











 text in
text in  English (pdf)
English (pdf)
 Article in xml format
Article in xml format Article references
Article references
 Send this article by e-mail
Send this article by e-mail Cited by SciELO
Cited by SciELO  Cited by Google
Cited by Google  Similars in
SciELO
Similars in
SciELO  Similars in Google
Similars in Google 
 Permalink
PermalinkIntroduction
The main causes of death in trauma patients during the first 24hours are exsanguination and central nervous system (CNS) injuries. Whenever there massive bleeding involving the CNS, mortality rises to 50% within the first hour.1 Bleeding results in important physiological changes that may even lead to the lethal triad of acidosis, hypothermia, and coagulopathy.2 Coagulation disorders are an independent factor for mortality3 accounting for 30% of the deaths of civilian trauma patients.4 The initial treatment of trauma patients requires surgical damage control and management of the hemorrhagic shock, in order to reduce blood loss to the minimum and restore tissue perfusion.5 These interventions include minimizing the use of crystalloids to prevent organ dysfunction associated with fluid overload-such as dilutional coagul opathy-and early use of blood products.6 These measures are resuscitation with damage control, intended to perform a hemostatic resuscitation to prevent death from exsanguination.7 In trauma patients requiring massive transfusion, the fresh frozen plasma (FFP) to platelets and red blood cells (RBCs) ratio has been studied, which provides the best protective effect. Consequently, there is an increasing number of trials assessing the impact of the FFP:RBC ratio on outcomes such as mortality or multiple organ failure, with controversial results.
Since 2005, the United States Army's Institute of Surgical Research Conference suggested the administra tion of a high ratio (1:1:1) instead of a low ratio (1:1:2).8 Later on, the Prospective, observational, multicenter, major trauma transfusion trial (PROMMTT)9 found that the administration of blood products with a high FFP:RBC ratio was associated with decreased mortality during the first 6 hours after the trauma event. In contrast, the clinical trial Transfusion of plasma, platelets, and red blood cells in a 1:1:1 vs a 1:1:2 ratio and mortality in patients with severe trauma (PROPPR),10,11 did not find any mortality reduction at 24 hours and at 30 days; however, there was a lower risk of early death due to exsanguination in patients treated with a high ratio. Moreover, some trials have reported an increase in the number of pulmonary complications and multiple organ failure with a higher FFP input.12,13
Notwithstanding, the consensus to intervene early in coagulopathy, with limited crystalloid use and early treatment with blood products,14 it is not clear however about which plasma: RBC ratio provides the best outcomes. Some observational studies and clinical experiments have compared different FFP:RBC ratios with varying results, attributable to differences in the definition of massive bleeding, early exclusion of deceased patients, and interventions at different time periods.15,16
The objective of this systematic review was to assess the impact on early and late mortality of the administration of high vs low FFP:RBC, in patients with civilian trauma massive bleeding, and to determine the sources of heterogeneity of the trials.
Methodology
Selection of trials
A systematic literature review was conducted to identify observational studies and clinical controlled trials that addressed the research question, with no language restrictions. The PRISMA (Preferred Reporting Items for Systematic reviews and Meta-Analyses) recommendations were followed.17 The systematic review protocol was previously registered in PROSPERO (Record ID 111387).
The quality of the observational studies was assessed with the Newcastle-Ottawa scale (NOS),18 and in the case of clinical experiments, the Cochrane collaboration instruc tions were adopted.19 In order to identify the studies, the following e-databases were consulted, between the first week of 1990 and week 40 of 2019: MEDLINE, MEDLINE In-Process & Other Non-Indexed Citations, MEDLINE Daily Update, Embase, PsycINFO, and Lilacs, using the following search strategy: (trauma OR traumatic OR injur* OR wound*) AND (massive OR major) AND (haemorrhag* OR hemorrhag* OR bleed* ORtransfus* ORblood) AND (plasma OR component) AND (mortal* OR death* OR die OR died). In addition, the structured filters validated for observational studies of the Scottish Intercollegiate Guidelines Network were used, and for controlled clinical trials. The search was manually complemented with the snowball strategy and gray literature search using OpenGrey.
