











 text in
text in  English (pdf)
English (pdf)
 Article in xml format
Article in xml format Article references
Article references
 Send this article by e-mail
Send this article by e-mail Cited by SciELO
Cited by SciELO  Cited by Google
Cited by Google  Similars in
SciELO
Similars in
SciELO  Similars in Google
Similars in Google 
 Permalink
Permalink
What do we know about this topic?
We know that the effective dose ED-90 for intrathecal hydromorphone is 75 μg.
The limited literature available ascertains that the combination of bupivacaine, hydromorphone and fentanyl compared against bupivacaine, morphine and fentanyl shows no statistically significant differences with regards to the quality of the anesthesia, analgesia or adverse effects.
The morphine hydrochloride available in Colombia has no indication in the safety data sheet for intrathecal use, whilst hydromorphone does.
What are contributions of the study?
The mixture of hydromorphone and bupivacaine may be a valid option to replace the traditional mixture with bupivacaine, morphine and fentanyl, for subarachnoid anesthesia in cesarean section, with the added advantage of improved postoperative pain control over the first 12 hours.
INTRODUCTION
The Clinical practice guidelines for obstetric anesthesia of the American society of Anesthesiology and those of the American Society of Pain, recommend the routine use of neuraxial anesthesia for cesarean section 1, because it reduces the maternal risk, has improved fetal outcomes, and provides better postoperative analgesia. 2
The classical regimen for cesarean section is based on a combination of the local anesthetic (LA), one lipophilic opioid - for instance, fentanyl - and one long-acting hydrophilic opioid-for instance morphine -. 3
The erratic availability of morphine is a real challenge in Colombia and in other countries. 4,5 Reasons such as the lack of stimulus for the pharmaceutical companies to produce molecules with expired patents, and shifts in the demand for the product, may result in drug shortages. On the other hand, excipient-free morphine sulphate is the preparation endorsed for intrathecal use; however, it is not available in Colombia, so morphine hydrochloride has been used, although this preparation is not registered for this route of administration. Hydromorphone in contrast, does have a safety data sheet for spinal administration.
With regards to fentanyl, there are no studies available assessing the relevance of removing it from the preparations with hydromorphone for spinal injection. The academic discussion among anesthesiologists to remove fentanyl was based on two aspects: 1. The maximum effect of fentanyl is achieved after 10-20 m and that of hydromorphone is achieved after 20-30 m, which is not a clinically significant difference in the context of neuraxial anesthesia. 6-8. 2. The duration of the effect of fentanyl is 130 m, which is very similar to the local anesthetic (LA). 9
The results of this study are consistent with those claiming a lower pain score in anesthesia for cesarean section with hydromorphone, but disagree with the studies describing an equivalence to morphine. This may be due to variations in the doses studied 10, and suggest that the effective dose described in the literature may approach the cut-off point for such effect. 5
As a contingency mechanism in 2017, due to the shortage of morphine, the SES Hospital in Caldas, prepared bupivacaine, morphine and fentanyl (BMF) and bupivacaine, fentanyl and hydromorphone (BFH) prefilled syringes for subarachnoid anesthesia at its compounding central, based on the available publications 4,5, and one without fentanyl bupivacaine and hydromorphone (BH). The objective of this paper is to compare the clinical analgesic efficacy of these three anesthetic mixtures used in cesarean section, at the time of the incision and over the first 12 hours after surgery.
METHODS
Type of study: Observational, analytical.
Ethical approval: This study received the approval of the two committees: Ethics Committee of the Universidad de Caldas (Ethics Committee CBCS-032, May 7, 2018) and Ethics Committee of the SES Hospital of Caldas (Ethics Committee DC-048-18, May 7, 2018), both in Manizales, Colombia. Moreover, each patient surveyed completed their informed consent.
Setting: SES Hospital of Caldas is a third-level referral center for highly complex obstetric care in the Department of Caldas, located in Manizales city, Colombia.
