










Services on Demand
Journal
Article
 Spanish (pdf)
Spanish (pdf)
 Article in xml format
Article in xml format Article references
Article references
 Send this article by e-mail
Send this article by e-mailIndicators
-
 Cited by SciELO
Cited by SciELO -
 Access statistics
Access statistics
Related links
-
 Cited by Google
Cited by Google -
 Similars in
SciELO
Similars in
SciELO -
 Similars in Google
Similars in Google
Share

 Permalink
PermalinkBiomédica
Print version ISSN 0120-4157On-line version ISSN 2590-7379
Biomédica vol.26 suppl.1 Bogotá Oct. 2006
Effect of knowledge and economic status on sandfly control activities by householders at risk of cutaneous leishmaniasis in the subandean region of Huila department, Colombia
Raúl H. Pardo 1, Alexander Carvajal 2, Cristina Ferro 1, Clive R. Davies 3
1 Laboratorio de Entomología, Subdirección de Investigación, Instituto Nacional de Salud, Bogotá D.C., Colombia.
2
Unidad de Entomología, Secretaría de salud Departamental del Huila, Neiva, Colombia.3
Department of Infectious and Tropical Diseases, London School of Hygiene and Tropical Medicine, London, United Kingdom.
Recibido: 22/08/05; aceptado: 13/12/05
Introduction.
Householder vector control measures can be encouraged by health promotion campaigns which take into account peoples attitudes and focus on key gaps in knowledge.Objectives. To describe household sandfly control practices in an endemic area of cutaneous leishmaniasis in the department of Huila, Colombia, and determine how these are influenced by attitudes, knowledge and socioeconomic status.
Materials and methods. A household questionnaire was applied to collect information on: demography, socioeconomic status, knowledge of cutaneous leishmaniasis and of sandflies and their role in transmission, and the control activities practiced. Indoor sandfly abundance was estimated by light trap collections.
Results. Amongst 249 interviewees, 86% knew about cutaneous leishmaniasis and 98% sand flies. 35% of interviewees who knew about cutaneous leishmaniasis practiced measures with the purpose of its control. This practice was higher amongst the 32% who knew that sand flies transmit cutaneous leishmaniasis. However, 82% of interviewees practiced sand fly control measures, and these were significantly associated with high sand fly abundance. Measures included smoke, bednets, and house spraying with insecticide or non-insecticidal substances. Householders using the high cost measures (bednets and insecticide) had the highest economic status.
Conclusions. Health education programmes should note that sand fly nuisance can initiate control measures, but that knowledge of the role of sand flies in transmission could enhance activities. The socioeconomic findings indicate that targeted bednet subsidies could reduce inequities in health status amongst cutaneous leishmaniasis endemic communities.
Key words: Psychodidae; Lutzomyia; health knowledge, attitudes, practice; prevention & control, leishmaniasis, Colombia.
Efecto del conocimiento y nivel socioeconómico sobre las actividades de control realizadas por la población en riesgo de adquirir leishmaniasis cutánea en la región subandina del departamento del Huila, Colombia
Introducción. Las medidas de control vectorial en el ámbito familiar pueden ser estimuladas por campañas de promoción en salud que tengan en cuenta los conocimientos y actitudes de la población con énfasis en vacíos claves en el conocimiento.
Objetivos. Describir las prácticas de control para flebótomos realizadas por las familias en un área endémica de leishmaniasis cutánea en el departamento del Huila, Colombia, y determinar cómo estas prácticas son influenciadas por las actitudes, conocimientos y el estatus socioeconómico.
Materiales y métodos. Se aplicó un cuestionario a nivel familiar para recolectar información sobre: demografía, estatus socioeconómico, conocimientos sobre leishmaniasis cutánea y sobre los flebótomos y su papel en la transmisión, y la práctica de actividades de control. La abundancia intradomiciliar de flebótomos fue estimada con trampas de luz.
Resultados. De 249 entrevistados, 86% conocían la leishmaniasis cutánea y 98% los flebótomos. 35% de los entrevistados que conocían la leishmaniasis cutánea practicaron medidas para su control. Estas prácticas fueron mayores, 32%, en las familias que conocían que los flebótomos transmiten la LC. Sin embargo, 82% de los entrevistados practicaron medidas de control para los flebótomos, y estas prácticas estuvieron significativamente asociadas con altas abundancias de flebótomos. Las medidas de control practicadas incluyeron humazo, toldillos, fumigación intradomiciliar con insecticidas o con sustancias no insecticidas. Las familias que usaron medidas de costo alto (toldillos e insecticidas) tenían el estatus económico más alto.