Inclusion criteria for the studies in this review
The studies that met the following criteria were included: clinical controlled trials or observational cohort, case controlled, studies that should include civilian trauma patients, report the FFP:RBC ratio admin istered, assess the mortality outcome, and embrace the previously established massive transfusion definition of ≥ 10 units in 24 hours, ≥ 6 units in 12 hours, or ≥ 5 units in 4 hours.20
Exclusion criteria for the studies
Any studies with the following characteristics were excluded: (a) studies such as case reports or case series; (b) studies using a historical cohort as the comparator; (c) studies that failed to consider the severity of the patients using scales such as the Injury Severity Score (ISS); and (d) studies, including patients with war or military trauma, or that included patients undergoing pro grammed surgeries.
Data mining
From each study, the information collected included the FFP:RBC ratio used for each one of the comparator groups, the mean age, the severity assessed with the ISS score, and in terms outcomes, mortality at 6,12, and 24 hours and at 30 days after hospital discharge. Two reviewers (HO, DM) independently checked all the abstracts, taking the exclu sion and inclusion criteria into account. Any differences among the studies selected were identified and reconciled, and the studies were independently reviewed as full texts.
Statistical analysis
The quality of the selected observational studies was assessed using the NOS scale,18 and in the case of clinical experiments, the Cochrane collaboration instructions were followed.19 Two reviewers (HO, DM) independently assigned a quality score and settled any disagreements by consensus. High-quality studies were those that obtained 7 or more points in NOS. The heterogeneity of the studies was assessed using the Q of Cochran, the I2, and the Tau index; high heterogeneity was considered as I2 > 50%. The odds ratio (OR) was measured in each study, with their corresponding confidence intervals (CIs). Mortality before 24hours was considered early and at 30 days late. The FFP: RBC ratio used was taken into account both in the intervention and in the comparator, and the accepted high ratio was that defined for each study. A 1:1 ratio represented the same number of units of FFP and RBC; in contrast, a 1:2 meant twice the amount of RBC per FFP unit, and this latter one was a lower ratio. For the combination of early and late mortality outcomes, it was stratified in accordance with the exclusion of deceased patients at 6, 12, and 24hours, in order to assess the differential opportunity to receive therapy for survival. The OR values were obtained for each summary measurement through the fixed effects models of the Mantel and Hansen model; the random effects model by inverse variance, charts, and analyses were conducted using the statistical software STATA 15.0 (StataCorp, College Station, TX).
Results
General findings and quality assessment of the trials
With the search strategy, 1295 studies were identified and 74 of them were selected based on title and abstract; 25 failed to meet the inclusion criteria and an additional 16 were excluded due to various reasons; finally, 33 studies were included for analysis (Fig. 1).
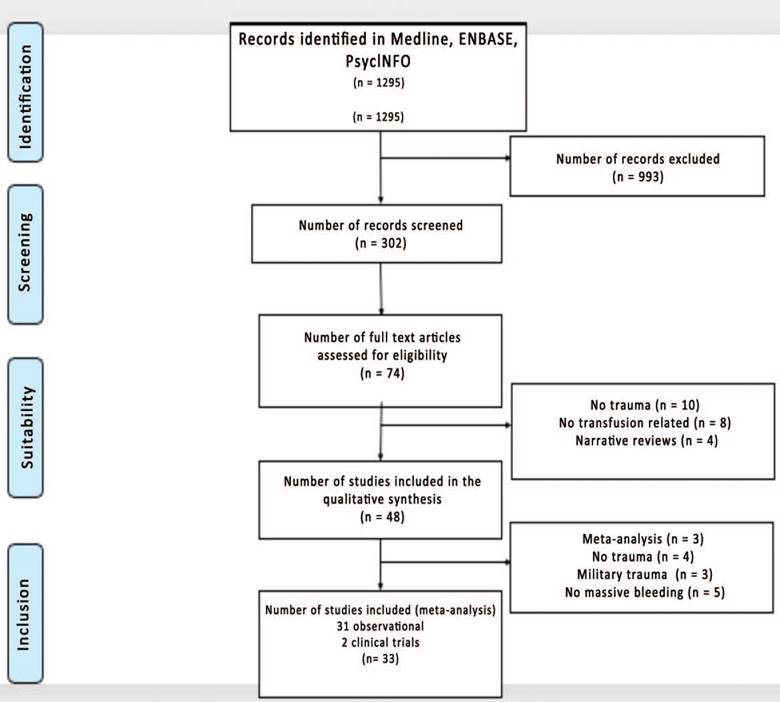
Source. Authors.
