










Serviços Personalizados
Journal
Artigo
 Inglês (pdf)
Inglês (pdf)
 Artigo em XML
Artigo em XML Referências do artigo
Referências do artigo
 Enviar este artigo por email
Enviar este artigo por emailIndicadores
-
 Citado por SciELO
Citado por SciELO -
 Acessos
Acessos
Links relacionados
 Citado por Google
Citado por Google -
 Similares em
SciELO
Similares em
SciELO  Similares em Google
Similares em Google
Compartilhar

 Permalink
PermalinkBiomédica
versão impressa ISSN 0120-4157versão On-line ISSN 2590-7379
Biomédica v.25 n.2 Bogotá jun. 2005
Malassezia yeast species isolated from patients with dermatologic lesions
Sandra Rincón 1, Adriana Celis 1, Leticia Sopó 2, Adriana Motta 3, María Caridad Cepero de García 1
1 Centro de Investigaciones Microbiológicas, Universidad de los Andes, Bogotá, D.C., Colombia.
2
Laboratorio Especializado de Micología Médica, Edificio El Bosque, Bogotá, D.C., Colombia.3
Universidad El Bosque, Bogotá, D.C., Colombia; Hospital Simón Bolívar, Bogotá, D.C., Colombia.Introduction. Yeasts of the genus Malassezia form a normal component of skin flora, but are also associated with several dermatological disorders. Since 1996, the description of new species in this genus have led to new questions about their epidemiology and pathogenicity.
Objective. Herein, the frequency of Malassezia species in individuals with pityriasis versicolor, atopic dermatitis, seborrhoeic dermatitis, seborrhoeic dermatitis was compared in HIV patients and healthy individuals. Three body sites were selected for examination -head, thorax, and upper and lower extremities.
Material and methods. The 154 Malassezia species were isolated from 112 individuals and grouped as follows: 39 with seborrhoeic dermatitis (20 were HIV-positive patients), 18 with pityriasis versicolor, 18 with atopic dermatitis and 37 without dermatological leisions. HIV patient samples were examined microscopically, and specimens from both patients and healthy subjects were cultured on modified Dixon agar medium. Subsequently, isolates were identified by macroscopic, microscopic and physiological characteristics.
Results. The most commonly isolated species were Malassezia globosa (37.5%), M. sympodialis (31.3%) and M. furfur (31.3%). Malazzerzia globosa predominated in patients with pityriasis versicolor (67%) and in HIV-positive patients with seborrhoeic dermatitis (85%). In non-HIV patients with atopic dermatitis or seborrhoeic dermatitis, M. furfur and M. restricta were isolated in 72% and 26% of the cases, respectively.
Conclusion. Several conclusions were evident. First, Malassezia species was present in subjects with and without dermatological pathologies. Second, the species frequency in the sampled population differed from frequencies reported from other geographic areas. Third, Malassezia globosa was involved at high frequency in patients with dermatological pathologies, suggesting a higher pathogenicity of this species. Additional studies on each species are recommended to clarify their pathogenic roles in association with HIV-positive and normal subjects.
Keywords: Malassezia, tinea versicolor, seborrheic dermatitis, HIV, atopic dermatitis
Especies de Malassezia aisladas de pacientes con lesiones dermatológicas
Introducción. Las levaduras del género Malassezia forman parte de la flora normal de la piel y se asocian con varios tipos de lesiones dermatológicas. Desde 1996, la descripción de nuevas especies dentro de este género planteó numerosos interrogantes sobre su epidemiología y patogenicidad.
Objetivo. El fin de este trabajo fue encontrar la frecuencia de las diferentes especies de Malassezia en individuos con pitiriasis versicolor, dermatitis atópica, dermatitis seborreica, dermatitis seborreica en pacientes positivos para VIH, y en individuos sin lesiones a partir de tres zonas corporales (cabeza, tórax, extremidades inferiores y superiores).
