











 text in
text in  English (pdf)
English (pdf)
 Article in xml format
Article in xml format Article references
Article references
 Send this article by e-mail
Send this article by e-mail Cited by SciELO
Cited by SciELO  Cited by Google
Cited by Google  Similars in
SciELO
Similars in
SciELO  Similars in Google
Similars in Google 
 Permalink
Permalink
What do we know about this topic?
The assessment of surgical and anesthesia care capacities has never been previously conducted in the Piura region.
What is the new contribution of this study?
It discusses the measurements of surgical and trauma capacities in a distant region from the capital and assesses the infrastructural gaps in public hospitals.
INTRODUCTION
Perú is a South American country, classified by the World Bank as a high-middle income country. It had an estimated per capita Gross National Income (GNI, previously called GDP) of US$ 6,740 in 2019 1. The economically active population totaled 17,830,481 inhabitants in 2019, with a life expectancy of 76.5 years from 2015-2020. 1,2
Surgical and anesthesia care is a critical component of a functional healthcare system and a requirement for universal health coverage. 3 The estimated world population with poor access to this type of care was 2 trillion in 2010. 4 It is precisely the middle-and-low-income countries (LMIC) that endure most of the challenges for access and delivery of surgical care. 3 Consequently, there is a need to improve the conditions of healthcare facilities where surgical care is provided in order to identify weaknesses and design adequate interventions. 5 Furthermore, the Peruvian surgical volume exhibited a growing trend, and in 2019 there were 2,631 surgeries per 100,000 inhabitants (854,795 surgeries in 32,495,510 inhabitants) 6,7 in contrast to 1,969 surgeries per 100,000 in 2015. 8
More than 5 million people die as a result of injuries around the world, representing 9%of the total number of deaths. Approximately one fourth of this number are the result of homicides and suicides, and another fourth are due to traffic accidents (TA). Similarly, in many LMIC deaths from injuries have increased over the last few years. 9 It has been estimated that in these countries, almost 2 million lives could be spared if the fatality rates of these cases were similar to those of high-income countries and that 52 million years of life adjusted for disability could be avoided if basic surgical care were to be expanded. 9,10 However, many survivors of these injuries experience temporary or permanent disabilities. 9
In Perú, the number of TA experienced a growing trend between 2002 and 2016 (accounting for 74,221 and 116,659 TA, respectively) £n], with a decline in 2018 (87,480 TA). (12I However, the number of fatalities resulting from TA showed a decreasing trend between 2012 and 2017 (with 4,037 and 2,826 deaths, respectively), with a rise in 2018 (3,244 deaths). 12
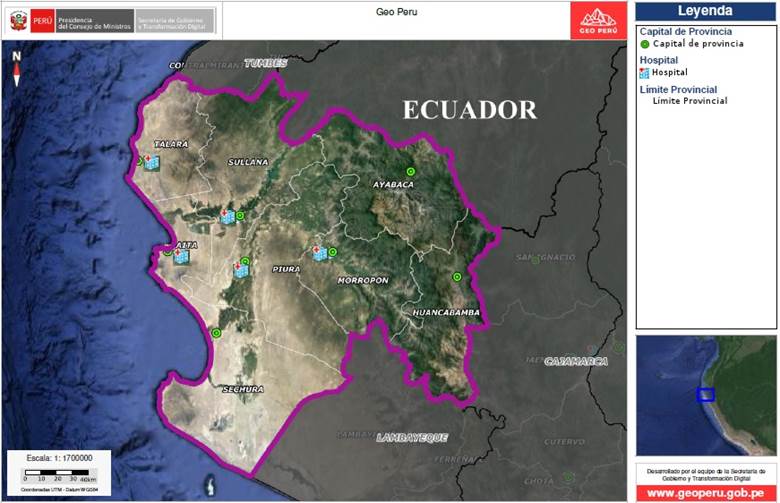
The Piura region is in the northern part of Perú, bordering Ecuador. It comprises eight provinces (Ayabaca, Huancabamba, Morropón, Paita, Piura, Sechura, Sullana and Talara), and has different natural zones according to the altitude (Coast or Chala up to 500 m above sea level; maritime Yunga from 500-2,300 m above sea level, Quechua from 2,300-3,500 m above sea level, and Suni from 3,500-4,000 m above sea level) (Figure 1). The population is 1,856,809 inhabitants according to the 2017 census, being the second largest after Lima; out of this total, the urban population is 1,471,833 and the rural is 384,976 inhabitants. 13 The primary objective of this study is to estimate the surgical and trauma care capacity of public hospitals throughout the provinces in the region, through the administration of international surveys. One additional objective was to estimate any inequalities in these capacities between the public hospitals in the capital province (Piura province) and the hospitals in the peripheral provinces of the region (located outside the Piura province) and among the various levels of complexity. The information about these capacities may offer a comprehensive description of surgical and trauma care delivered in the region, in order to identify any shortfalls and to implement improvement plans.