Conclusiones. Los programas de educación en salud deben considerar que la molestia sanitaria causada por los flebótomos puede iniciar la práctica de medidas de control y que el conocimiento del papel de los flebótomos en la transmisión puede aumentar estas actividades. Los resultados con relación al estatus socioeconómico indican que subsidios para adquirir toldillos pueden reducir desigualdades en salud en comunidades en donde la leishmaniasis cutánea es endémica.
Palabras clave: Psychodidae; Lutzomyia; conocimientos, actitudes y práctica en salud; prevención y control, leishmaniasis, Colombia.
Throughout the cutaneous leishmaniasis endemic regions of the Andean countries there are few vertically organized vector control programmes. House spraying activities by health ministry personnel tend to be sporadic, with limited coverage, and little formal evaluation (1). Hence, households in endemic zones can currently most effectively reduce their risk of cutaneous leishmaniasis by carrying out their own vector control measures. Whether such measures are taken could depend on a combination of factors –including the incidence of disease, the attitudes of the local people to the disease, knowledge of the possible control measures, and the ability to pay for the measures.
Knowledge of vector control measures for cutaneous leishmaniasis implies an understanding of the role of insects in its transmission. However, control activities could also be carried out simply to target the nuisance caused by sandfly bites, without any appreciation of their role in disease transmission. Hence, any investigation of sandfly control activities in endemic communities should determine the principal reasons for householder practices.
Previously reported surveys of knowledge, attitudes and practice amongst cutaneous leishmaniasis endemic communities throughout the world have focused mainly on factors related to the disease. Despite differences in questionnaire design and definitions, most reported studies have detected a relatively high (>75%) knowledge of the disease but relatively poor (<30%, in the majority of cases) knowledge of its control (2-10, Chappuis, F, Cavailler, P. Perception of Kala Azar among Pokot communities in Amudat, Eastern Uganda. Report: Epicentre, centre collaborateur de lOMS pour la recherche en epidemiologie et la reponse aux maladies emergentes. December 6th., 2002). Knowledge of sandflies has been less frequently investigated and the few data reported are highly variable (<25% to 98%) (5,6,8); and, crucially, past studies have tended to detect very variable (<10% to 60%), but generally poor, knowledge of sandflies role in transmission (2,3,5,6,8,9,11, Chappuis et al., 2002).
While no previous study appears to have addressed the extent to which sandfly control activities are affected by knowledge of their role in cutaneous leishmaniasis transmission, there has been at least one study addressing the impact of household income on control practices (12). This study found that in a cutaneous leishmaniasis endemic area of Brazil, control measures which demanded an expenditure were more frequently practiced by households with higher incomes. In addition, in cutaneous leishmaniasis endemic communities in Afghanistan, 78% of households interviewed apparently did not use bednets because bednets were too expensive (2). Both studies therefore provide evidence that without government support, protection against cutaneous leishmaniasis by vector control activities is likely to be inequitably distributed.
The present study describes the sandfly control activities by households in a cutaneous leishmaniasis endemic region of Colombia where sandfly indoor biting is important, and addresses the extent to which household practices are influenced by (1) knowledge of the disease and its transmission, and (2) socioeconomic status. The questionnaire survey was carried out in Huila department, location of a major cutaneous leishmaniasis epidemic from 1993-1996 (cases reported=1,232), with a peak departmental incidence of 275 per 100,000 in 1994. Incidence in this region has risen again in recent years, 57 per 100,000 in 2004 (cases reported=178).
Materials and methods
Study area
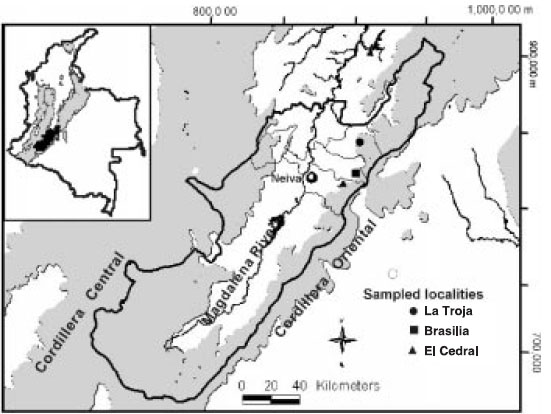
The study was carried out between January to March 2001 in three rural localities on the subandean region of the north-western side of the Cordillera Oriental (mean altitude of 1,660 masl), La Troja (Baraya municipality), Brasilia (Tello municipality), and El Cedral (Neiva municipality), within the cutaneous leishmaniasis epidemic area of Huila department (figure 1). Mean rainfall is 1,311 mm, with an increasing gradient from north to south, and mean temperature is 18.5o C. Rainfall follows a bimodal pattern with two dry, or low rainy, seasons (January-February and July-September) and two rainy seasons (March-May and October-November). The economy of the area is based on agricultural products, mainly coffee crops and pasture. The natural vegetation has been highly disturbed and only a few remnants of the subandean forest have survived. Most of the human population is formed by mestizos peasants.