Materiales y métodos. Se identificaron 154 aislamientos de especies de Malassezia de 112 individuos: 39 con dermatitis seborreica de los cuales 20 eran positivos para VIH, 18 con pitiriasis versicolor, 18 con dermatitis atópica y 37 individuos sin lesión dermatológica (controles). Las escamas de piel de los pacientes se observaron microscópicamente y las muestras de pacientes y controles se cultivaron en agar Dixon modificado. Posteriormente, se observaron las colonias y se identificaron según sus características macroscópicas, microscópicas y fisiológicas.
Resultados. Las especies más frecuentemente aisladas en el total de los grupos estudiados fueron: Malassezia globosa (37,5%), M. sympodialis (31,3%) y M. furfur (31,3%). M. globosa predominó en los aislamientos de pacientes con pitiriasis versicolor (67%) y en pacientes positivos para VIH con dermatitis seborreica (85%). En pacientes con dermatitis atópica y dermatitis seborreica sin diagnóstico de VIH, se aislaron M. furfur y M. restricta en el 72% y el 26% de los casos, respectivamente.
Conclusiones. Las diferentes especies de Malassezia pueden aislarse de pacientes con lesiones dermatológicas o sin ellas. Además, la frecuencia de especies en la población muestreada difiere de lo reportado en otras zonas geográficas. Se destaca la alta frecuencia de M. globosa en pacientes con lesiones lo que podría indicar la mayor patogenicidad de esta especie. No obstante, se requieren estudios adicionales para determinar el papel de las diferentes especies del género Malassezia, asociadas con estas patologías.
Palabras clave: Malassezia, pitiriasis versicolor, dermatitis seborreica, VIH, dermatitis atópica.
Lipophilis yeasts of the genus Malassezia are part of the skin´s normal flora which under the influence of certain predisposing factors can give rise to different dermatological disorders (1-3). Nowadays, next to pityriasis versicolor, some authors associate the presence of Malassezia yeasts with other dermatological disorders such as atopic dermatitis, seborrhoeic dermatitis, some forms of folliculitis, psoriasis, Gougerot-Carteaud reticulated confluent papillomatosis, annular centrifugal erythema, seborrhoeic marginal blepharitis, intertrigo, onychomycosis and neonatal acne. In addition, opportunistic systemic infections of Malassezia yeasts have been reported in neonates to whom lipidic infusions have been administered, and also in patients in intensive care units (1-4).
Studies on Malassezia cutaneous isolates from healthy humans and animals indicate that M. sympodialis is the commonest species in healthy and diseased skin. M. globosa is frequently isolated from pytiriasis versicolor and seborrhoeic dermatitis, as well as from healthy skin. M. restricta, together with other species, has been associated with dandruff and seborrhoeic dermatitis of the scalp and face, respectively. Both M. slooffiae and M. pachydermatis are infrequently found on human skin, while M. obtusa and M. furfur are rarely isolated from these body sites. The species M. furfur and M. pachydermatis have also been isolated from systemic infections (2,5-7).
Despite reports in 1996 describing four new species for the genus (2), and development of a protocol to identify species by conventional laboratory tests (2,8,9), there have been studies in other countries, not in Colombia, aimed for the determination of species usually found in association to certain pathologies (10-19).
The goal of this study was to determine the relative presence of Malassezia species ocurring on both patients with dermatologic lesions of atopic dermatitis, seborrhoeic dermatitis, seborrhoeic dermatitis in HIV+ patients, pityriasis versicolor, and from individuals with no lesions (healthy controls) on three body sites (head, thorax and lower and upper extremities). As far as we know, this is the first report of Malassezia isolated from random patient populations in Bogotá, Colombia.
Materials and methods
Studied population
A total of 112 persons residing in Bogotá, Colombia, were included in the study: 75 with skin lesions, of which 18 corresponded to atopic dermatitis, 39 with seborrhoeic dermatitis, and 20 of which were HIV-infected patients, 18 had pityriasis versicolor and 37 healthy control individuals. The studied population consisted of 65 men and 47 women, ranging in age from 4 to 60 years. Individuals were sampled from August 1999 to December 2001. Samples were collected from clinically selected patients who had previously attended dermatological consultation or had been hospitalized in the Simón Bolívar Hospital (Bogotá, Colombia).