Figure 1 Flowchart identification and selection of the trials that met the inclusion criteria.
Of the studies included, 22 reported mortality in the first 24hours; in other 22, death was reported at 30 days, and 15 studies reported both outcomes. Most of the studies established as high FFP:RBC ratio cut points above 1:1.5 and 1:2. The quality of the observational studies assessed using NOS18 was three points for only one study.21 The rest had scores between 6 and 9, which translates into adequate-good quality. The risk of bias was low in the clinical experiments (Table 1).
Table 1 Overall characteristics of the studies.
| Reference | Outcome mortality | n | Age | ISS | High ratio | Odds ratio CI (95%) | Quality Newcastle- Ottawa (18) | |
| Holcomb et al22 | 30 days | 418 | 39 | 33 | 1:2 | 1.99 | (1.32-2.98) | 8 |
| 24 hours | 418 | 39 | 33 | 1:2 | 1.81 | (0.16-2.81) | 8 | |
| Sperry et al23 | 30 days | 415 | 41 | 34 | 1:1.5 | 0.73 | (0.45-1.20) | 8 |
| 12 hours | 415 | 41 | 34 | 1:1.5 | 0.28 | (0.10-0.80) | 8 | |
| Duchesne et al24 | 24 hours | 135 | 33 | 27 | 1:1 | 0.05 | (0.02-0.13) | 8 |
| Maegele et al25 | 30 days | 713 | 41 | 41 | 1:1 | 0.51 | (0.36-0.71) | 8 |
| 24 hours | 713 | 41 | 41 | 1:1 | 0.34 | (0.22-0.41) | 8 | |
| Gunter et al26 | 30 days | 259 | 34 | 25 | 2:3 | 0.43 | (0.24-0.76) | 6 |
| Kashuk et al27 | 24 hours | 140 | 35 | 36 | 1:2 | 0.54 | (0.27-1.06) | 6 |
| Teixeira et al28 | 30 days | 383 | 32 | 31 | 1:2 | 0.37 | (0.26-0.60) | 7 |
| Snyder et al29 | 24 hours | 134 | 39 | 33 | 1:2 | 0.48 | (0.24-0.96) | 7 |
| Dente et al30 | 30 days | 73 | 35 | 29 | 1:1 | 0.56 | (0.20-1.55) | 6 |
| 24 hours | 73 | 35 | 29 | 1:1 | 0.37 | (0.11-1.23) | 6 | |
| Zink et al31 | 30 days | 452 | 33 | 31 | 1:1 | 0.43 | (0.22-0.83) | 6 |
| 6 hours | 452 | 33 | 31 | 1:1 | 0.07 | (0.01-0.55) | 6 | |
| Mitra et al32 | 30 days | 331 | 42 | 36 | 1:1.5 | 0.93 | (0.49-1.74) | 9 |
| 4 hours | 331 | 42 | 36 | 1:1.5 | 0.32 | (0.10-1.08) | 9 | |
| Shaz et al33 | 30 days | 190 | 37 | 27 | 1:2 | 1.18 | (0.66-2.10) | 6 |
| 24 hours | 190 | 37 | 27 | 1:2 | 1.8 | (0.92-3.54) | 6 | |
| Lustenberger et al34 | 24 hours | 229 | 40 | 37 | 1:1.5 | 0.08 | (0.04-0.16) | 7 |