METHODS
Design of the study: A survey was administered which combined Spanish versions of the PIPES survey (Capacity survey based on personnel, infrastructure, procedures, equipment and supplies) 5 and the INTACT survey (International Assessment of Capacity for Trauma) 14. Likewise, some items not included in the previous surveys were assessed qualitatively, with regards to surgical equipment and essential surgical care supplies, and emergency care from the WHO "Tool for Situational Analysis to Assess Emergency and Essential Surgical Care". 15 The survey was administered both in hard copy and electronically.
The survey was conducted in seven public hospitals that offer surgery in the Piura region: three in the Piura province (a level hospital, a level II-2, and one level one level II-2 in the Sullana province, one level in the Talara province, one level in the Morropón province and one level II-1 in the Paita province. Their current classifications are consistent with Ministerial Resolution 546-2011/MINSA, of the Ministry of Health of Perú, and were registered under the National Health Superintendency of Perú (SUSALUD). 16 The classification of the Peruvian health organizations is based on the availability of certain minimal healthcare units and delivery of health and support services. The first level of care (level I) comprises the primary care facilities for the first four levels of complexity (categories I-2, I-3, I-4). The second level comprises the organizations classified as with the following service units as a minimum: Outpatient Clinic, Emergency Department, Hospitalization, Obstetrics Center, Surgical Center, Rehabilitation Medicine, Diagnostic Imaging, Clinical Pathology Pharmacy, Hemotherapy and Blood Bank, Nutrition and Dietetics, and Central Sterile. Level II-2 organizations shall have available Intensive Care Unit and Pathological Anatomy, in addition to all the Level II-1 services. Level Three institutions (type III-1) include Hemodialysis Units, in addition to all the services required for Level II-2. Hence, all institutions from level two onwards have a Surgical Unit. 16
Participants: Surgical staff members of the public hospitals in the region were interviewed to complete one single survey for each institution.
Quantitative Variables: The PIPES survey comprises 4 personnel criteria (from the surgical area), 14 infrastructure criteria, 40 surgical procedures criteria, 22 equipment criteria and finally 25 criteria regarding supplies available to the hospital or health institution. The personnel category accounted for the number of surgical specialists and anesthesia nurses. In terms of the infrastructure (for instance power availability) and equipment categories (for instance availability of pulse oximeter), one point was given if the criterion or item was always available, and 0 if it wasn't. With regards to the procedures category, one point was assigned if a particular type of surgery (for instance appendectomy) was conducted in the hospital. Finally, in the supplies category (for instance nasogastric tube) one point was given if the item was available or if there were sufficient stocks in the institution.
The INTACT survey has 7 infrastructure criteria (for instance, having a blood bank), 5 supplies criteria (for instance having urinary catheter), 16 procedures criteria (i.e., performing laparotomy), 10 equipment criteria (i.e., having an anesthesia machine available) and 2 personnel criteria (availability of anesthesiologists and surgical specialists). One point was assigned per item available in the institution or hospital. Hence, the maximum scores for infrastructure, supplies, procedures, equipment and personnel were 7, 5, 16, 10 and 2 respectively. The total scores per category and the total scores for each survey were estimated.
