











 text in
text in  English (pdf)
English (pdf)
 Article in xml format
Article in xml format Article references
Article references
 Send this article by e-mail
Send this article by e-mail Cited by SciELO
Cited by SciELO  Cited by Google
Cited by Google  Similars in
SciELO
Similars in
SciELO  Similars in Google
Similars in Google 
 Permalink
Permalink
INTRODUCTION
Technological developments and breakthroughs in the various health domains, in addition to the growing relevance of patient-centered care over the past few years, have led healthcare stakeholders and scientific societies to search assertive strategies that initiate and maintain an open dialogue between doctors and patients, on the adequate use of diagnostic tests, treatments, or health technologies.
Bases on such need, the American Board of Internal Medicine [ABIM]), launched in 2012 a program called Choosing Wisely. The original program focused on identifying low value tests and therapies; i.e., which fail to contribute with any additional benefit to the patient and hence may result in waste of resources and harm. Afterwards, they looked for partnerships with other medical societies so that each developed five recommendations that were based on scientific literature. Since the Choosing Wisely initiative was launched, over 8o scientific societies have developed recommendations and 18 additional countries have become involved. 1,2 Later, Canada adopted Choosing Wisely International (CWI) in order to strengthen a network for cooperation among national initiatives to be implemented based on lessons learned and technical support to the countries that are just beginning this journey.
The Colombian Association of Scientific Societies (ACSC) identified this international initiative as a sound approach to highlight the urgent need of adopting self-regulatory powers previously enacted under the Health Statutory Law and according to other government regulations. Thus, the initiative enables the development of concrete strategies by suggesting the rational use of health technologies which could be ineffective or even harmful to patients.
In Colombia, the work team decided to call this initiative "Choosing Wisely -Caring from knowiedge". As a result, each scientific society is required to prepare a list with five "Do not do recommendations"; in other words, avoid any activities/actions that may impact patient safety and quality of care. Hence, the general objective of the initiative in Colombia is:
To implement in the largest possible number of scientific societies members of ACSC, the initiative of lists with five "Do not do" recommendations to reduce the use of ineffective or unsafe health technologies, and hence to contribute to healthcare quality improvement and patient safety.
Moving forward, the five principles of the initiative at the international level were adopted, in addition to the following statements in the light of the historical circumstances experienced in the country as a result of the implementation of the Healthcare sector Statutory Law. 3
Principles of the Choosing Wisely initiative adopted in Colombia under the Choosing Wisely project3,4:
That it is consistent with the protection of the fundamental right to health and patient safety.
That it is led by physicians pursuant to their obligation to self-regulation.
That it is patient-centered and its implementation should be agreed with the patient.
That it is multi-professional since compliance requires the involvement of various health professions, besides medicine.
That it is evidence-based.
That it is transparent; i.e., should be carried out avoiding the participation of individuals with conflicts of interest.
Following is the paper prepared by the Colombian Society of Anesthesiology and Resuscitation (S.C.A.R.E.), which brings together the anesthesiologists in the country and allowed for the consolidation of the five recommendations considered to be relevant for the practice of anesthesia in the country. The expectation is to be able to implement this project throughout the healthcare institutions.
The final paragraph of this article discusses the roadmap for its implementation and dissemination.
METHODOLOGY
Once the work to be done was clear, each scientific society internally defined its own strategy for making their recommendations. Figure 1 presents the strategy used by our society.
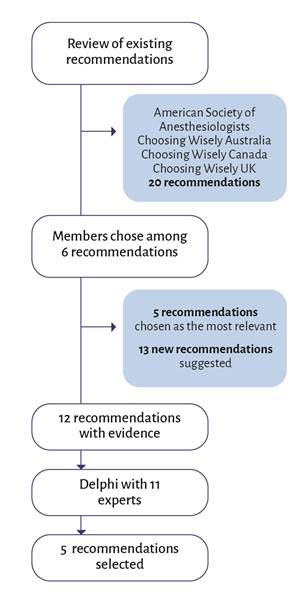
S.C.A.R.E. compiled the recommendations of the American Society of Anesthesiologists, Choosing Wisely Australia, Choosing Wisely Canada, and Choosing Wisely UK Anaesthesia. Naturally, the recommendations were specifically related to the management of anesthesia. This initial selection was consolidated in a QuestionPro survey form 5; the form was forwarded to the anesthesiologists members of S.C.A.R.E. to select the most important recommendations, or to suggest new recommendations with their respective evidence.
The results of the survey were used to identify some additional recommendations and a short list of twelve recommendations was developed. Then, using the Delphi methodology, a validation process took place with a selected group of experts. Two fundamental criteria were the basis to decide the composition of the group of experts: first, clinical experience; and second, the absence of any relationships that could result in a conflict of interests. The ACSC suggested some criteria to identify potential conflicts of interest and these were the criteria used. The following were considered conflicts of interest 6:
Full time employee in non-clinical activities of the Ministry of Health, or State, District, or Municipal health secretariats.
Full time employee in non-clinical activities of a healthcare provider institution (EPS) or agency responsible for payment.
Full time employee of a manufacturer or distributor of medical technologies (medicines, devices, medical equipment, medical supplies).
owner or Board Member of any the above-mentioned companies.
A team of eleven experts was organized in accordance with the above criteria; prior to the meeting, each expert received a document with a summary of the results accomplished so far and the preliminary proposals for do-not-do recommendations. The experts had the opportunity to make comments to these preliminary proposals from April 8 through 18, 2022. A QuestionPro questionnaire was used to indicate the experts' agreement with the inclusion of these recommendations. This initial review and ballot was called the preliminary round.
