











 texto en
texto en  Inglés (pdf)
Inglés (pdf)
 Articulo en XML
Articulo en XML Referencias del artículo
Referencias del artículo
 Enviar articulo por email
Enviar articulo por email Citado por SciELO
Citado por SciELO  Citado por Google
Citado por Google  Similares en
SciELO
Similares en
SciELO  Similares en Google
Similares en Google 
 Permalink
PermalinkIntroduction
Orthotopic liver transplantation (OLT) is a recognized intervention for patients with end-stage liver disease.1 However, this procedure is characterized by a high rate of bleeding and exposure to transfusions, due to its surgical complexity, the duration of the procedure, and the inherent characteristics of the recipient, such as malnutrition, thrombocytopenia, pre-operative anemia, and coagulopathy.2
The fact that Jehovah's Witnesses (JW) refuse heterologous blood transfusions as candidates for an OLT, involves a number of difficult changes for the teams and institutions responsible for the procedure.3 The biggest challenge may be ensuring strategies to reduce intraoperative bleeding (IOB), since there is sufficient evidence that IOB is a high-risk predictor for infection, multiple organ failure, and death.4,5
Materials and methods
Patients who were JW who had undergone OLT between July 2007 and August 2012 were identified. Each case was reviewed considering the cause of liver failure and recording various hematological parameters such as the level of hemoglobin, hematocrit, platelet count, and conventional hemostasis tests [prothrombin time and International Normalized Ratio (INR)] during the pre-operative, immediate postoperative, and 30 days after surgery. The quantity of fluids administered, IOB, volume recovered through cell salvage, duration of the procedure, and complications experienced over a 1-year follow-up, were also recorded.
Every patient signed an advance directive and a power of attorney indicating their refusal of blood transfusions. While in the waiting list, induced erythropoiesis and oral iron supplementation was administered in order to ensure levels of hemoglobin above 12g/dL. During the intraoperative period, hematology and hemostasis were assessed with sequential cell blood counts, thromboelastography (heparinase), and fibrinogen serum levels (Clauss method). The study was approved by the Biomedical Research Ethics Committee FVL (No. 365 of January 14, 2019).
Case series
The following information corresponds to details on the progress and management of the 4 subjects reported.
Case 1
A 56-year-old woman with a diagnosis of autoimmune cirrhosis, scored as Child-Pugh B at admission. There was no evidence of ascites or encephalopathy. Following the procedure, the patient was transferred to the intensive care unit (ICU), where she was extubated early, with no evidence of postoperative complications. In the second month posttransplant, the patient presented with elevated serum transaminases, and a liver biopsy was conducted. The biopsy showed signs of acute graft rejection and was managed with steroid pulses, resulting in a favorable response. A few weeks later, a new increase of transaminases (8-fold the normal value) was documented and the patient tested positive for cytomegalovirus infection (CMV-Ag). Valganciclovir was initiated with a favorable response to treatment and no further complications.
Case 2
A 55-year-old male with cryptogenic cirrhosis, classified as Child-Pugh B in terms of the severity of the disease. At admission, the patient presented with ascites, with no encephalopathy. During ICU stay, the patient presented with a torpid evolution due to surgical site infection, renal failure, and seizures associated to the use of cyclosporine and required levetiracetam, with no further relapses. Subsequently, the patient clinical condition progressively improved and he was discharged. During the first month after surgery, the patient experienced elevated trans-aminases up to 8-fold the normal level; a liver biopsy was conducted which evidenced mild acute graft rejection. The patient responded favorably to immunosuppressive therapy and a new control with biopsy at thirty days showed no evidence of rejection.
Case 3
A 41-year-old female with cirrhosis secondary to recurrent cholangitis and biliary stenosis; the patient had a hepatic jejunal anastomosis and billiar stent without improvement, requiring percutaneous transhepatic shunt. The severity of the disease classified as Child-Pugh B. During the initial ICU stay, the patient required vasoactive support and mechanical ventilation for a longer than usual period. Because of persistent fever, a extended spectrum beta lactamase (BLEE)-positive Escherichia coli bacteremia was identified, requiring antibiotic management with meropenem. The subsequent evolution was favorable and the patient could be discharged.
Two months after surgery, the patient experienced elevated transaminases and a liver biopsy was conducted, evidencing acute moderate graft rejection which was treated with steroid pulses. Six months after surgery, a colangiocarcinoma was identified, so cisplatin/gemcitabine management was initiated. As a result of the relapse and tumor progression, new chemotherapy regimens were required (oxaliplatin/capecitabine and placlitaxel). The patient had a 5-year survival after the original diagnosis.