Qualitative Variables: 11 equipment criteria and 3 supplies criteria were assessed (detailed under the results paragraph) which were absent in the PIPES and INTACT surveys, and obtained from the WHO "Tool for Situational Analysis to Assess Emergency and Essential Surgical Care". Additionally, further inquiries were made about the most frequent type of surgery in hospitals, the need for surgical training, availability of trained trauma care personnel, distance to the nearest referral hospital and the reasons why these surveys could be helpful for surgical care in each hospital.
Data sources and measurements: With regards to the PIPES survey, the personnel category score - since it depends on the number of surgical specialists and anesthesia nurses - did not have a maximum score. The infrastructure category had a maximum number of 13 (if all of the points were reached for each item required) plus the number of functional Operating Rooms. The procedures category had a maximum of 40 (if the hospital conducted all the 40 different types of surgeries). The equipment category had a maximum score of 22 (if the hospital had all the items required). The supplies category had a maximum of 25 (if the institution had the 25 types of supplies available). The estimate of the PIPES score (total score) was done adding the scores for personnel, infrastructure, procedures, equipment and supplies. Then, the result was divided into 105 (total number of criteria) and then multiplied by 10. The highest PIPES scores correspond to the highest total surgical capacity.
To estimate the INTACT score, one point was assigned per each criterion or item met. Then, that score was divided into the total number of criteria (40) and multiplied by 10. The maximum INTACT score (total score) was 10 points. The highest INTACT scores correspond to the highest surgical capacity specifically for managing trauma.
Potential biases: To measure a similar time period in every hospital, the first two weeks in March 2020 were selected to collect the information. This choice was based on the national emergency resulting from the SARS-CoV-2 pandemic. Except for one province, the authors visited all public hospitals of the peripheral provinces to confirm the information collected with the reality of the facilities.
Sample size: The study was conducted in all general and public hospitals of the Piura region with a Surgical service unit. 16 One institution that only performed specialized ophthalmological surgery was excluded.
Statistical methods: The scores of both surveys were combined based on the localization of each hospital (within the capital province or in the peripheral provinces) and their level of complexity (level II-1 vs. level II-2), using medians as a central trend measurement and interquartile ranges as a measure of dispersion. Then, Mann-Whitney bilateral tests were conducted to assess the differences in the average hospital scores, according to localization and complexity. A p value < 0.05 was used. All the statistical procedures were conducted using the StatCrunch software (Pearson Education Inc).
The research protocol for this study was approved by the Ethics in Research Committee of the School of Health Sciences of the Universidad Nacional de Piura, under Minutes 26 of March, 2021 and submitted to the Education and Research Support Offices of the various participating hospitals.
RESULTS
Seven public hospitals of the Ministry of Health (MINSA) and Social Security of Perú (EsSALUD) which practiced surgery in five of the eight provinces of Piura were assessed. Four level II-1, two level II-2 and one level hospitals were included. The total number of hospital beds available were 838 (199 were third level and 639 were second level of care). Likewise, 479 beds were located in the Piura province and 359 in the peripheral provinces of the region.
The Piura province (capital province) which is the most densely populated and includes the capital city of the region, had three public hospitals. There was a difference in accordance with the geographical location in the INTACT survey, because the medians of the scores in the hospitals of this province tended to be higher than the medians of the hospitals in the peripheral provinces (9.5 vs. 8.25, p = 0.04). The difference was still present in the PIPES survey (16.38 vs. 10.91, p = 0.06).