| Spoerke et al35 | 30 days | 529 | NA | NA | 1:4 | 0.39 | (0.25-0.62) | 7 |
| 24 hours | 529 | NA | NA | 1:4 | 0.29 | (0.16-0.52) | 7 | |
| Rowell et al36 | 30 days | 704 | 40 | 32 | 1:2 | 0.71 | (0.53-0.96) | 9 |
| 24 hours | 704 | 40 | NA | 1:2 | 0.54 | (0.38-0.76) | 9 | |
| Peiniger et al37 | 30 days | 1250 | 41.8 | 42 | 1:2 | 2.11 | (1.65-2.69) | 9 |
| 24 hours | 1250 | 41.8 | 42 | 1:2 | 3.29 | (2.52-4.29) | 9 | |
| Magnotti et al38 | 24 hours | 103 | 38 | 32 | 1:2 | 0.39 | (0.17-0.89) | 7 |
| Borgman et al39 | 30 days | 659 | 43 | 34 | 1:2 | 0.61 | (0.44-0.85) | 8 |
| 24 hours | 659 | 43 | 34 | 1:2 | 0.47 | (0.33-0.68) | 8 | |
| Biasi et al40 | 24 hours | 393 | 39 | 32 | 1:3 | 1.54 | (0.93-2.54) | 6 |
| Spinella et al41 | 30 days | 461 | 38 | 40 | 1:2 | 0.74 | (0.40-1.35) | 6 |
| Wafaisade et al42 | 30 days | 1362 | 45 | 36 | 1:1 | 0.66 | (0.51-0.85) | 8 |
| 24 hours | 1362 | 45 | 36 | 1:1 | 0.51 | (0.36-0.73) | 8 | |
| Brown et al43 | 6 hours | 604 | 43 | 37 | 1:1.5 | 0.37 | (0.14-0.95) | 6 |
| Sharpe et al44 | 30 days | 135 | 37 | 32 | 1:1.5 | 0.46 | (0.23-0.94) | 7 |
| Duchesne et al45 | 24 hours | 451 | 38 | 23 | 1:2 | 0.38 | (0.22-0.65) | 9 |
| Simms et al46 | 3 hours | 151 | 33 | 29 | 1:1.4 | 0.19 | (0.08-0.45) | 6 |
| Guidry et al47 | 6 hours | 234 | 35 | 25 | 1:2 | 0.63 | (0.35-1.14) | 9 |
| Nascimento et al48 | 30 days | 69 | 41 | 35 | 1:1 | 4 | (1.03-16.3) | ∗ |
| Kudo et al49 | 30 days | 15 | 60 | 25 | 1:1.5 | 0.8 | (0.10-6.35) | 7 |
| 6 hours | 15 | 60 | 25 | 1:1.5 | 1 | (0.11-8.95) | 7 | |
| Kim et al50 | 30 days | 100 | 47 | 32 | 1:2 | 0.61 | (0.26-1.46) | 8 |
| 24 hours | 100 | 47 | 32 | 1:2 | 0.08 | (0.02-0.39) | 8 | |
| Rubén Peralta et al21 | 30 days | 77 | 34 | 29 | 1:1.5 | 0.2 | (0.07-0.55) | 3 |
| 24 hours | 77 | 34 | 29 | 1:1.5 | 0.15 | (0.05-0.45) | 3 | |
| Stanworth et al51 | 24 hours | 298 | 38 | 28 | 1:2 | 0.35 | (0.19-0.65) | 9 |
| Holcomb et al11 | 30 days | 680 | 34 | 26 | 1:1 | 0.81 | (0.57-1.15) | * |
| 24 hours | 680 | 34 | 26 | 1:1 | 0.71 | (0.47-1.09) | ∗ | |
| Endo et al52 | 30 days | 1777 | NA | NA | 1:1.25 | 0.85 | (0.60-1.21) | 8 |
* RCT = randomized controlled trials.
Source: Authors.
