloc, and determine whether the results are comparable to the current standard of care based on femoral and sciatic nerve blocks.
Conclusion
In TKA, neuroaxial anesthesia associated with regional analgesia techniques that combine FNB and IPACK together with a multimodal intravenous regimen of limited opioid use, is the most promising option for adequate postoperative pain control, although there is little evidence supporting its systematic use. Therefore, the possibility exists of less motor blockade with the combined use of adductor canal block and IPACK, preserving long-term analgesic effect, and setting the basis for future research.