In terms of the level of complexity, there was a trend for average scores of level II-2 hospitals to be higher than the level II-2 hospitals in the PIPES survey (14.38 vs. 10.91) and INTACT (8.38 vs. 8.25). Similarly, the averages of the PIPES and INTACT scores increased as hospitals grew in complexity. Hence, for level II-1 the scores were 10.91 and 8.25; for level II-2 the scores were 14.38 and 8.38; and for the level hospital, were 16.48 and 9.5 (PIPES and INTACT scores respectively). The summary of the scores for each criterion of the PIPES and INTACT tools of the public hospitals are illustrated in Supplementary content 1 and 2, respectively. Table 1 shows the scores for each category, the location in each province and the level of complexity.
Table 1 Answers to short questions of the survey in public hospitals in the Piura region.
| Survey | Province | Talara | Morropón | Sullana | Paita | Piura | Location | Level of complexity # | ||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Category* | Hospital | Hospital | Hospital II-2 | Hospital | Hospital II-2 | Hospital | Hospital | Within the Piura Province (n = 3)* | Outside the Piura Province (n = 4)* | P& | Level (n = 4)* | Level II-2 (n =2)* | P& | |
| P | Personnel | 22 | 31 | 55 | 30 | 73 | 44 | 77 | 73 (33) | 30.5 (17) | 0.11 | 30.5 (11.5) | 64 (18) | 0.13 |
| I | Infrastructure | 13 | 11 | 13 | 12 | 16 | 13 | 18 | 16 (5) | 12.5 (1.5) | 0.1 | 12.5 (1.5) | 14.5 (3) | 0.22 |
| P | Procedures | 30 | 32 | 35 | 24 | 38 | 32 | 35 | 35 (6) | 31 (6.5) | 0.21 | 31 (5) | 36.5 (3) | 0.1 |
| E | Equipment | 20 | 20 | 11 | 22 | 21 | 21 | 21 | 21 (0) | 20 (5.5) | 0.35 | 20.5 (1.5) | 16 (10) | 0.63 |
| S | Supplies | 24 | 23 | 16 | 24 | 24 | 23 | 22 | 23 (2) | 23.5 (4.5) | 1 | 23.5 (1) | 20 (8) | 0.8 |
| PIPES Score | 10.38 | 11.14 | 12.38 | 10.67 | 16.38 | 12.67 | 16.48 | 16.38 (3.81) | 10.91 (1.24) | 0.06 | 10.91 (1.38) | 14.38 (4) | 0.27 | |
| I | Infrastructure | 5 | 5 | 5 | 6 | 7 | 5 | 7 | 7 (2) | 5 (0.5) | 0.24 | 5 (0.5) | 6 (2) | 0.58 |
| N | Supplies | 5 | 5 | 2 | 3 | 5 | 4 | 5 | 5 (1) | 4 (2.5) | 0.56 | 4.5 (1.5) | 3.5 (3) | 0.81 |
| T | Procedures | 12 | 13 | 14 | 12 | 16 | 13 | 15 | 15 (3) | 12.5 (1.5) | 0.15 | 12.5 (1) | 15 (2) | 0.1 |
| A | Equipment | 9 | 8 | 4 | 10 | 10 | 10 | 9 | 10 (1) | 8.5 (3.5) | 0.27 | 9 (2) | 7 (6) | 1 |
| C | Personnel | 2 | 2 | 2 | 2 | 2 | 2 | 2 | 2 (0) | 2 (0) | 1 | 2 (0) | 2 (0) | 1 |
| T | INTACT Score | 8.25 | 8.25 | 6.75 | 8.25 | 10 | 8.5 | 9.5 | 9.5 (1.5) | 8.25 (0.75) | 0.04 | 8.25 (0.13) | 8.38 (3.25) | 1 |
Notes *: The scores are expressed as medians and interquartile range. & p values obtained using the bilateral Mann-Whitney test. PIPES: Capacity survey based on personnel, infrastructure, procedures, equipment, and supplies. INTACT: International Assessment of Capacity for Trauma.
Source: Authors.
Personnel: The public hospitals in the region reported 119 general surgeons, 62 anesthesiologists, and 151 specialists in other surgical areas. None of the hospitals reported anesthesiology nurses. A difference was identified according to the location (73 in the Piura province vs. 30.5 in the peripheral provinces, p = 0.11). Based on complexity, there was a difference in the PIPES score (64 in level II-2 vs. 30.5 in level II-1, p = 0.13). There was no difference in the INTACT survey with regards to location or level of complexity.