Summary measurements of mortality assessment
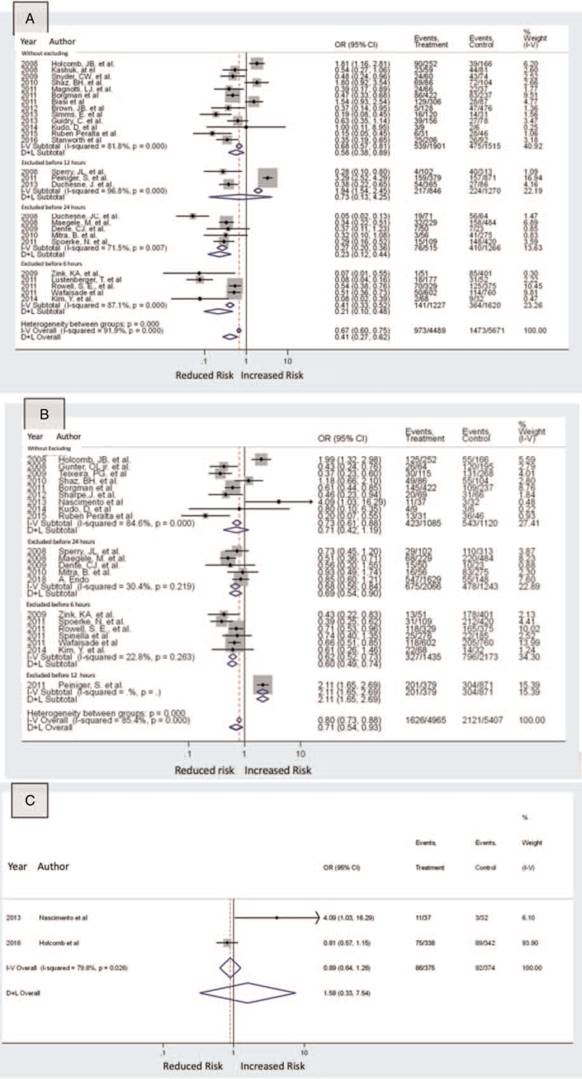
When analyzing the 31 observational studies (n = 13924), the use of a high FFP:RBC ratio was associated with lower early mortality (OR 0.67; 95% CI, 0.60-0.75) and late (OR 0.79; 95% CI, 0.71-0.87), but with a significant heterogeneity for both estimates, with an I2 of 91.9% and 86.3%, respectively. There were no differences between the groups when assessing the clinical (n =749) (OR 0,89; 95% CI, 0.64-1.26) and the heterogeneity was high (I2 79.8%). The observational studies took into account the potential differences due to the exclusion of deceased patients over the first 24hours following admission, and hence the summary measurements were stratified (6,12, and 24 hours and studies that did not exclude the deceased patients). The result was that by not excluding the death over the first 24hours, the protective effect on early mortality was maintained (OR 0.58; 95% CI, 0.38-0.89), but that was not the case for late mortality (OR 0.72; 95% CI, 0.46-1.11) (Fig. 2).
Heterogeneity assessment
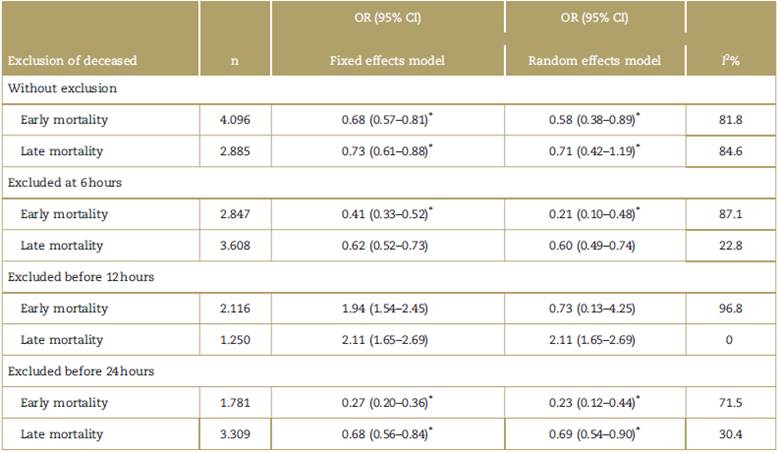
As shown in Table 2, when mortality was stratified in accordance with the exclusion of deceased patients at 6,12, and 24hours, the heterogeneity decreased in all categories as compared against the global I2. Additional stratifications were conducted, keeping in mind the time at which the transfusion was initiated (4,6,12, and 24hours); no reduced heterogeneity was observed in the studies.
