











 text in
text in  English (pdf)
English (pdf)
 Article in xml format
Article in xml format Article references
Article references
 Send this article by e-mail
Send this article by e-mail Cited by SciELO
Cited by SciELO  Cited by Google
Cited by Google  Similars in
SciELO
Similars in
SciELO  Similars in Google
Similars in Google 
 Permalink
Permalink
Introduction
The need for palliative health care has been defined as "the population's ability to benefit from palliative care."1,2 This designation includes a professional perspective, which is useful when considering the need for palliative care at a national population level.3 In epidemiology, "need" refers to "specific indicators of disease which require intervention because the level is above that generally accepted within a particular society."4 Following this definition, "needs" must reflect value judgments on the ability to control the problem but also awareness about certain growing problems within societies.5
Demographic changes leading to aging of the population and the accompanying increase in long-term conditions and multimorbidity requiring advanced medical care have moved all health sectors to provide day-to-day care to patients with more advanced diseases and end-of-life. Many people, not only terminally ill patients, could benefit from palliative care which is mainly focused on quality of life and relief of symptoms.6,7
It is well known that worldwide, there is a big discrepancy in availability of palliative care services between countries, with most low-income and middle-income countries having clearly unmet needs. In this study, we set out to determine the needs of palliative care for cancer and non-cancer diseases in Colombia, which is considered an upper middle-income country by the World Bank but as well a country with many challenges in society and very large socioeconomic inequalities between and within regions of the country.8,9
The demographic composition of the Colombian population is changing rapidly, due to general demographic changes, combined with a large influx of refugees from Venezuela and the recent "peace" process, which has greatly diminished deaths due to violence. In general, the tendency is for the population ages 65+ to proportionally increase rapidly-which almost automatically implies strong increases in the prevalence of non-communicable diseases.10 This translates into an expected, but currently undocumented, increased need for palliative care. Understanding healthcare needs is essential to planning and expanding services, yet no national palliative care needs estimation has been carried out in Colombia nor, as far as we know, in South America.
Since 2014, the Colombian government has introduced regulation regarding health care of people with advanced, degenerative, terminal, and irreversible diseases.11 In addition, a guideline for the treatment of people in palliative care is available, as well as access to opioids for pain management.12,13
Patients with a large variety of conditions are in need of palliative care. A particular, and frequently studied group of diseases is cancer-which need many different types of palliative support, from nutrition to ventilation and from pain management to psychologic and spiritual counseling.14,16 However, many other diseases are also very important in the need for palliative care.17,18 Therefore, in this project we estimate the potential population in need of palliative care services in Colombia based on national mortality data-disaggregated by cancer and non-cancer deaths. Using the available data from the national palliative care observatory, we intend to compare the estimated needs with the current offer, to help decision makers in determining where the greatest needs are.
Provide an estimate of the need of palliative care services in Colombia and compare these needs with the current available offer.
Methods
We developed an observational cross-sectional death certificate-based study of individuals deceased above 18 years in Colombia between 2012 and 2016. The analyses are based on public and anonymized data from death certificates provided by National Administrative Department of Statistics of Colombia (DANE). Vital records are continuous statistics that collect information on births, fetal and non-fetal deaths, thus providing the information on changes in the levels and patterns of mortality and fertility. These information is publicly available through website of DANE (https://www.dane.gov.co). Chronic conditions for which palliative care is requires were identified from the main cause of death using ICD-10 codes.
Deaths requiring palliative care
A minimal estimate was calculated based on the number of deaths from specific conditions identified as having palliative care needs.3 Unfortunately, it was not possible to link with hospital records, limiting the possibility of more reined estimates. In line with the methods applied by Gomes et al,19 in their modification to a previous paper,3 we defined deaths requiring palliative care as those deaths with underlying cause of death coded as summarized in Table 1. These deaths-related codes have shown a requirement of palliative care ranging from 69% to 82%.3
Table 1 Description of Cause of Death and ICD-10 codes used to categorize deaths requiring palliative care.
| Underlying cause of death | ICD-10 codes |
|---|---|
| Malignant neoplasm | C00-C97 |
| Heart & cerebrovascular disease | I00-I52 (excluding I12 and I13.1), I60-I69 |
| Renal disease | N17, N18, N28, I12, I13.1 |
| Liver disease | K70-K77 |
| Respiratory disease | J06-J18, J20-J22, J40-J47, J96 |
| Neurodegenerative disease | G10, G20, G35, G122, G903, G231 |
| Alzheimer's, dementia and senility | F01, F03, G30, R54 |
| HIV/AIDS | B20-B24 |
Source: Authors.