Questionnaire design and application
Evaluation of the knowledge and practice of human populations in relation to cutaneous leishmaniasis and vector control of sandflies was carried out in a section of a questionnaire answered by the heads of households in 237 houses, during a house risk factor study. Only households who had lived for at least one year in the surveyed houses were included in the study. The vocabulary used in the questionnaire was chosen based on the experience gained in a previous study (Nicholls S, Castaño L, Palau T, Álvarez C, Ayala M, Corredor S et al., 1998. Conocimientos, actitudes y prácticas sobre la leishmaniasis tegumentaria en tres zonas endémicas de Colombia. Informe: Convenio COLCIENCIAS e Instituto Nacional de Salud R.C. 020-93) and by a pilot test of the questionnaire. The topics included in the questionnaire were: demography (number of persons per house by age and gender); knowledge of cutaneous leishmaniasis and sandflies, role of sandflies in transmission, type of control measures (for both disease and sandflies); and building features and the ownership of domestic animal which were used as an indirect measure of economic status. The study was approved by the ethics committee of the Instituto Nacional de Salud.
Control measures
Information on the different control measures (mainly bednets, house spraying with insecticides, house spraying with non-insecticides, and smoke) included: date of start and frequency of use (i.e. all the time, only during the sandfly season [as specified by the interviewee] or other, as specified). Information on product name (for house spraying with insecticides or with non-insecticides), type of material used as fuel (for smoke), and mesh size (for bednets) was also recorded. Additional information about cost of the control measures was obtained from the main market in Neiva city (for bednets) and small shops in Tello municipality (for insecticides).To distinguish control measures for disease and control measures against sandflies (i.e. amongst householders who did not recognize the role of the sandflies in disease transmission) the same questions concerning control practices for cutaneous leishmaniasis were repeated later during the questionnaire, this time referring to sandfly control (i.e. household measures to protect themselves from sandfly nuisance). Only control measures applied by the inhabitants in the current house were recorded.
"Integral understanding" of cutaneous leishmaniasis
The level of "integral understanding" of cutaneous leishmaniasis and its control by householders was evaluated qualitatively based on the presence/absence of knowledge on cutaneous leishmaniasis, sandflies, sandfly role in disease transmission, and the practice of control for cutaneous leishmaniasis. Practices of control for sandflies were not included in this analysis to allow comparison with previous studies, as the majority of these studies had only addressed disease control. Householders were classified in six categories of "integral understanding": (a) very good: householders knew the disease, the sandfly, the role of the sandflies in the transmission, and practised some measure of control for cutaneous leishmaniasis; (b) good: householders knew the disease and some measure of control for cutaneous leishmaniasis; but may or may not recognize sandflies; (c) acceptable: householders knew the disease, the sandfly, and the role of the sandflies in the transmission of the disease; (d) bad: householders knew the disease and sandflies, but were unaware of any association between them; (e) poor: householders knew about the sandflies only; although, some also recognized the role of sandflies in transmission of the disease; (f) none: no knowledge of cutaneous leishmaniasis or sandflies. Results are presented as percentages with each category of integral understanding.
Economic status and control measures
The association between economic status and the use of control measures was based on the comparison of frequencies of practice of the four main control measures (i.e. bednets, house spraying with insecticides, house spraying with noninsecticides, and smoke) with an "index of economic status". The index was generated on the basis of building features and the ownership of domestic animals, both of which should reflect the economic status of the householders. Building features chosen as indicators of a "better" economic status were: walls made of bricks, few or no cracks in walls (0-30%), presence of a ceiling, few or no openings in the house (0-5.8 m2), and availability of electricity service; while the indicators of "low" economic status were: walls made of bahareque or other material, many cracks in walls (>30%), absence of a ceiling, many openings in the house (>5.8 m2), and no electricity service. Ownership of pigs, cows, and equines was considered as an indicator of "better" economic status. The index was obtained by summing the values for all eight features considered as indicators of "better" economic status (where 1=presence, 0=absence). Hence, the index could range between 0, the lowest status, and 8, the highest.