Meta-regression
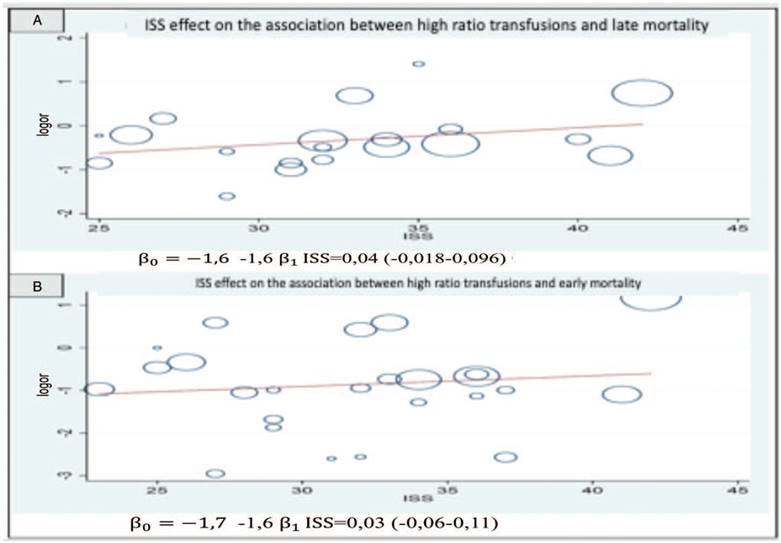
To assess the ISS and age with the association between high FFP:RBC and early and late mortality, a meta-regression was conducted using the random effects model. As shown in Fig. 3, as the ISS value increases, the strength of the association between a high FFP:RBC ratio and mortality reduction. This can be inferred from the value of the slope ß0 = 1.6 for early mortality and ß0 = 1.7 for late mortality. However, the CIs are wide and contain the zero value.
Publications bias
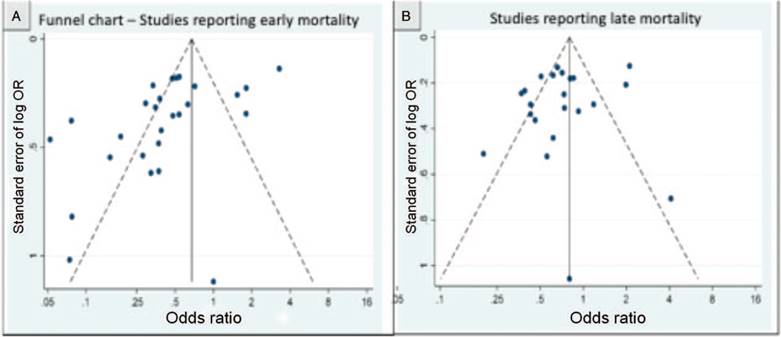
The publication bias assessment used the funnel chart and Egger's test to determine the asymmetry via lineal regression. An asymmetry was found mainly for the studies that assessed the late mortality outcome. This asymmetry could be due to a very high heterogeneity, to the quality differences and to the size of the trials (Fig. 4).
Discussion
In this meta-analysis, the use of a high FFP:RBC ratio in civilian trauma patients and massive transfusion was associated with a lower mortality risk over the first 34 hours to 30 days when the observational studies were evaluated. There were no significant differences when conducting clinical experiments. When the outcome was stratified based on the exclusion of deceased patients over the first 24 hours, the protective effect was maintained only for early mortality but not for late mortality; this may be due to the survival bias. Furthermore, the ISS changed the association between a high FFP:RBC ratio and mortality, being lower when the ISS was high.
Resuscitation of severe trauma patients and major bleeding has experienced significant changes, including the restricted use of crystalloids, surgical damage control, and balanced ratio transfusions, that are intended to match the total blood, an approach known as damage control resuscitation.53 This particular strategy has been associated with lower requirements of blood products, decreased inflammation, and probably improved survival.