Offer of palliative care services
Data to estimate the current offer of palliative care services was extracted from the Colombian Observatory of Palliative Care, which provides information about availability of palliative care services per 100,000 inhabitants on a departmental level. These estimates are based on current hospitality offer of services related to palliative care and registered as health providers including day care, ambulatory palliative medical consultations, short or long stay hospital-based palliative care, residential-based palliative care, and home-based palliative care.17
Analysis
We stratified the analyses for cancer and other conditions (as specified in Table 1), age groups and major cities. We considered as variables of interest the total population (and stratified by age) and the total (and per category) number of deaths. R software (version 3.5.0, R 3.5.0: R Core Team. R: A Language and Environment for Statistical Computing [Internet]. Vienna, Austria: R Foundation for Statistical Computing; 2019. Disponible en: https://www.R-project.org/) was used for data analysis and graphs.
Results
Between 2012 and 2016, the Colombian estimated population grew from 46,581,823 to 48,747,708 persons. In the same period, the proportion of the population aged 60 years and over increased from 10.3% to 11.4% of the total population.
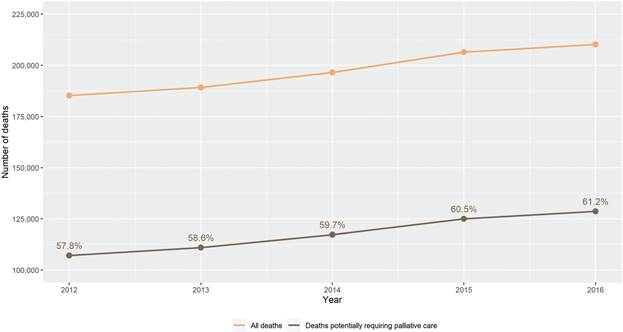
Figure 1 illustrates the increase in numbers of deaths due to any cause as well as those due to diseases which likely require palliative care: the absolute numbers of deaths increased from 185,248 in 2012 to 210,224 in 2016; the numbers of deaths requiring palliative care according to our definition increased from 107,065 in 2012 to 128,670 in 2016 (61.2%). About 1/3 of these cases were cancer-related (31.3% in 2016).
Source: Authors.
Figure 1 Absolute number of deaths due to any cause and proportion of deaths potentially requiring palliative care from 2012 to 2016 in Colombia.
The number of deaths likely to require palliative care increased with age, over the study period there were 7667 deaths requiring palliative care in the age group 18 to 44 years, increasing to 26,840 for ages 45 to 64, 42,288 for 65 to 79 and 48,203 for the 80+ population. Figure 2 shows how the causes of these deaths vary by age group, with a clearly more important proportion of heart and cerebrovascular diseases as well as dementia in advanced age-groups, and HIV/AIDS being much more important in the younger segments of the population. In all age groups, malignant neoplasms are an important part of the causes of deaths of those requiring palliative care.
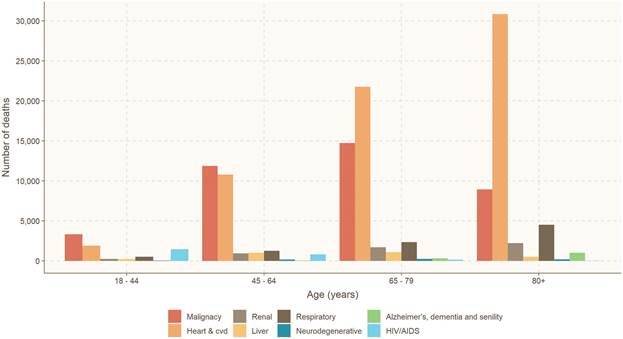
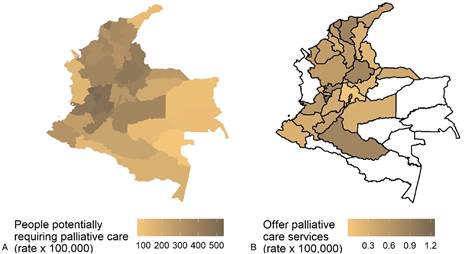
Figure 3A shows the people potentially requiring palliative care per 100,000 person-years-with concentrations in the more densely populated areas of the country. Contrasting this need of palliative care with the formal offer of palliative care services as reported by the national observatory of palliative care (Fig. 3B), it is clear that in some areas, there is no offer at all, in other areas with high need, the offer is limited, whereas in some areas with high demand the offer is below national average.