Population: Full term pregnant women over 15 years old, with an indication for cesarean section and subarachnoid anesthesia, from June 2018 and May 2019. Patients with multiple pregnancies, chronic use of opioids, allergies to any of the drugs of the prefilled syringes, suspicion of maternal-fetal abnormalities, and patients who received any additional medication or a lower dose than the intrathecal premix, as prescribed by their treating physician, were all excluded.
Exposure: Subarachnoid anesthesia for cesarean section is a standard practice at the hospital. The preparations of the packaged prefilled syringes in the compounding central are:
Hyperbaric Bupivacaine 05 % 2 mL + morphine 100 μg and fentanyl 10 μg (2.3 mL) (BMF)
Hyperbaric Bupivacaine 0.5 % 2 mL + hydromorphone 80 μg and fentanyl 10 μg (2.4 mL) (BFH)
Hyperbaric Bupivacaine 0.5 % 2 mL + hydromorphone 80 μg (2.1 mL) (BH)
Data collection: All data were collected by the team of investigators. The instrument to measure postoperative pain at 3, 6 and 12 hours was standardized, the reviewers received a preliminary training to use of the SES Hospital of Caldas rule, which is based on the numerical visual analogue scale (VAS). The electronic medical records and the anesthesia records were reviewed to identify any missing data. Patients were followed for 24 hours in the hospital.
Biases: A convenience sampling was conducted between June 2018 and May 2019, regardless of the anesthesiologist in charge, or of the reason for choosing the premix, in order to control the selection bias. All paints remained hospitalized for at least 24 hours to control for the non-response bias. All outcome variables were objectively measured, and pain was directly scored by each patient. All of the patients receiving care accepted to participate in the study.
Statistical analysis: The information obtained was logged into a previously designed Excel database and was analyzed using the SPSS version 25 software. The results are shown on frequency distribution charts. The normal distribution continuous variables are summarized as averages and standard deviation. The continuous variables with non-normal distribution are summarized with median and interquartile range. The Kruskal-Wallis non-parametric test was used at all time points in which the VAS was analyzed. The variance analysis for repeated measurements was not used due to the small sample size. A bivariate analysis was conducted to identify the association between pain at the time of the cesarean section incision, adverse effects, and postoperative pain with the intrathecal mixture used. The categorical variables were compared using Chi square or the exact Fisher's test, as needed. A new stratified analysis was conducted to control for any confounding variables, such as having received prophylactic antiemetics during the trans-operative period, and adjuvant analgesia during the intra and post-operative periods.
RESULTS
71 patients were studied (figure 1), of which 40.9 % (n: 29) received the usual BMF combination; 22.5 % (n:16), BFH; and 36.6 % (n: 26), BH. No patients were lost to follow-up. The characteristics of the population are shown in Table 1. The reason for the anesthesiologist to prescribe one or other combination is described in Table 2.
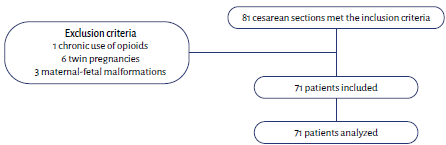
TABLE 1 Characteristics of the population.
