











 text in
text in  English (pdf)
English (pdf)
 Article in xml format
Article in xml format Article references
Article references
 Send this article by e-mail
Send this article by e-mail Cited by SciELO
Cited by SciELO  Cited by Google
Cited by Google  Similars in
SciELO
Similars in
SciELO  Similars in Google
Similars in Google 
 Permalink
Permalink
The accompanying images exhibit a large tumor arising from the right hepatic lobe (Image A) that subsequently spontaneously ruptures leading to hemoperitoneum (Image B).
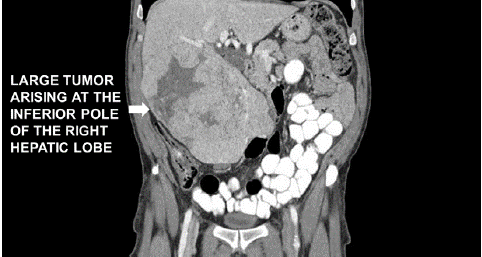
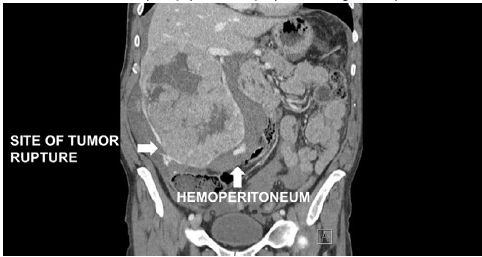
Hepatocellular carcinoma often occurs in the context of chronic liver disease. Spontaneous tumor rupture is an uncommon but life threatening event and may result from rapid tumor growth and necrosis. As tumor blood supply is from the hepatic artery, hemorrhagic shock can rapidly ensue. In addition to sudden onset severe abdominal pain and distension, patients present with features of acute bleeding including tachycardia, tachypnea, hypotension and concurrent decrease in serum hemoglobin levels.1
Emergent hepatectomy is often required when hepatic artery embolization is contraindicated, unavailable or fails to control bleeding. In addition to establishing invasive arterial monitoring and large bore intravenous access, early activation of massive blood transfusion protocol is prudent. Prior to induction, the surgical team should prepare and drape the patient in readiness to make incision. Anesthetic goals include maintaining a normal pH, core temperature >35 degree centigrade, ionized calcium levels of 1.1-1.35 mmol/L, hemoglobin of 7-9 g/ dl and lactate < 4 mmol/L. Large volume resuscitation with 0.9% normal saline and starch based colloids is discouraged as the former leads to dilutional coagulopathy with hyperchloremic acidosis and the latter precipitates an acquired von Willebrand syndrome by interfering with factor VIII function. Vasopressors are often required to maintain adequate systemic perfusion. Thromboelastography helps guide platelet, fibrinogen and plasma replacement. In conjunction with clinical assessment, frequent blood gas analysis helps determine need for blood transfusion. Although hyperventilation to compensate for metabolic acidosis seems intuitive, it may compromise cerebral perfusion and impede right ventricular filling by increasing intrathoracic pressure. 2 Optimization of oxygen delivery, restoration of tissue perfusion and use of buffers such as sodium bicarbonate or tris-(hydroxymethyl)-aminomethane (THAM) when the pH is < 7.1-7.2 helps ameliorate metabolic acidosis 3.