Discussion
Our results clearly show the high and growing need for palliative care services in the population, and also the deficiency of palliative care services on offer. Estimates from routine mortality data can give rough but reliable estimates of the population's need for palliative care.3,18,19 This information is essential to plan services. A real palliative care policy, not only on paper but implemented in reality, is necessary in Colombia to improve the palliative care service offer. Our findings clearly indicate a high potential need for palliative care in many areas of the country where this type of care is not currently widely offered.
More palliative care support is expected to be required for some illnesses and clinical syndromes, such as patients with multimorbidity, chronic progressive illnesses with long disease courses, diseases with complex symptoms and demographic changes. Our estimates show that the proportion of total deaths potentially requiring palliative care increases with time and they are in agreement with results from other middle-income and high-income countries.3,7,20 The proportion of individuals who died from diseases that indicate palliative care needs at the end of life ranged in the literature from 38% to 74% with an important cross-country variation.20-22 At population level, these estimations provide robust indications of the challenge countries are facing without major differences between high-income and middle-income countries.20 Our estimates of palliative care needs are probably quite similar to those of other Latin-American countries in transition, the palliative care offer depends heavily on the health systems in place in each country.
It is as yet very unclear how exactly health professionals and the entire Colombian health care system are to meet the increased population palliative care need. The current offer of palliative care is mainly due to services in third level of care (high complexity services) with 13 programs in the country, only 1 program at a second level hospital, 3 multi-level services and around 60 palliative home care services for the whole country (low-complexity services).23 Despite the strong increase between 2012 and 2016 in the offer of palliative care services (an increase of 500%), those services are located in urban big cities and departments (i.e., Bogotá D.C., Antioquia, Valle del Cauca, and Atlántico). Unfortunately, there were no data available regarding the capacity and scope of those providers at national level. Our data show that there are several areas with no offer at all in terms of palliative care.
There is a clear and urgent need for training in palliative care in medical faculties and adaptations from the side of the health system and health insurers to facilitate all kind of palliative care services. The current number of palliative care specialists is still very low and required early training is scarce. Research from low-income and middle-income countries highlights the need for education and training of staff and healthcare practitioners in palliative care and palliative care services.24 Besides training in palliative care skills at all levels, legal reforms will be necessary as the current legislation leaves little to no room for a wide range of health practitioners to be involved, to prescribe or apply, for example, morphine derivatives or nutritional interventions. In 2012, there were 57 medical faculties in Colombia and only 3 included palliative care training as an integral part of their health sciences curriculum.23 All these faculties and current palliative care services are located in urban big cities without major covering of middle cities or rural areas.
Limitations
Of course, a study based on death certificate information suffers from all factors that influence the quality of the death certification. Fortunately, in the studied period, a very large proportion of the deaths included in our analyses were certified by medical doctors, cause of death coding is always tricky.25 Some patients suffering from the diseases under study may have died of other diseases and not have been included. In some remote areas and particularly in isolated populations, such as some indigenous tribes, not all deaths may have been reported. However, we believe that by and large, our estimates reflect the need of palliative care-in all of its forms-in Colombia in recent years. Considering that not only fatally ill people need palliative care for optimum treatment, our estimates are likely a conservative estimate-the real need may be substantially higher. The contrast with the current official offer of palliative care is stark. Strong legislation regarding opioid availability is limiting availability of vital pain management medicines,26 and lack of knowledge and human resources for all aspects of palliative care is clearly lacking.
Conclusion
The current offer of palliative care services seriously lags behind the current demand. With very limited training facilities in the field of palliative care and a growing need because of the rapidly ageing populations, effective policy is urgently needed to improve the situation.
Ethical responsibilities
Design. Observational cross-sectional death-certificate based study of individuals deceased above 18 years in Colombia between 2012 and 2016.
Data sources. The analyses are based on public and anonymized data from death certificates provided by National Administrative Department of Statistics of Colombia (DANE). Chronic conditions for which palliative care is requires were identified from the main cause of death using ICD-10 codes.
Ethical approval. Since this study used routinely, anonymized, and publicly available data, no ethical approval was necessary for this study.

