











 text in
text in  English (pdf)
English (pdf)
 Article in xml format
Article in xml format Article references
Article references
 Send this article by e-mail
Send this article by e-mail Cited by SciELO
Cited by SciELO  Cited by Google
Cited by Google  Similars in
SciELO
Similars in
SciELO  Similars in Google
Similars in Google 
 Permalink
PermalinkIntroduction
The classical definition of a difficult airway (DA) of the American Society of Anesthesiologists is the clinical situation in which a conventionally trained anesthetist has difficulty ventilating the patient with a facial mask, tracheal intubation, or both.1 When it is identified before induction, it is classified as anticipated DA (ADA) and it constitutes a scenario of great concern in the practice of anesthesia because of its association with high morbidity and mortality in failure cases.2
There is agreement as to the standard of care for this situation, consisting of management of the airway with the patient awake or on spontaneous ventilation,3 mainly in the trauma setting4,5 and in critically ill patients.6,7 Although recognized as versatile alternative tools, flexible fibroscopy, and videoendoscopy intubation may fail.
There is a paucity of evidence regarding rescue video-laryngoscopy in the setting of ADA. Only a combined approach using fibrolaryngoscopy and videolaryngoscopy is described in the setting of blunt airway trauma.8 We report 7 cases in which rescue angled blade videolaryngoscopy was used successfully following failed flexible fibroscopy in awake patients with ADA.
Clinical cases
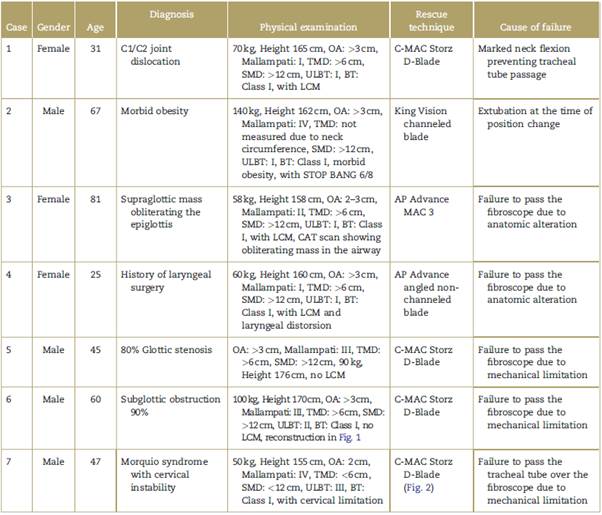
All the cases included in this report were diagnosed as ADA and subjected to awake intubation with flexible fibroscopy. Sedation was based on titrated doses of remifentanil between 0.1 and 0.3 µg/kg/min, associated with a spray as you go technique with 2% lidocaine instillation through the working channel with doses ranging between 200 and 450mg and topical application of 50 mg of oxymetazoline through both nostrils, plus local anesthetic applied on the anatomical fibroscope entry site (oropharynx or nasopharynx with 10% lidocaine spray).
Table 1 shows a summary of the baseline characteristics of the patients and the rescue technique following failed fibroscopy.
Discussion
Patients with DA are one of the biggest challenges for the anesthetist. Access to airway in the awake patient using techniques such as fiberoptic bronchoscopy (FOB) has been recognized as the gold standard for the management of patients with ADA, it being the most studied and recommended option.2,9 However, there are downsides to this technique, including the training required, the skills needed to identify airway structures, cost, the need for frequent maintenance, and the fragility of the equipment.