| BMF (n: 29) | BFH (n: 16) | BH (n: 26) | p | |
|---|---|---|---|---|
| Age in years (SD) | 28.6 (6) | 30.6 (7.4) | 27.5 (6.4) | |
| Gestational age, weeks (IR) | 39 (38-39) | 39 (38-40) | 39 (38-39) | |
| ASA Classification | ||||
| ASA 2 | 96.5 % | 93.8 % | 92.3 % | 0.82 |
| ASA 3 | 3.5 % | 6.2 % | 7.7 % | |
| Pregnancy | ||||
| Pregnancy | 34.5 % | 37.5 % | 45.8 % | 0.74 |
| Pregnancy 2 | 37.9 % | 43.8 % | 25 % | |
| Pregnancy ≥ 3 | 27.6 % | 18.7 % | 29.2 % | |
| Previous cesarean sections | ||||
| Cesarean sections 0 | 48.3 % | 62.5 % | 50 % | 0.51 |
| Cesarean sections 1 | 34.5 % | 37.5 % | 41.7 % | |
| Cesarean sections 2 | 17.2 % | 0 % | 8.3 % | |
| Indication | ||||
| Previous cesarean section | 27.6 % | 25 % | 16.7 % | 0.82 |
| Failed induction | 10.3 % | 6.2 % | 16.7 % | |
| Dysfunctional labor | 6.9 % | 6.2 % | 8.3 % | |
| Unsatisfactory fetal status | 6.9 % | 6.2 % | 0 % | |
| Fetopelvic disproportion | 13.8 % | 0 % | 4.2 % | |
| Abnormal presentation | 20.7 % | 31.3 % | 25.0 % | |
| Maternal pathology | 10.3 % | 25.0 % | 20.8 % | |
| Maternal wish | 3.5 % | 0 % | 8.3 % | |
ASA: American Society of Anesthesiologist, BFH: bupivacaine, fentanyl and hydromorphone, BH: bupivacaine and hydromorphone, BMF: bupivacaine, morphine and fentanyl, IR: interquartile rank SD: standard deviation. SOURCE. Authors.
TABLE 2 Reason for selecting the anesthetic mixture.
| Preference | BMF | BFH | BH | |||
|---|---|---|---|---|---|---|
| n | % | n | % | n | % | |
| Is the one I have always used | 21 | 72.4 | 0 | 9 | 0 | 0 |
| I think a new option is interesting | 2 | 6.9 | 16 | 100 | 24 | 92.4 |
| I believe there is less vomiting | 0 | 0 | 0 | 0 | 1 | 3.8 |
| Only option available | 1 | 3.5 | 0 | 0 | 1 | 3.8 |
| By chance | 4 | 13.7 | 0 | 0 | 0 | 0 |
| Syringe allocated by nurse | 1 | 3.5 | 0 | 0 | 0 | 0 |
| Total | 29 | 100 | 16 | 100 | 26 | 100 |
BFH: bupivacaine, fentanyl and hydromorphone, BH: bupivacaine and hydromorphone, BMF: bupivacaine, morphine and fentanyl. SOURCE. Authors.
Regardless of the mixture used, none of the patients experienced pain during the incision, or required changing the anesthetic technique. There were no statistically significant differences in terms of the incidence of pruritus (p 0.64) and hypotension (p 0.10), none of the patients experienced respiratory distress and there was no difference in the duration of the motor block (table 3).
TABLE 3 Recovery of motor block.
| BMF (n: 29) | BFH (n: 16) | BH (n: 26) | |
|---|---|---|---|
| Time in minutes (SD) | 155 (8.35) | 153.6 (7.12) | 152.5 (8.12) |
| 95 % CI | 137.8-172.1 | 138.3-168.9 | 135.8-169.2 |
BFH: bupivacaine, fentanyl and hydromorphone, BH: bupivacaine and hydromorphone, BMF: bupivacaine, morphine and fentanyl, CI: Confidence interval, SD: standard deviation. SOURCE. Authors
Forty two patients received a prophylactic antiemetic (16 BMF, 11 BFH y 15 BH), 16 patients received two prophylactic antiemetics (7 BMF, 4 BFH and 5 BH) and 12 patients did not receive any of those drugs. There were no statistically significant differences among the groups in terms of nausea or vomiting (table 4).
TABLE 4 Stratified analysis of nausea and vomiting.