Case 4
A 22-year-old female diagnosed with biliary cirrhosis secondary to biliary tract atresia. The patient had undergone choledocojejunostomy 57 days after birth. There was no evidence of ascites or encephalopathy at admission, and the severity of the disease was classified as Child-Pugh B. During her ICU stay she required nitro-prusside vasodilatory support because of poor blood pressure control and mechanical ventilation. The nitro-prusside infusion was discontinued after 2 days and the patient was weaned from the ventilator after 3 days. On the third postoperative day, the patient presented with elevated transaminases, prolongation of the conventional coagulation tests and portal flow alteration, suggestive of vascular graft dysfunction. The patient continued to deteriorate, with systemic compromise, acute renal failure, thrombocytopenia, hydroelectrolytic imbalance, and pulmonary dysfunction. On the 11th day after surgery, the patient continued to decline, developing multiple organ failure and disseminated intravascular coagulation and died on the same day.
Results
Global perioperative characteristics
Four OLTs were conducted in JW subjects. The mean age at the time of surgery was 42 years (range 22-55). End-stage liver disease diagnoses comprised autoimmune disease (n = 1), cryptogenic (n = 1), and sclerosing cholangitis (n = 2) (Table 1).
Table 1 Demographic characteristics of Jehovah's Witnesses undergoing orthotopic liver transplantation between July 2007 and August 2012.
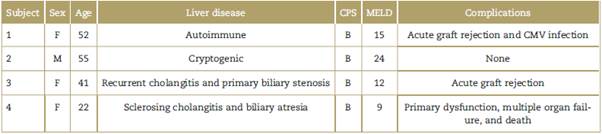
CMV=citomegalovirus, CPS=Child-Pugh Score, MELD=Model of end-stage liver disease.
Source: Authors.
The amount of intraoperative fluids in these patients was normal, as well as the retransfused volumes by cell salvage (average volume of 344mL [range 113-520]). The mean duration of the procedure was 343 min (range 330370), and the approximate amount of bleeding tended to be low as compared to the usual levels (average bleeding of 625 min [range 300-1000]) (Table 2).
Table 2 Fluids administered, approximate intraoperative bleeding, and volume recovered from cell salvage.
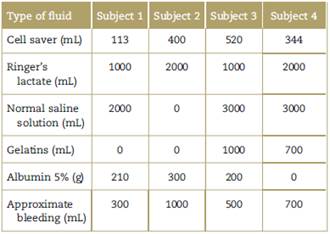
Source: Authors.
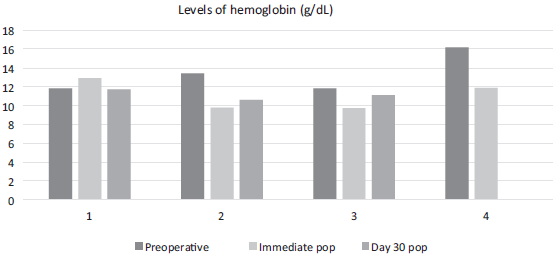
Before surgery the subjects exhibited average hemoglobin and hematocrit levels of 13.3 g/dL (range 11.8-16.2) and 40.1% (range 36.2-48.8), respectively. The average platelet count was 225,000/µL (range 93,000-363,000) and the mean INR was 1.25 (range 1.06-1.53). These levels were maintained within very similar ranges until day 30 after surgery (Table 3). When specifically analyzing the evolution of the hemoglobin levels, all subjects maintained levels above 9 g/dL during the study period (Fig. 1)(Table 3).
Table 3 Mean hematological tests during the perioperative of Jehovah's Witnesses undergoing orthotopic liver transplantation between July 2007 and August 2012.
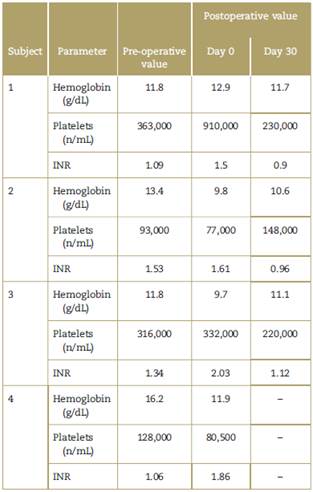
INR=International normalized ratio.