Despite all of these, the ideal FFP:RBC ratio is still controversial. The literature published between 2007 and 2015, based on observational studies, found that high ratios have a protective effect on mortality and hence the scientific associations issue recommendations based on this guideline.54 However, these studies must be inter preted with caution because of their design. Rahouma et al15 suggest some limitations with regards to the survival bias because several studies ignored the exact time of the blood products transfusion; hence, it might be possible that balanced ratios (high) could have been administered to the patients who survived the first hours, that is, the less severe. Our meta-analysis supports the possibility of survival bias in the observational studies, because when the outcomes were stratified in accordance with the exclusion of deceased patients over the first 24 hours, the early mortality protective effect declined and was non-existent for the late mortality.
There are other potential variables apart from the FFP: RBC ratio that may influence the mortality outcome; for instance, the early and timely administration of blood products (FFP in particular). So only by improving the transfusion protocol for patients with massive bleeding, has it been possible to report decreases in mortality from 45% to 19%.55 These appreciations were tested in a clinical experiment. Holcomb et al in the PROPPR trial10,11 found no significant differences in mortality at 24 hours and 30 days, though homeostasis was achieved faster and there were less deaths as a result of exsanguination in the group treated with a high ratio. Moreover, the authors claim that about 15% of the deaths were due to traumatic brain injury, which could have contributed to the absence of differences.
The PROPPR trial11 also showed that the administra tion of higher than 1:1 ratio had no additional benefiting mortality, which is a consistent finding with the result of this meta-analysis, since we stratified based on different FFP:RBC ratios, we did not identify that as a source of heterogeneity. With regards to other sources of heterogeneity suggested by other authors, such as time of initiation of the administration of blood products,56 the total number of units transfused, and the amount of crystalloids administered,44,57 these became study limitations and made it impossible to stratify based on these variables because they were not reported.
Our study has its limitations. First, the volume of crystalloids administered over the first few hours is unknown and this is a risk factor for coagulopathy and death;52,58 however, this is a limitation typical of individual studies, since these variables are not reported. Neither is the use of other interventions assessed, such as cryoprecipitates, prothrombin complex concentrate, fibrinogen concentrates, and tranexamic acid. Moreover, the definition of massive transfusion includes a very long period of observation (up to 24hours), which could delay the onset of adequate therapy and favor the survival bias. This has shorten the time to diagnosis of MT to just a few hours (critical threshold for the administration of three units in one hour)59,60 and to adopt massive bleeding prediction models such as: modified shock index,61 Assessment of Blood Consumption score ABC62 Trauma Associated Severe Hemorrhage Score TASH,63 Schreiber Score64 Emergency Transfusion Score ETS,65 and the Prince of Wales Hospital Score PWH.66 The final goal of this reasoning is to reduce the observation period and start hemostatic resuscitation early.63
Although the right blood products ratio continues to be a valid query, its generalized use has been questioned, because of the risk of acute pulmonary injury and multiple organ failure. Along these lines, the proposal is to individualize treatment and direct transfusion support based on a therapy guided by objectives, aimed at achieving normal hemostasis, since it has been able to reduce bleeding, decrease the amount of blood products used, and improve other outcomes.67 To this end, "bedside" coagulation tests are conducted with viscoelastic methods (VEM) and based on the results, the specific blood products used are determined. Some authors suggest a mixed strategy that comprises transfusion therapy with high ratio during the early massive bleeding, and then make some adjustments in accordance with a VEM algorithm (thromboelastography or thromboelastometry).68
Conclusion
The use of high FFP:RBC ratio in civilian trauma patients and massive transfusion was associated with a lower mortality risk in the first 24 hours and at 30 days when the observational trials were assessed. There were no signifi cant differences when analyzing the clinical experiments. When the outcomes were stratified in accordance with the exclusion of deceased patients over the first 24hours, a protective effect was maintained only for early mortality, with no differences in late mortality. The studies identified showed an increased heterogeneity resulting from multi ple sources; one of the most relevant ones was the exclusion of patients who die early, before the first 24 hours after the trauma event, which represents a survival bias. Other sources of heterogeneity, such as the severity of the trauma, changed the use of blood products and mortality, as evidenced in the meta-regression.