The meeting of experts was held online on April 22, 2022. On the day of the meeting, the information collected by the developer team was presented again, together with the results of the preliminary round. First, a ten-minute discussion was opened for each recommendation - maximum one minute per participant - for a total of thirty minutes, to analyze the recommendations over which there was no agreement for its inclusion or exclusion. The items over which there was disagreement in the preliminary round were subject to vote with two rounds. Before the start of the second round, a discussion took place on the recommendations over which there was no agreement; this discussion lasted again for ten minutes, with a maximum of one minute per intervention.
After the decision was made regarding the recommendations to be included, these recommendations were prioritized to identify the five recommendations to be submitted as Wise Decisions in Anesthesiology. The prioritization was done using QuestionPro, via a list to classify the five most important recommendations according to each expert. This information was analyzed in terms of percentages to establish the five best rated recommendations in the group. This methodology was the basis to select the recommendations listed in Table 1.
Table 1 Recommendations of Wise Decisions in Anesthesiology.
| Recommendation | Commentary |
|---|---|
| Do not allow prolonged fasting in patients undergoing elective surgery; unless there is a contraindication, consider the intake of clear fluids up to two hours before surgery. | Randomized, controlled trials have shown that clear fluid intake up to two hours and light solids up to six hours before the induction of anesthesia is safe and improves the patient's wellbeing. 7 |
| Do not require "routine" laboratory tests (electrocardiogram, chest X-rays, spirometry, CBC, coagulation tests), in ASA I or II patients undergoing a low risk procedure and when no blood loss is anticipated. | By reducing the number of unnecessary tests, there is a reduction in the number of adjournments and delays; it is also considered a cost-effective measure that reduces healthcare costs. 8,9 A pilot study on the elimination of routine preop tests in ambulatory surgery, showed that the number of adverse events did not increase. 10 |
| Do not administer supplemental oxygen in regional anesthesia in healthy patients, unless sedatives are used or when the oxygen saturation is below 90 %. | In ASA I-III patients under spinal anesthesia, the routine use of oxygen supplementation is nor necessary, due to the low incidence of intraoperative hypoxemia (oxygen saturation 90 %). 11 The use of oxygen supplementation to healthy term pregnant mothers during elective cesarean section under regional anesthesia failed to show any benefit or to be detrimental to the mother or the fetus. 12
However, in some geographies with an altitude over 2600 meters above sea level, this figure could be higher and a 92% oxygen saturation should be considered as the baseline. 13,14 |
| Do not administer packed red blood cells to a young patient with no comorbidities, no blood loss, with a hemoglobin (Hb) ≥ 7 g/dL, except if the patient is symptomatic or hemodynamically unstable. | The updated guidelines of the American Society of Anesthesiology recommend red blood cells transfusion if the Hb is < 7 g/dL in most of the asymptomatic patients with no cardiovascular disease. Red blood cells transfusion should not be exclusively determined based on the level of hemoglobin. 15
In a study in an intensive care setting a restrictive group with transfusion if the Hb was below 7 g/dL to maintain it at 7-9 g/dL was compared against a liberal group, with a level for transfusion of Hb < 10 g/dL to be maintained between 10-12 g/dL, there was no statistical difference in the 30-day mortality between the two groups. 16 Most allogeneic red blood cells transfusions may be avoided in patients with a level of hemoglobin around 7-8 g/dL. 17 |
| Do not administer fresh frozen plasma (FFP) prophylactically during the perioperative period of patients without active bleeding. | EThe prophylactic use of FFP prior to an invasive procedure with altered coagulation tests, but without active bleeding, is not supported by good quality evidence; the conclusion is that altered coagulation tests are not a predictor for bleeding 18; there is no evidence supporting the prophylactic use of plasma. 19
Any personal or family history of bleeding, the use of medications, and the risk of bleeding during the procedure, are more important indicators than routine coagulation tests. 20 |
Source: Authors.
Disclosure of the results and next steps moving forward
After collecting all of the recommendations from the pioneer societies that replied to the first call of the ACSC, and submitting them in a specially designed form, a kickoff webinar was held on May 5, 2022, which was widely broadcasted to ensure participation of the different stakeholders in healthcare. The session began with a conference on the international experience by Dr. Wendy Livingston, followed by a short presentation of a summary of the recommendations of each society by the developer group. On July 12, S.C.A.R.E held an online meeting to introduce the recommendations in anesthesiology and to answer questions from the audience.
However, this is not the end of the journey. The next step is the implementation of the recommendations in the healthcare institutions, measuring the results before and after their implementation, to evidence the benefits achieved; simultaneously, the dissemination of the recommendations to patient organizations and education institutions, in order to promote the initiative among the organizations responsible for the development of human resources. The ACSC shall continue to lead this activity, inviting and advising other scientific societies to encourage their participation. S.C.A.R.E is particularly interested in moving forward in the areas of our specialty where recommendations may be issued on specific topics such as: pediatric anesthesia, obstetric anesthesia and regional anesthesia, inter alia.
ACKNOWLEDGMENTS
Contributions by the authors
LMGB and JRE: Conception of the strategy, planning of the study, preparation of the draft, drafting and revision and approval of the manuscript.
NFSB: Planning of the study, development of the research protocol, statistical analysis of the results, drafting, revision and approval of the final manuscript.