Sample-collection and processing
Samples were taken from affected areas by scraping with a disposable scalpel and collecting the scrapings in a sterile Petri dish or in between sterile slides sealed with tape, all of which were transported to the laboratory and processed in less than two hours. A portion of the sample was used for direct examination with 20% KOH plus Parker blue-black ink while the remaining portion was homogenized in 2 ml solution of water plus 0.05% Tween 80 and used for culturing. The contents were vortexed and 0.5 ml were inoculated onto modified Dixon-Agar plates (3.6% malt extract, 0.6% peptone, 2% desiccated ox bile, 1% tween 40 0.2% glycerol, 0.2% oleic acid, 1.2% agar, 0.5 g/L chloramphenicol and 0.5 g/L cycloheximide) (2,8), and then incubated at 32±2°C for seven days.
Samples were also taken from control volunteers without lesions and who did not receive oral or topical anti-fungal treatments. No direct examinations were done on these volunteers. Samples were collected according to the body area and the number of sites was proportional to samples taken from patients with dermatologic lesions. Samples were collected by rubbing the area with sterile swabs dampened in 2 ml water plus 0.05% Tween 80, which were introduced in tubes with the same solution. In our first study, we showed that no statistically significant differences occurred between both methods (swabbing and scraping) (20) (García MC, Gutiérrez NE, Sopó L. Abstracts of the 96th General Meeeting of the American Society for Microbiology, New Orleans, Louisiana, May 19-23, 1996. Abstract F-31:79). Cultures were procesed as described above.
Isolation and identification of colonies compatible with Malassezia
Cultures were observed by means of the stereomicroscope and colonies compatible with the genus Malassezia were selected. The different morphotypes (different colony characteristics) observed were subcultured for species identification. The isolates were maintained under liquid nitrogen. The conventional tests described by Guého et al., Guillot et al., and Mayser et al., (2,8,9) were performed in order to confirm the genus and species. The identification scheme used in this study is summarized in
figure 1.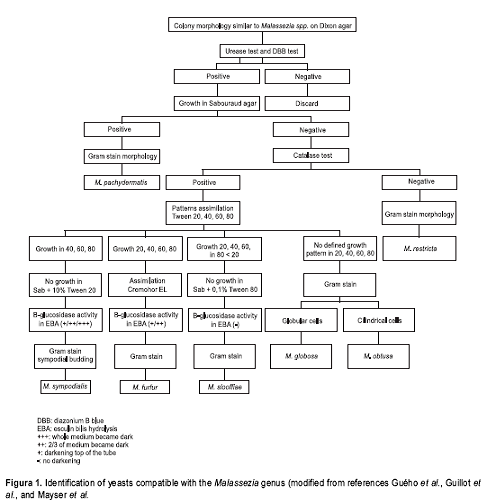
Three sampling groups were formed, namely group I corresponding to samples from head (scalp, face and neck), group II were samples from the thorax and group III contained isolates from the extremities (upper and lower).
Results were analyzed by Fisher's exact test.
Results
All samples taken from the 75 patients were positive for Malassezia yeasts upon direct examination. Samples taken from the 112 individuals (75 with lesions, 37 healthy controls) yielded 154 isolates, as more than one colony was observed in certain primary cultures. The distribution of the Malassezia species isolated is presented in
table 1. Six Malassezia species could be identified from patients and controls, but 22 isolates could not be identified (Malassezia spp.). Three species, M. globosa (37.5%), M. sympodialis (31.3%), and M. furfur (31.3 %) were predominant in the group of isolates as a whole. When separating isolations by groups (patients and controls) a significant difference was noticed for M. globosa, which was isolated from 48% of the patients and from 16.2% of the controls (p=0.003). Otherwise, the various species were represented in equal amounts in both patients and controls.