Sandfly sampling
In addition to the questionnaire survey, each house was sampled once with a CDC light trap set up in an inhabited bedroom (13), during the night (18:00 to =7:00 h) in order to provide a crude estimate of relative indoor sandfly abundance, for comparison with the reported household practice of sandfly control. Inhabitants were requested not to apply any control measures during the sampling night. Collected sandflies were identified using the keys of Young (14) and Young and Duncan (15).
Statistical analysis
Information collected by the questionnaire was digitalized in Epi-Info 6.04d (Centers for Diseases Control and Prevention, Atlanta, Georgia, USA) and validated by dual entry. Analysis of the relationship between knowledge and the practice of control was carried out in relation to both cutaneous leishmaniasis control and sandfly control. The description of control measures, as well as their relation with economic status, was carried out only in relation to the practice of sandfly control. This was because the practice of sandfly control was dominant, 82%, as compared with the practice of cutaneous leishmaniasis control, 35%, and because the measures reported to control cutaneous leishmaniasis were, in general, also reported for control of sandflies. Frequencies (e.g. knowledge of the disease, sandflies, and the practice of control measures) were compared using the c2 test with Yates correction, and Fishers exact test, as appropriate.
Comparison of control measures in relation to the index of economic status was carried out by dividing households into two groups: "low" economic status (those with an index 0–3) and "high" economic status (those with an index: 4–8). Where households practised more than one control measure, they were only included in the analyses of associations with the more costly measure. The order of cost was bednets, house spraying, smoke and/or spraying with non-insecticidal substances. The analyses of the least two costly control measures was carried out twice, by varying their perceived order with respect to cost. Univariate analysis of variance was carried out with Stata 7.0 (Stata Corporation. Texas, USA) to test whether indoor sandfly abundance of the most probable vector, Lutzomyia longiflocosa (log transformed data of females/CDC light trap/night) was associated with the practise of any kind of control measure.
Results
Characteristics of the study population
A total of 85% (249/293) of interviewed householders (from 271 houses) were included in the study, as they had lived in their house for at least 1 year. Four additional householders were excluded because the families were absent during the survey. In a few houses (12/235) included in the study more than one (two or three) householders were interviewed. The overall village population was 1,244 inhabitants. Although male: female ratio was 1.25, interviewees were typically female (58.2%) and between 18-60 years old (84.7%).
Knowledge of cutaneous leishmaniasis, sandflies and their role as vectors
85.9% (214/249), of the interviewees knew cutaneous leishmaniasis, known locally as leishmaniasis, with no significant association with gender or age (c2< 0.01, p=0.97 and c2=0.01, p=0.94, respectively); and 98.0% (244/249) knew sandflies, known locally as "mantablanca" or "capotillo". When asked which disease is caused by "mantablanca", the answers by the 244 who responded were: "do not know": 45.5% (111); cutaneous leishmaniasis: 29.5% (72), including those who responded cutaneous leishmaniasis plus another disease; no disease: 15.6% (38); biting signs: 6.6% (16), i.e. weal, ampulla, itch, fever, and allergies; other diseases: 2.8% (7). Amongst interviewees who knew both sandflies and disease, only 31.6% (67/212) knew that sandflies transmit cutaneous leishmaniasis (figure 2), and this included a group of householders, 16.4% (11/67), who said they knew that sandflies transmitted cutaneous leishmaniasis but did not believe it. This scepticism was based on their own experience, e.g. saying: "Mantablanca do not transmit cutaneous leishmaniasis because we have been bitten by a lot of them and we have not got cutaneous leishmaniasis".