| Prophylactic antiemetics | BMF | BFH | BH | p* | ||||
|---|---|---|---|---|---|---|---|---|
| n | % | n | % | n | % | |||
| 1 antiemetic | Nausea | |||||||
| Yes | 11 | 68.7 | 4 | 36.3 | 5 | 33.3 | 0.10 | |
| No | 5 | 36.3 | 7 | 63.7 | 10 | 66.7 | ||
| Total | 16 | 100 | 11 | 100 | 15 | 100 | ||
| Vomiting | ||||||||
| Yes | 4 | 25.0 | 5 | 45.5 | 1 | 6.7 | 0.07 | |
| No | 12 | 75.0 | 6 | 54.5 | 14 | 93.3 | ||
| Total | 16 | 100 | 11 | 100 | 6 | 100 | ||
| 2 antiemetics | Nausea | |||||||
| Yes | 5 | 71.4 | 2 | 50.0 | 2 | 40.0 | 0.55 | |
| No | 2 | 28.6 | 2 | 50.0 | 3 | 60.0 | ||
| Total | 7 | 100 | 4 | 100 | 5 | 100 | ||
| Vomiting | ||||||||
| Yes | 1 | 14.3 | 1 | 25.0 | 2 | 40.0 | 0.61 | |
| No | 6 | 85.7 | 3 | 75.0 | 3 | 60.0 | ||
| Total | 7 | 11.1 | 4 | 0 | 5 | 0 | ||
* Kruskal-WallisTest. BFH: bupivacaine, fentanyl and hydromorphone, BH: bupivacaine and hydromorphone, BMF: bupivacaine, morphine and fentanyl. SOURCE. Authors.
All patients that received BMF and experienced hypotension (n: 16), had nausea; on the contrary, among those receiving BFH or BH, only 50 % of those that experienced hypotension, presented nausea during the trans-operative period.
There were group differences in the pain record at 3 and 6 hours. As seen in Figure 2, the mean difference was smaller among patients who received the BFH and BH mixtures, as compared to those receiving the BMF combination; according to the clinical manifestation, this suggests less postoperative pain in the groups of patients receiving hydromorphone.
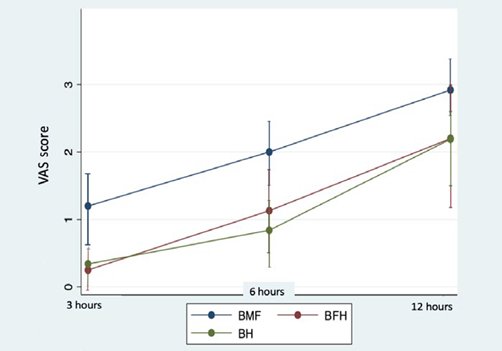
BFH: bupivacaine, fentanyl and hydromorphone, BH: bupivacaine and hydromorphone, BMF: bupivacaine, morphine and fentanyl, VAS: visual analogue scale. source. Authors.
FIGURE 2 Postoperative pain
Adjuvant analgesia during the trans-operative period included sodium dipyrone, 2 g IV; diclofenac, 75 mg IV; or both, upon removing the fetus. During the postoperative period, patients received - as instructed by the ObGy service - sodium dipyrone, 2 g IV every 8 hours; diclofenac, 75 mg IV every 12 hours; and oral acetaminophen, 1 g every 8 hours; the use of diclofenac was only avoided in patients with any presentation of renal impairment (n: 13).
DISCUSSION
The usual institutional mix is prepared with 10 mg of hyperbaric bupivacaine, in accordance with a meta-analysis conducted in 2011 by Arzola and Wieczorek 4, showing that although the low doses of bupivacaine (< 8 mg) are associated with a lower risk of hypotension, nausea, and vomiting, they compromise the effectiveness of the anesthetic block, which is evidenced by the increased need of additional analgesia during surgery and higher conversion rates to general anesthesia, as compared to the conventional doses (> 8 mg).
The liposolubility of the opioid is inversely proportional to the time or residence and diffusion into the cerebrospinal fluid (CSF). 7 With regards to the intrathecal puncture site, the rostral spread of the drug, and the analgesic effect of fentanyl - with an octanol:buffer (O:B) partition coefficient of 955 in contrast to morphine 7,11 - which has a barely metameric and short-lived spread; morphine O:B of 1 11,12 has a high and late spread, which accounts for the risk of respiratory depression up to 24 hours after its injection. Hydromorphone, with a comparative O:B of 525 11,12, has a long-acting effect as do all hydrophilic opioids, but an intermediate diffusion over time, and a higher dermatomeric extension than fentanyl, but lower than morphine 7(Figure 3).