The distribution of the Malassezia species according to the body site sampled irrespective of the dermatological condition is shown in table 2. In group I, the various species were isolated from both patients and controls. However, with the exception of M. pachydermatis, these differences were statistically not significant. On the contrary, when samples in groups II and III were tabulated it was noticed that differences existed according to the species isolated. Thus, in group II, statistically significant differences were seen for M. globosa between patients (45.2%) and controls
(7.7%) (p=0.035). Inverse figures were noticed for Malassezia spp. isolates, namely 38.5% in controls vs. 9.7% in patients (p=0.035). In group III no statistically significant differences ocurred for M. pachydermatis and Malassezia spp. isolated from both groups patients and controls. The Malassezia furfur isolates were obtained only from patients, but the small number of samples in this group (n=14) precludes proper interpretation. It can be seen that the largest number of species were isolated from group I, namely 6 identified species and non-identified Malassezia spp.
We attempted to determine the role of the Malassezia species in the pathogenesis of the various skin disorders. The species isolated from patients and controls were compared according to the different dermatologic entities. In atopic dermatitis, statistically significant differences were seen for M. furfur between patients (13/18) (72%) and controls (8/37) (22%) (p=0.0002). Additionally, significant differences were observed in seborrhoeic dermatitis for M. restricta in controls (2/37) (5.4%) and patients (5/19) (26%) (p=0.016), in HIV-positive patients M. globosa was isolated from 17/20 (85%) of the patients vs. 6/37 (16%) of the controls (p<0.01), and M. restricta ocurred in 5/20 (25%) patients and 2/37 (5.4%) controls (p=0.022). In pityriasis versicolor significant differences were noticed for M. globosa between patients (12/18) (67%), and controls (6/37) (16%) (p<0.01).
Discussion
The role of these lipophilic Malassezia yeasts in skin problems is controversial, although a number of studies have been undertaken to investigate the ecology and the epidemiology of the different Malassezia species in these pathological disorders, as well as of their presence on healthy skin (1-4,10-19). New questions have been raised about the significance and relationships of the Malassezia species in clinical infections (1,4), this is due to factors such as the recent description of new species (2,21,22), the isolation of Malassezia as part of the microbial community of human skin rich in sebaceous glands (1,2,6,16), and the variability in colonization according to different age groups and sebaceous glands activity (15,19,23).
Our results indicate that the most frequently isolated species from all populations studied were M. globosa (37.5%), M. sympodialis (31.3%) and M. furfur (31.3%). In accordance with previous reports, the remaining species M. restricta, M. obtusa, and M. pachydermatis were isolated less frequently (10,11,15,18).
We found isolates that did not correspond to previously reported patterns in the standard identification protocols (2,8,9), and these strains were grouped as Malassezia spp., a category that has been reported in previous studies as well (10,23,24). Recently, other new Malassezia species have been reported, namely M. japonica (21) and M. dermatis (22), and these may be similar to some of the unclassified species referred above.
Our results reveal the predominance of M. globosa (67%) in patients with pityriasis versicolor (p<0.01), which is in accordance with reports from various authors (10-12,17). Many reports consider that M. globosa is the etiologic agent of pityriasis versicolor isolated from 25-97% of the cases (6, 9-12,17,18). However, others have reported M. sympodialis as the most frequently isolated species (40-62.7%) (14,15).
Moreover, we have found different implications of Malassezia-related diseases in HIV-infected patients, in which the main pathology is not pityriasis versicolor, but seborrhoeic dermatitis with M. globosa as the predominant etiologic agent (85%) (p<0.01), followed by M. restricta (25%) (p=0.022). In contrast, in a previous study conducted in our laboratory, Malassezia spp. colonization was evaluated in HIV-infected patients from the same hospital, M. restricta (46%) was found to be the prevailing species (13). The difference could be explained by the sampling period and year, and because of the cutaneous microbial communities occurring on these patients (15,19). Nevertheless, the results of this study are interesting and indicate a superior pathogenic capacity for M. globosa, which call for additional study in this group of HIV-infected patients.