Practice of control of cutaneous leishmaniasis and sandflies: impact of knowledge
Only 35.4% (75/212) of interviewees who knew cutaneous leishmaniasis practised any measures with the purpose of controlling the disease. This practice was significantly associated with knowledge of the role of sandflies in transmission (c2 = 16.9, p<0.001), with 50.7% (37/73) of "disease control practitioners" having this knowledge, compared to only 21.9% (30/137) amongst nonpractitioners. In general, using our defined categories (table 1), only 15% of householders had a "very good" understanding of cutaneous leishmaniasis, compared to 56.3% with a "bad" or "poor" understanding of cutaneous leishmaniasis. Nevertheless, an understanding of cutaneous leishmaniasis was clearly not required to carry out sandfly control, as 77.1% of householders with a "bad" understanding of cutaneous leishmaniasis practised some measures to control sandflies. Indeed, 82% (200/244) of interviewees who knew sandflies practiced some control measures against them. There was some suggestion (though not significant: c2=2.68, p=0.102) that this practice was associated with knowledge of the role of sandflies in cutaneous leishmaniasis transmission, with 32% (64/200) of "sandfly control practitioners" having this knowledge, compared to only 18.2% (8/44) amongst non-practitioners. However, sandfly control was certainly associated with the extent of sandfly biting nuisance, as sandfly abundance was significantly higher ( F(6, 235) =2.75, p=0.013) in houses where sandfly control was practiced, Geometric Mean (GM) = 6.7 f/LT/n (females/ CDC light trap/night), than in houses where no control was practiced (2.4 f/LT/n).
Choice of sandfly control measure: impact of socioeconomic status
Amongst those who practiced sandfly control, four measures predominated: (1) smoke, 62% (124/200); (2) bednets, 36.5% (73/200); (3) house spraying with insecticide, 33.0% (66/200); and (4) house spraying with non-insecticidal substances, 23.0% (46/200). Other control measures, such as use of repellents, mosquito coils, vaporizing mats, closing of windows and doors in the evening, vapours of aromatic plants, and burning rubbish outside houses, accounted for 8.9% (17/200).
Smoke was produced from a small fire, made from different materials (e.g. Citrus spp., Pinus spp., Eucalyptus spp., manure from cow or horse, and coffee pods or ground), placed in the bedrooms for approximately five minutes. Householders reported that this method of control repels sandflies for approximately two hours. This measure had the longest history of use, with a median of 18.2 years. A total of 129 bednets were recorded, of which 57% (74/129) had a small mesh size (<1 mm) appropriate as a physical barrier for sandflies. There was a mean number of 0.41 (95% CI: 0.33 - 0.50) bednets/person/house, and an estimated 63% (258/409) of people who lived in houses with bednets slept under a net (assuming that bednets are used by an average of 2 persons). The median time of use was 3.7 years. The most common insecticides used for house spraying were domestic insecticides, 93.9% (62/ 66), with only 10.6% (7/66) of householders reporting the use of agricultural insecticides. This measure had been used for a median time of 6.2 years. The main non-insecticidal substances used for spraying houses were petroleum derivates (e.g. gasoline, kerosene, and other fuels): 95% (42/46). This measure has been practised for a median time of 7.2 years. Householders reported that these substances are used as repellents for sandflies because of their strong smell.
An overwhelming majority of householders said they used the control measures only during the "season of sandfly abundance": smoke, 91.1% (113/124); house spraying with insecticide, 86.2% (56/65); house spraying with non-insecticidal substances, 90.7% (39/43); and bednets, 76.4% (55/ 72) (table 2). This season was identified as either or both of the two dry seasons by 84.3% (145/ 172) of interviewees.
Bednets and house spraying with insecticides were considered high cost measures, whereas house spraying with non-insecticidal substances and smoke were low cost. The cost in the main market in Neiva city, where many people from the study area shop, of a small mesh size bednet is US$ 4.3. The cost of house spraying with domestic insecticides, based on information collected from Tello municipality, ranges from $1.0 to $1.3 per bottle (230 cm3); and householders who use insecticides could spend up to $18/year specifically for sandfly control. The cost of non-insecticidal substances was considered low because these were bought mainly for other uses (fuels for cooking and engines) rather than sandfly control. Smoke was considered as a measure of minimal cost because the fuels were obtained for free around the houses.
Householders using the relatively high cost measures tended to have the highest economic status index
(table 3): the use of bednets (mean index= 4.2) and house spraying with insecticides (3.8), as compared with households using lower cost measures: smoke (3.6) and house spraying with non-insecticidal substances (3.1). The association between socioeconomic status and the practice of using bednets was confirmed by a comparison of bednet usage amongst the two broad categories of economic status, with householders of "high" economic status significantly more likely to use bednets, 44.8% (43/96), than householders of "low" economic status, 23.9% (16/67) (c2=6.59, p=0.01). In contrast, no significant association was detected between economic status and the use of either house spraying with insecticides (p=0.089), smoke ( p=0.83) or house spraying with non-insecticidal substances (p=0.57).