Failure has been reported in conditions such as obstruction for nasal passage, posterior pharyngeal wall tumors, presence of blood and secretions, airway trauma, complete airway obstruction, distorted anatomy, or technical limitations preventing access to the glottic cavity with the endotracheal tube.10-13 These situations require immediate change of plan to establish access for intubation.14
Alternative plans described include translaryngeal accesses for rescue, although those techniques may have limitations due to lack of anesthetist experience, morbidity, late complications, and the time required to perform them. Reported success of the translaryngeal access performed by anesthetists in emergency situations is quite low, and it is accomplished in only 36% of the procedures. Series like the National Audit Proyect 4 report a failure rate as high as 60%.15 For this reason, the open technique suggested by the Difficult Airway Society is recommended at present, using scalpel blade, bougie, and a No. 6.0 endotracheal tube; it requires less training and shorter performance time, and success rates are higher.16
Likewise, other alternative anesthetic options after failed fiber-optic intubation are described, including blind intubation through supraglottic intubation devices, guide wire-aided blind intubation, and videolaryngoscopy. Over the last few years, the latter technique has gained acceptance for ADA patients, with results equivalent to those obtained with fibroscopy techniques, offering the possibility of securing the airway faster. It is estimated that an anesthetist must perform 25 intubations with FOB to acquire a basic learning curve compared to only 1 to 6 video laryngoscopy (VL) intubations to achieve the same skill level.17
In 2018, a meta-analysis of 429 patients compared VL vs FOB for awake intubation. This study showed shorter intubation time using the VL technique (45 seconds) as compared to FOB, but no differences in term of overall success rates, patient satisfaction, or adverse effects with the 2 strategies.17
Awake fibroscopy failure and loss of a previously secured airway by trained personnel are rare. The 7 cases presented here represent 0.76% of patients seen by the airway team at Universidad de Antioquia (921) over the past 3 years.
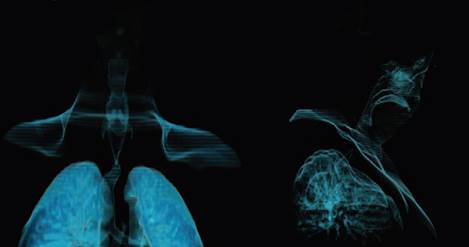
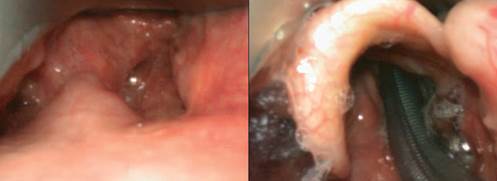
The causes of failure are summarized in Table 1. The authors believe that they were due to mechanical limitations associated with the anterior curvature (cases 3, 4, 5, 6, and 7) (Fig. 1). All of these were solved using VL, allowing glottic aperture and reducing neck flexion curvature (Fig. 2). On the other hand, given that tracheal tube insertion in videolaringoscopy is separate from visualization (non-channeled blades), tracheal tubes of different sizes may be readily exchanged, unlike what happens with the fibroscopy technique which requires new exploration with every change of tube size.
Source: Authors.
Figure 1 Three-dimensional reconstruction of the airway (case 6 with 90% subglottic stenosis).
Source: Authors.
Figure 2 Rescue with D-Blade videolaryngoscopy in patients with de Morquio syndrome.
Since VL intubation time is shorter than with fibroscopy -reported as at least 10 minutes in expert hands-VL may offer more successful rescue in cases of extubation due to position changes or inadequate fixation (case 2).
Conclusion
The conclusion of this case series is that VL could be a great option in ADA for awake intubation following failed FOB intubation. Advantages previously reported for VL are highlighted, including improved visual field, the ability to use different tubes and exchange them during the procedure without losing visualization, faster tracheal tube exchanges, as well as tissue traction which increases glottic aperture in cases of abnormal airway anatomy.
Our study is limited in that it is a case series; however, it is considered novel given that fibroscopy failure in expert hands is infrequent. We believe that anesthetists must train in the use of videolaryngoscopy in ADA, and prepare clear plans before approaching complex patients, thus improving safety in anesthesia.
Finally, further studies are warranted in ADA in order to determine which type of videolaringoscope is the most suitable in this context and when it should be used as the first choice, even before, or together with, flexible fibroscopy.
Ethical responsibilities
Human and animal protection: The authors declare that all the procedures were performed in accordance with the ethical standards of the responsible human experimentation committee, and the World Medical Association and the Declaration of Helsinki.
Data confidentiality: The authors declare that they followed the protocols of their center of practice regarding disclosure of patient data.
Right to privacy and informed consent: The authors declare that they obtained informed consents from the patients and/or subjects mentioned in the article. The relevant documents are kept by the corresponding author.
Each of the participants were informed before the procedure was carried out in relation to the alternatives and difficult airway devices including their risks, benefits and the need to perform such approaches under grade I sedation. Each of them filled out the informed consent of the difficult airway group of the Universidad de Antioquia prior to the anesthetic procedure. Document is attached. No other resolutions or approvals were required as it was a case series review, where clinical plans were based on international scientific recommendations without the need to intervene in other options than those established in the literature.