M. furfur isolated in 72% of the patients with atopic dermatitis has statistically significant differences (p=0.002), a finding that is also of interest. Although few studies have been conducted in this respect, our data are similar to those of Nakabayashi et al. in Japan (10) and differs from others, which report M. sympodialis as the most frequently isolated species (53%) in Canada (15) and 40% in Sweden (Faergemann J, Sandstrom M, Back O, Scheynius A, Samhult T, Linder M. Abstracts of the 15th Congress of the International Society for Human and Animal Mycology, ISHAM. San Antonio, Texas, May 25-29, 2003, Abstract 368:459). However, the heterogeneous nature of this disease has been recognized and it has been suggested that Malassezia yeasts act as allergens than as etiological agents (1,6,25).
Significant differences were found (p=0.016) in the isolation of M. restricta (26%) from patients with seborrhoeic dermatitis which is in accordance with studies performed in Spain where M. restricta was isolated in 43%-63.9% of the patients evaluated (11,12). Once more, this differs from other reports, as follows: M. globosa, 45% in Canada (15); M. sympodialis, 38.5%, and M. slooffiae, 34.6% in Mexico (18); M. furfur and M. globosa in equal percentages (21%) in Japan (10); M .obtusa, 35%, and M. sympodialis, 30% in other group of patients in Sweden (Faergemann J, Sandstrom M, Back O, Scheynius A, Samhult T, Linder M. Abstracts of the 15th Congress of the International Society for Human and Animal Mycology, ISHAM. San Antonio, Texas, May 25-29, 2003, Abstract 368:459).
We also evaluated (
table 2) the relation between the isolated species and the body sites head, thorax and upper and lower extremities, groups (I, II and III). Our results differ from other reports in the distribution of the species on body sites in different geographic areas of Spain, Japan and Canada (10-12,15,19). These differences are probably related to the ethnic origin of the population, the corporal zones, and the age of the individuals tested, as suggested by several authors (4,15,19). Our findings suggest the need of additional studies to determine the ecology of the different species in healthy skin and the clinical significance of the dermatoses associated with these yeasts, as well as the urgency of new studies to evaluate the differences in susceptibility to antifungal compounds and intra-specific differences using molecular techniques.
Conflict of interests
The authors declare that they have no competing interests.
Financial support
This study was supported by a grant of Colciencias (Cod.: 1204-04-10175).
Acknowledgments
We would like to thank Ángela Restrepo who provided invaluable assistance in analyzing the results and for the critical review of the manuscript, and Orlando Martínez for his help in the statistical analysis.
References
1. Guého E, Boekhout T, Ashbee HR, Guillot J, van Belkum A, Faergemann J. The role of Malassezia species in the ecology of human skin and as pathogens. Med Mycol 1998;36(Suppl.1):220-2. [ Links ]
2. Guého E, Midgley G, Guillot J. The genus Malassezia with description of four new species. Antonie van Leeuwenhoek 1996;69:337-55. [ Links ]
3. Marcon MJ, Powell DA. Human infections due to Malassezia spp. Clin Microbiol Rev 1992;5:101-19. [ Links ]
4. Midgley G. The lipophilic yeasts: state of the art and prospects. Med Mycol 2000;38(Suppl.1):9-16. [ Links ]
5. Guého E, Guillot J, Crespo E. Malassezia yeast infections: update. Mycoses 2001;44(Suppl.1):83. [ Links ]
6. Ashbee HR, Evans EG. Immunology of the diseases associated with Malassezia species. Clin Microbiol Rev 2002;15:21-57. [ Links ]
