











 text in
text in  English (pdf)
English (pdf)
 Article in xml format
Article in xml format Article references
Article references
 Send this article by e-mail
Send this article by e-mail Cited by SciELO
Cited by SciELO  Cited by Google
Cited by Google  Similars in
SciELO
Similars in
SciELO  Similars in Google
Similars in Google 
 Permalink
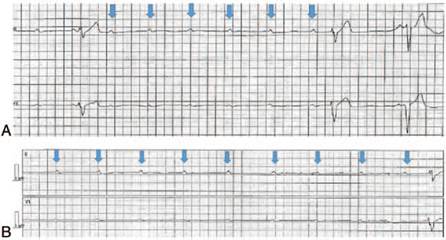
PermalinkClassic myotonic dystrophy is a multisystem disorder that results from RNA toxicity and is one of the commonest adult onset muscular dystrophies. Patients often present with muscle stiffness from myotonia and dysphagia or dysarthria from laryngopharyngoesophageal muscle weakness. Benign electrocardiogram changes such as first degree atrioventricular block are commonly present and rarely merit further work up. Occasionally, patients develop advanced conduction defects which can unexpectedly progress to complete heart block perioperatively.1 This circumstance is demonstrated by the accompanying images. The preprocedure 12 lead electrocardiogram exhibits a 2:1 atrioventricular block pattern (Fig. 1). The blue arrows in Lead II mark the position of P waves. For every 2 P waves, 1 narrow QRS complex is seen. During cystoscopy under general anesthesia, the rhythm suddenly deteriorates to complete heart block (Fig. 2A and B).
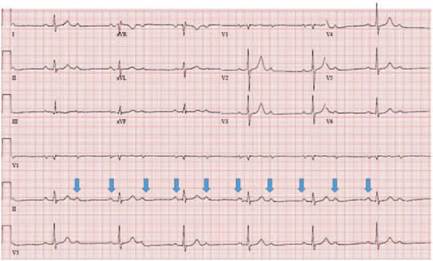
2:1 atrioventricular block is a distinct second-degree heart block that merits immediate consultation as even asymptomatic patients may need permanent pacemaker implantation before surgery. Presence of wide QRS complexes with this pattern suggests infra-atrioventricular nodal disease and a heightened risk of progression to complete heart block. Rarely, even narrow QRS complexes may represent infranodal disease, as in this instance. Unlike a resting electrocardiogram, a cardiac electrophysiological study reliably identifies infranodal disease.2
Hyperkalemia, hypothermia, and use of vagomimmetic medications like remifentanil or beta blockers can worsen atrioventricular conduction and precipitate complete heart block in these patients.3 Hemodynamically unstable complete heart block is characterized by non-conduction of atrial impulses to the ventricles, an unreliable slow ventricular escape rhythm, abrupt decrease in cardiac output, precipitous hypotension, and cardiovascular collapse. As complete heart block is often resistant to treatment with atropine or inotropes, transcutaneous pacing should be instituted early. Persistent complete heart block necessitates transvenous pacing. Intraoperatively, invasive arterial monitoring, plethysmography, and echocardiography help confirm successful mechani cal capture during pacing.2
Ethical responsibilities
Protection of people and animals: no experiments on people or animals were done.
Confidentiality of the data: all protocols at our institute were followed and patient or hospital identifiers have been removed from all images.
Right to privacy and informed consent: as patient and hospital identifiers have been removed, no informed consent was solicited for this production.