Source: Authors.
Source: Authors.
Figure 1 Hemoglobin levels during the pre- and postoperative in Jehovah's Witnesses undergoing orthoptopic liver transplantation between July 2007 and August 2012.
During the follow-up, 3 patients survived over 1 year and all of them presented early episodes of immune graft rejection, but responded satisfactorily to immunosuppressive therapy. One of them presented with vascular dysfunction of the graft and early death.
Discussion
This retrospective series shows the experience and out-comes of a referral center of JW patients with end-stage liver disease undergoing OLT. Our data show that under current hospital care conditions, it is possible to perform these high complexity procedures that involve a high risk of exposure to blood products in patients who refuse allogeneic transfusions, with a high probability of success.
Several publications have shown a trend to considerably reduce the average number of blood product units transfused in OLT subjects. This behavior is due to the implementation of improved surgical strategies aimed at preserving blood volume and a more effective pre-operative optimization that includes intervention of anemia and secondary hemostasis disorders.6 Similar series of JW patients undergoing OLT and other surgical procedures with a high risk of bleeding, reporting high success rates and low rates of complications have been previously published. Recently, the introduction of the concept "patient blood management" (PBM), which includes the perioperative intervention of the red cell mass and other bleeding-associated conditions, has proven its non-inferiority to the liberal use of allogeneic blood products, with a subsequent reduction in costs and transfusion-associated adverse events.7,8
When analyzing our series of patients, all of them were taken to the procedure in the best possible conditions, as shown by hematocrit levels >35% and a lower level of systemic compromise at admission (low MELD scores). To achieve these preoperative goals, an interdisciplinary management was required, intended to improve the general conditions of the underlying disease. According to Thompson et al, his approach has been associated with a low risk of bleeding.9 There have been a number of publications showing the benefits of optimizing the hemoglobin levels before undergoing major surgery.10,11
Our work also shows that the management of blood-sparing intraoperative techniques such as cell salvage, the use of specific tests to assess functional hemostasis, limited use of fluids, and the use of tranexamic acid,12 contributed to reduce the overall bleeding rates. These rates were even lower than those reported by Jeong et al.13 In addition, none of the patients experienced a significant drop in hemoglobin below 9 g/dL during the first month after surgery.
It is noteworthy that most of our patients experienced acute graft rejection, and this may be related to a higher stimulus of the innate immunity as a result of the non-utilization of allogeneic blood products, which have been associated with immunomodulation and immunosuppression.14 Since there is no inhibition of the activity of macrophages and dendritic cells, or cytotoxic anti-human leukocyte antigens (HLA) transfusion-mediated response, these individuals could have expressed an earlier and increased immune response to the graft.15,16
Considering the limited and retrospective nature of the data herein discussed, there may be some concerns regarding to potential bias or overestimation of treatments. However we believe that this is the first publication in Colombia presenting a series of JW patients undergoing OLT. Our results are similar to those of previous studies17,18 reaffirming the feasibility of this procedure for patients who refuse to receive blood transfusions. Any group wanting to include JW in their waiting lists for OLT, should consider the pre-operative implications herein discussed, strengthen their communication with other support specialists involved in the preoperative optimization, and develop a carefully designed perioperative plan that covers the clinical, ethical, and legal aspects involved in the care of these patients.
Conclusion
Significant progress made in terms of optimization and perioperative care, makes it possible to offer OLT as an option for JW with end-stage liver disease. It requires a surgical team that understands the importance of achieving the best possible clinical conditions before the procedure, and of an efficient multidisciplinary interaction aimed to respect the wish of these patients of not being transfused but to do it in a safe and controlled manner to avoid unnecessary high risk. To achieve the best possible results, implicated teams must be committed with the implementation of surgical, pharmacological and non-pharmacologic strategies intended to preserve the patient's own blood, going hand in hand with the PBM initiative, in the quest for the efficient use of healthcare resources and patient wishes-centered care.
Ethical responsibilities
Protection of human beings and animals. The authors declare that the procedures used in this study followed the ethical standards for experimentation in humans and were consistent with the Medical World Association and the Declaration of Helsinki.
Confidentiality of the data. The authors declare that they have followed the protocols and processes needed to protect the identity of the subjects.
Right to privacy and informed consent. The authors obtained the corresponding ethical authorizations to extract the necessary information to prepare this paper and maintained the privacy of the subjects involved. The document is under custody of the corresponding author.