Infrastructure: Two hospitals in the region reported issues with continuous water supply (2/7 hospitals). Every hospital had an emergency power generator. Moreover, only four hospitals (4/7) had an incinerator and two had a functional around the clock CT-Scanner (2/7). Two did not have around-the-clock blood bank service (2/7). The total number of functional operating rooms was 25 in the public hospitals and only one hospital reported an operating room out of order.
Procedures: Higher medians were found in the PIPES survey (35 vs. 31, p = 0.21) and INTACT (15 vs. 12.5, p = 0.15) in the hospitals in the Piura province as compared to the peripheral provinces. The median in the level II-2 hospitals was higher than the median in the level II-1 segment in the PIPES survey (36.5 vs. 31, p = 0.1) and INTACT (15 vs. 12.5, p = 0.1). Likewise, all public hospitals administered regional and/or spinal anesthesia with ketamine and general anesthesia. Finally, the less frequently performed procedures were: cricothyroidotomy (1/7), pediatric abdominal wall defect (2/7), imperforate anus repair, and release of contractured limbs (3/7). The most frequent procedures are shown in Supplementary content 1.
Equipment: With regards to location, there were differences in the PIPES score (21 in the Piura province vs. 20 in the peripheral provinces, p = 0,35), and INTACT (10 vs. 8.5, p = 0.27). It should be noted that the PIPES (16 vs. 20.5) and INTACT (7 vs. 9) scores obtained in the Level II-2 hospitals were lower than those in Level Four hospitals (4/7) had central oxygen supply and only three (3/7) had endoscopes available. One (1/7) had problems with the availability of sterilization equipment (autoclave).
Supplies: The PIPES scores were slightly lower in the capital province versus the peripheral provinces (23 vs. 23.5), but not in INTACT (5 vs. 4). Both scores were lower in the Level II-2 hospitals versus the Level (PIPES [20 vs. 23.5, p = 0.8] and INTACT [3.5 vs 4.5, p = 0.81]).
Three hospitals (3/7) lacked eye protection equipment (safety goggles) and three (3/7) did not have any tracheostomy tubes. Two (2/7) had no protection facemasks and laparoscopy supplies.
Finally, the scores reported for each category of the PIPES and INTACT surveys of each hospital are shown in Supplementary content 1 and 2, respectively.
Additional criteria: With regards to the equipment and supplies section of the WHO Tool for Situational Analysis to assess essential and emergency surgical care, only three hospitals (3/7) had cricothyroidotomy equipment available and four had artery forceps (4/7). Two (2/7) had no IV infusion bags available, three (3/7) lacked equipment to insert chest tubes, one (1/7) did not have any splints for arms and legs, and one (1/7) had no needle holders. All had functional Macintosh laryngoscopes (adult and pediatric), retractors (spreaders), scissors, Magill forceps (pediatric and adult), garbage cans and soap.
Answers to short questions: Nine people said that the most common surgical training required was laparoscopic surgery. In the Level hospitals, the most frequent surgeries performed were cesarean section, appendectomy, hernia repair, and cholecystectomy. In Level II-2 the most frequent procedures were appendectomy, cholecystectomy, cesarean section, exploratory laparotomy due to abdominal trauma. In the Level hospital, the most frequent surgeries were appendectomy, cholecystectomy, exploratory laparotomy due to bowel obstruction and cesarean section. Moreover, in five hospitals (5/7) none of the surgical specialists received any basic or advanced training in trauma. All the respondents expressed a positive perception to the administration of these surveys. The reasons argued and the distances to the respective referral hospitals are shown in Table 2.