7. van Belkum A, Boekhout T, Bosboom R. Monitoring spread of Malassezia infections in a neonatal intensive care unit by PCR_mediated genetic typing. J Clin Microbiol 1994;32:2528-32. [ Links ]
8. Guillot J, Guého E, Lesourd G, Midgley G, Chévrier G, Dupont B. Identification of Malassezia species. A practical approach. J Mycol Méd 1996;6:103-10. [ Links ]
9. Mayser P, Haze P, Papavassilis C, Pickel M, Gruender K, Guého E. Differentiation of Malassezia species: selectivity of cremophor EL, castor oil and ricinoleic acid for M. furfur. Br J Dermatol 1997;137:208-13. [ Links ]
10. Nakabayashi A, Sei Y, Guillot J. Identification of Malassezia species isolated from patients with seborrhoeic dermatitis, atopic dermatitis, pityriasis versicolor and normal subjects. Med Mycol 2000;38:337-41. [ Links ]
11. Crespo V, Ojeda A, Vera A, Crespo A, Sánchez F, Guého E. Mycology of pityriasis versicolor. J Mycol Méd 1999;9:143-8. [ Links ]
12. Crespo V, Ojeda A, Vera A, Crespo A, Sánchez F. Aislamiento e identificación de Malassezia spp. en pitiriasis versicolor, dermatitis seborreica y piel sana. Rev Iberoam Micol 1999;16:16-21. [ Links ]
13. Mancera M, Motta A, Sopó L, De García M. Determination of Malassezia spp. in HIV+ and AIDS patients with seborrhoeic dermatitis diagnosis. Mycoses 2001;44(Suppl.1):71-2. [ Links ]
14. Gupta AK, Kohli Y, Faergemann J, Summerbell RC. Epidemiology of Malassezia yeasts associated with pityriasis versicolor in Ontario, Canada. Med Mycol 2001; 39:199-206. [ Links ]
15. Gupta AK, Kohli Y, Summerbell R, Faegermann J. Quantitative culture of Malassezia species from different body sites of individuals with or without dermatoses. Med Mycol 2001;39:243-51. [ Links ]
16. Aspiroz C, Moreno LA, Rezusta A, Rubio C. Differentiation of three biotypes of Malassezia species on human normal skin. Correspondence with M. globosa, M. sympodialis and M. restricta. Mycopathologia 1999;145:69-74. [ Links ]
17. Aspiroz C, Ara M, Varea M, Rezusta A, Rubio C. Isolation of Malassezia globosa and M. sympodialis from patients with pityriasis versicolor in Spain. Mycopathologia 2002;154:111-7. [ Links ]
18. Hernández-Hernández F, Méndez-Tovar L, Bazán- Mora E, Arévalo-López A, Valera-Bermejo A, López- Martínez R. Especies de Malasssezia asociadas a diversas dermatosis y a piel sana en población mexicana. Rev Iberoam Micol 2003;20:141-4. [ Links ]
19. Gupta A, Kohli Y. Prevalence of Malassezia species on various body sites in clinically healthy subjects representing different age groups. Med Mycol 2004;42: 35-42. [ Links ]
20. Gutiérrez N. Comparación de los recuentos de Malassezia furfur en individuos con y sin dermatitis seborreica (tesis). Bogotá, Colombia: Universidad de los Andes; 1995. [ Links ]
21. Sugita T, Takashima M, Komada M, Tsuboi R, Nishikawa A. Description of a new yeast species, Malassezia japonica, and its detection in patients with atopic dermatitis and healthy subjects. J Clin Microbiol 2003;41:4695-9. [ Links ]
22. Sugita T, Takashima M, Shinoda T, Suto H, Unno T, Tsuboi R et al. New yeast species, Malassezia dermatis, isolated from patients with atopic dermatitis. J Clin Microbiol 2002;40:1363-7. [ Links ]
23. Huérfano S, Rodríguez S, Cepero de García MC. Frecuencia de colonización and distribución de especies de Malassezia aisladas como flora normal en población de 0-60 años (tesis). Bogotá, Colombia: Universidad de los Andes; 1998. [ Links ]
24. Cepero de García MC. Caracterización morfológica, fisiológica y genética de aislamientos humanos nativos de Malassezia spp. (tesis). Bogotá, Colombia: Universidad de los Andes; 1999. [ Links ]
25. Jensen-Jarolim E, Poulsen LK, With H, Kieffer M, Ottevanger V, Stahl Skov P. Atopic dermatitis of face, scalp and neck: type reaction of the yeast Pityosporum ovale. J Allergy Clin Immunol 1992;89:44-51. [ Links ]