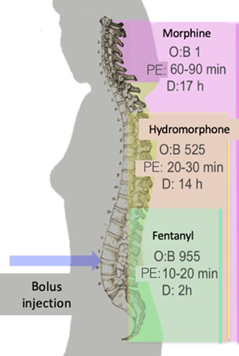
D= Duration, O:B= octanol:buffer, PE= peak effect . FUENTE. Modified by the authors, based on Mugabure, et all 7,8.
FIGURE 3 Spread of opioid analgesia following spinal administration.
Morphine has a pKa of 8.21 13,14 and a pH of 7.32, corresponding to the CSF; it has an 11.4 % of non-ionized fraction (Non-ionized fraction = 10(pH-pKa) ÷ 1-10(pH-pKa)). Morphine in the neuraxial scale has an onset of action of 15-30 minutes, a peak effect at 60-90 minutes 8 and an average duration of 17 hours without the need to administer any rescue opioids, at doses of 200 μg 4. Hydromorphone also has a pKa of 8.2 13,14, but due of its additional pharmacokinetic characteristics has an onset of action at 10-15 m, a peak effect at 20-30 m 8 and a mean duration of 14.6 hours with no need to administer any rescue opioids, at an intrathecal dose of 60 μg 4
Johansen et al., discovered that intrathecal hydromorphone is faster in accessing the dorsal horn neurons and a faster onset of analgesia. 15 Moreover, due to its intermediate liposolubility, hydromorphone has a lower rate of adverse effects with an epidural administration. 16,17. The current reference ED 90 is 75 μg for hydromorphone and 150 μg for morphine. 5. The decision to do the hydromorphone preparations with 80 μg was a joint decision adopted by the team of anesthesiologists of the SES Hospital of Caldas and the compounding central, in order to avoid mistakes during preparation.
In our study, there was improved pain control over the first 12 postoperative hours in the BFH and BH groups. Beatty et all., compared 38 pregnant women in labor that received 0.04 mg of spinal hydromorphone and 76 who received 0.1 mg of spinal morphine, and found no differences in terms of analgesia or incidence of side effects. 18 The disparity with our study, in terms of analgesia, may be due to the higher dose of hydromorphone. 5 Rauch et all., found that the patients receiving hydromorphone experienced significantly lower pain levels after 4, 12 and 24 hours, as compared to other combinations (LA and LA plus). The conclusion was that intrathecal hydromorphone seems to be more effective in providing analgesia during the intra and post-operative period in cesarean section than other opioids, including morphine. 11 There is however one yet unanswered question regarding the physical and affinity characteristics for the dorsal horn receptors.
Regarding the recovery time of the anesthetic block, it has been widely known that thinner nerves are more sensitive to the effects of LA agents, due to the high relationship between the surface area of the membrane and the unit volume of the axon. 19. This may lead us to believe that the LA may result in a visceral analgesic effect (non-myelinated C 0,3-1 μm fibers) long after the motor recovery (myelinated Α-δ, 1-4 μm fibers), in average 153 minutes in our study, giving hydromorphone enough time to start acting.
One of the arguments to use fentanyl in the subarachnoid mix is that phenylpiperidine-derived opiates exhibit close structural similarities of the LA agents, and this may result in a synergistic effect of its action on the C sensory fibers and the possibility to lower the LA dose 20, in order to reduce hypotension, nausea and vomiting in the transoperative period. 15,16 However, no studies have yet been conducted to forcefully proof this fact. 16 Moreover, the anatomic variations in pregnant patients must be taken into consideration, i.e.: reduced CSF volume as a result of the distention of the epidural veins, cephalic movement of hyperbaric anesthetics in supine position, and the huge sensitivity of the nerve fibers that result in lower intrathecal anesthetic requirements versus the non-pregnant population. 21 Furthermore, the duration of analgesia with intrathecal fentanyl is approximately 130 minutes 8,9,22, very similar to the duration of LA agents, which further questions the actual benefit of such drug. 9
The effects of fentanyl and morphine, alone and in combination, as adjuvants for spinal anesthesia in elective cesarean section, were examined in a clinical trial. The conclusion of the trial was that the opioid combination adds no further advantages versus the mix with morphine only. 23 Specifically, the trial failed to show a difference in the incidence of adverse effects between the groups. It may be reasonable to believe that by reducing the burden of opioids, their side effects will be less. Maybe larger studies could specifically show the clinical benefit of removing fentanyl from the hydromorphone mix.