Table 2 Answers to short questions of the survey in public hospitals in the Piura region.
| Province/ Question | Talara Hospital | Morropón Hospital | Sullana Hospital II-2 | Piura Hospital II-2 | Piura Hospital | Paita Hospital | Piura Hospital |
|---|---|---|---|---|---|---|---|
| Requirement for surgical training | Laparoscopic surgery | Resuscitation | Bariatric, advanced laparoscopic surgery | Neurosurgery | Laparoscopic surgery | Laparoscopic surgery, patient with cardiovascular comorbidities | Laparoscopic surgery |
| Trauma care training | None of the members received training | None of the members received training | One staff member received ATLS training | None of the staff members received training | None of the members received training | No trauma care training (ATLS) | Surgeons in the emergency department received ATLS training |
| Distance to the nearest referral hospital * | 120 km (2 hours approximately) | 64.2 km (60 minutes) | 39.6 km (44 minutes) | 6 km (15 minutes) | 2.3 km (7 minutes) | 61.2 km (1 hour) | 217 km (3 hours) |
| Reasons for usefulness of the survey for the hospital and the surgical department or service | For planning and scheduling | For improving quality of service via improved processes | Learning about the work conditions and infrastructure and improving the patients' conditions | Identify the capacity and materials available in the hospital | Identify strengths and weaknesses | Fostering the development of the surgical center and perioperative management of patients | Helps to correct deficiencies and improving patient service |
Notes: ATLS: Advanced Trauma Life Support. *The travel time to the nearest referral hospitals was estimated using Google Maps.
Source: Authors.
DISCUSSION
The Piura province (capital province) is the most populated province in the region, accounting for 43 % of the population and also comprises the capital of the region. 13 The trauma care capacity of public hospitals in this province was larger than the peripheral provinces, indicating intraregional inequalities.
The inequality in the Peruvian regions with regards to territorial variables such as altitude, capital versus interior of the region and rural environment was already highlighted. Hence, there was a non-equitable distribution in terms of access to services between the population in the capital provinces of the regions versus the population in the hinterlands, notwithstanding the fact that there was a decline in the population with no access to water, sewage and electricity between 1993 and 2007. 17 Moreover, the variation coefficient for such access was higher for districts than for regions; and, following the economic growth, the level of inequality increased in both cases. 17
There was also an inverse correlation between poverty and urban development; growth had a positive influence on cities or areas in the vicinity of the capitals. 17 As illustrated in Figure 2, all public hospitals located in the different capitals of five provinces of the region were in the Coast (at less than 500 m over sea level). 18 Consequently, three provinces lacked public healthcare facilities as hospitals, two of which are the most remote provinces from the regional capital. Such is the case for the Ayabaca and Huancabamba provinces, with capitals located in the sierra of the region (a geographical area with an altitude above 500 m above sea level), specifically, the Quechua region (2,300-3,500 m above sea level) and the maritime Yunga region (500-2,300 m above sea level), respectively. 18 Fortunately, the infrastructure of the hospitals for these two provinces is now under construction, including a third facility for the Huarmaca district located in the Huancabamba province; however, access by road is difficult. 19
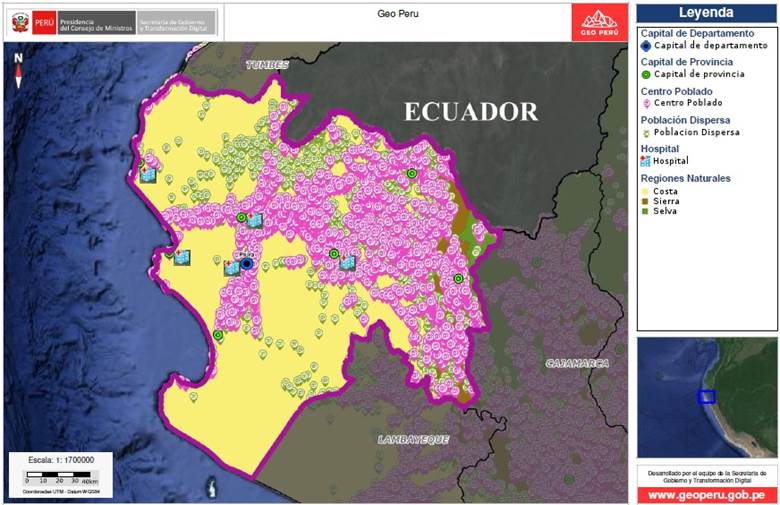
Source: Authors, based on the National Platform of Geo-Referenced Data - GeoPerú.
Figure 2 Location of public hospitals with surgical care with respect to the natural region, populated areas and scattered population in the Piura region.
Higher total scores were recorded from both surveys in Level II-2 hospitals, which are higher complexity than Level 16 However, in the categories of supplies and equipment, both scores of Level II-2 hospitals were lower than in the Level II-1. These differences may be because both Level II-2 hospitals and two of the Level II-1 hospitals belong to different public agencies, with separate financing and supplies coverage. This showed that shortages may also affect the higher complexity hospitals. Finally, the availability of cricothyroidotomy equipment must be improved in most public hospitals.
This study lays the foundation to suggest urgent infrastructural improvements to the leaders of the various public institutions in highly important areas such as water supply, around-the-clock availability of CT-scanners and blood banks in the hospitals serving the peripheral provinces. The coverage of supplies and equipment should be extended, particularly to Level II-2 hospitals. Likewise, training in trauma care and laparoscopic surgery should be included in the surgical services of all public hospitals in the region. The authors believe that it will be useful to share the results of the survey with each participating hospital in order to facilitate the implementation or remedial actions to correct the shortfalls identified.
The PIPES and INTACT surveys conducted in Bolivia reported that the surgical capacity indexes (departments of Potosí and Santa Cruz) and trauma care (Potosí) of urban institutions were higher than in the rural institutions. 20,21 Likewise, over fifty percent of the surgeons and anesthesiologists in Potosí work in urban institutions; and, in the case of Santa Cruz, several rural institutions did not have an anesthesiologist available. In the Piura region, all the surgical care centers were in urban areas. Similarly to Potosí, the most needed training was in laparoscopic surgery.
One of the limitations of this study was that it was only conducted in public hospitals, and hence the number of surgical specialists in the region was not estimated. Moreover, the short answers to the training needs were given by specialists in different surgical specialties. Hence, any future survey should seek answers to these questions from a member of each basic specialty involved in surgical care. Another important limitation due to the small sample of institutions assessed is the significant potential for type II error in the statistical analysis. Hence the results are preliminary. However, further analysis of the problem areas identified in a future research shall include the public and private hospitals in the region, with a larger number of facilities assessed to enable a more robust statistical analysis. Finally, one item in PIPES considers the category "regional anesthesia blocks", which includes both peripheral and neuraxial blocks, which may result in an overlap with the category of spinal anesthesia in the same survey.
In conclusion, this study makes an initial assessment of the surgical and trauma care capacities in a Peruvian region, identifying inequalities in trauma care capacity among the public hospitals in the region. Moreover, the most significant weakness was the hospital infrastructure. Urgent actions are needed to overcome the existing deficiencies in infrastructure, equipment, and supplies of various healthcare institutions, including building hospitals in two of the most geographically remote provinces, considering the difficulties for access and the scattered population. Finally, training shall be provided in the areas indicated by the health practitioners.
ETHICAL RESPONSIBILITIES
Endorsement of the ethics committee
The study was endorsed by the Ethics in Research Committee of the School of Health Sciences of the Universidad Nacional de Piura (Perú), under minutes dated March 26, 2021.
Protection of persons and animals
The authors declare that this study is a research in healthcare systems.
ACKNOWLEDGEMENTS
Contributions by the authors
RMG: The author developed the study project, participated in the administration of surveys, visited the public hospitals included in the study and approved the final report.
CSZ: The author participated in the administration of the surveys, visited the public hospitals included in the study, prepared and approved the final report.
RCZV, DPGC, MAOM, JCPP, EER, AHVA, JSCT, SJAU, RDR, YMMV: The authors completed the study survey and approved the final report.