With regards to hypotension, it is clear that its incidence in this group of patients is multifactorial in origin, and increases when raising the dose of operative bupivacaine, while decreases only when doses of < 6 mg are used. 21 However, the deleteriouseffect of using such low doses is well known. The anesthesia guidelines for cesarean section recommend the simultaneous loading with crystalloids, the prophylactic use of a vasopressor (ephedrine, phenylephrine, norepinephrine) and the lateralization of the uterus, to prevent this frequent outcome of neuraxial anesthesia. 21,24. In our hospital in particular, phenylephrine as a vasopressor is not available, and instead, norepinephrine is used in boluses of 8 μg or etilefrine 1 to 2 mg, in accordance with the preference of the anesthesiologist; this is a limitation in this study. Along these lines, the presence or absence of hypotension may be more related to the sympathetic block caused by the LA agent, rather than by the combination of opiates.
According to the literature, the incidence of respiratory depression is of 0.03-7 %. 6 Lipophilic intrathecal opiates may cause early respiratory depression (0-1 hour), whilst the more hydrophilic opiates may result in either early or late respiratory depression (up to 24 hours). Specifically morphine may induce respiratory depression between 3.5 and 12 hours after the injection, with a peak at 6 hours. 6 It should be mentioned that the clinical monitoring of the hospitalized patients was performed for a minimum of 24 hours, and no incidents of this nature were experienced.
The presence of pruritus in this study is consistent with the current literature. It is known to be more frequent in pregnant women, probably due to disruptions in gestational hormones in the opioid receptors. Its incidence according to previous reviews ranges from 0 and 100 %, and predominantly affects the face, the neck, and the upper chest. 6
These results should be carefully interpreted, since this is an observational analytical study, with some limitations such as convenience sampling, imbalanced groups, and no sample size calculation which probably resulted in indication and selection biases, since the intervention was not randomized. No minors were exposed to any risks on behalf of the investigators, since the allocation of the premix is part of the autonomous and usual clinical practice of each treating anesthesiologist.
The external validity of this study is limited to high complexity obstetric centers that have available a compounding central pharmacy for preparing medications. This study may be the basis for designing future randomized, controlled clinical trials with a more rigorous methodological approach and adequate sample sizes, able to contest or reaffirm the results, and generate significant impact on clinical practice.
CONCLUSION
Mixtures with hydromorphone may be a valid option to replace the usual mixtures with bupivacaine, morphine and fentanyl, in subarachnoid anesthesia for cesarean section. Hydromorphone has the advantage of having a safety data sheet that authorizes its intrathecal use, and apparently results in improved postoperative pain control after 3, 6 and 12 hours.
ETHICAL RESPONSIBILITIES
Protection of humans and animals
The authors declare that no experiments were conducted in human beings or in animals for this research project.
Confidentiality of the information
The authors declare that all of the institutional protocols regarding the publication of patient data were followed.
Right to privacy and informed consent
The authors have obtained the informed consents of all patients and/or subjects mentioned in this article. The corresponding author is the custodian of these documents.
Ethical approval
This study received the approval of the two committees: Ethics Committee of the Universidad de Caldas (Ethics Committee CBCS-032, May 7, 2018) and Ethics Committee of the SES Hospital of Caldas (Ethics Committee DC-048-18, May 7, 2018), both in Manizales, Colombia. Moreover, each patient surveyed completed their informed consent.
ACKNOWLEDGEMENTS
Contributions by authors
CIOG and GAOG: Original project design, planning of the study, data collection, interpretation of the results, and initial and final approval of the manuscript.
JFVR: Planning of the study, data collection, interpretation of the results and final approval of the manuscript.
FAG: Planning of the study, analysis and interpretation of the results and approval of the final manuscript.