Finally, it is notable that the highest sandfly abundance was detected in the houses of the poorer householders who practised low cost control measures (table 3): house spraying with non-insecticidal substances, 20 (7.6–49) f/LT/n, and smoke, 8.2 (5.4–12) f/LT/n. In contrast, the lowest sandfly abundance, 2.4 (1.3-3.9) f/LT/n, occurred in the houses of those householders who did not use control measures and who had a relatively high economic status (4.1).
Discussion
A remarkable 82% of all householders claimed to have used some sandfly control measure. The positive association detected between sandfly abundance and the practice of control measures does not imply that these control measures are necessarily ineffective. Instead it indicates that control activities are largely practiced in response to sandfly nuisance. This also explains why the majority of householders claim to only practice control measures during the seasons of high sandfly abundance, i.e. the dry seasons. It is notable that in the only other survey of sandfly (rather than disease) control measures used by cutaneous leishmaniasis endemic populations in Latin America (in southern Bahia state, Brazil), this practice was apparently much less common (43%) (12).This could be due to many factors, not least differences in indoor sandfly biting rates. Indoor sandfly biting rates in Huila do appear to be relatively high, with a reported indoor geometric mean during the dry season of 2.8 sandflies/LT/n in Neiva municipality and 6.6 sandflies/LT/n in Baraya municipality (Pardo R, Ferro C, Lozano G, Lozano CA, Cabrera O, Davies C. Flebótomos (Diptera: Psychodidae) vectores de leishmaniasis cutánea y sus determinantes ecológicos en la zona cafetera del departamento del Huila. Memorias, XXVI Congreso de la Sociedad Colombiana de Entomología, Bogotá; 1999. p.147-63).
Almost all sandflies collected indoors are L. longiflocosa, and nearly all bloodfeds collected indoors were shown to have fed on human blood. This would also explain why all but 5 interviewees in this survey knew sandflies, consistent with the results of the previous survey in the region (>80%: Nicholls et al., 1998). In areas where human exposure to sandflies is low, one would expect a poorer sandfly knowledge. For example, amongst a cutaneous leishmaniasis endemic population living in the coffee plantations of Minas Gerais state, Brazil, where the sandfly abundance was apparently low, only 23.1% of the interviewees knew sandflies (16).
In contrast, while 86% of householders in the Huila survey recognized cutaneous leishmaniasis, relatively few (35%) householders in the Huila survey reported that they practiced control measures against cutaneous leishmaniasis. Relatively low levels of cutaneous leishmaniasis control activity was also detected by Nicholls and co-workers (1998) in cutaneous leishmaniasis endemic populations in two other subandean endemic localities: Norte de Santander (17.9%) and Cundinamarca (18.9%). The practice of cutaneous leishmaniasis control in Huila was significantly more frequent amongst householders who knew the role of sandflies in transmission (51%), implying that knowledge of this role could provide householders with a rationale for practicing disease control by targeting sandflies.
Further evidence for this association is provided by the previous surveys in three sub-Andean departments by Nicholls et al. in which the most frequent practise of cutaneous leishmaniasis control was detected in Huila (48%), where interviewees also had the highest knowledge of the role of sandflies in cutaneous leishmaniasis transmission (70%), as compared with populations in Norte de Santander and Cundinamarca, where <20% of householders had knowledge of the role, and a similar small percentage practised cutaneous leishmaniasis control.
However, high levels of knowledge of the role do not guarantee high levels of control activity as is evident in previous studies for leishmaniasis where high percentages (60%->75%) of knowledge of the role corresponded with poor knowledge of cutaneous leishmaniasis control (0–22%) (5, 7, Chappuis and Cavailler, 2002). Indeed, high knowledge of vector biology and control often fails to correspond to the practice of effective vector control for a range of vector borne diseases, such as dengue (17). For leishmaniasis, this discrepancy could depend on the extent to which sandflies are endophagic. Measures of control by householders are applied mainly indoors; for exophagic sandflies, the knowledge of the sandfly role in transmission is not expected to have a significant effect on the practice of cutaneous leishmaniasis control.
In addition to knowledge, the survey found evidence that household economic status also limits the practice of some control measures. The poorest households were more likely to practice the less costly control measures, smoke and house spraying with non-insecticidal substances, as compared with the more costly measures, bednets and house spraying; and bednets, in particular, were significantly more utilised by households in the "high" (45%) rather than "low" (24%) economic status group. A similar finding was indicated in a cutaneous leishmaniasis endemic population in Bahia state, Brazil (12), where families with lower incomes were apparently less likely to practise control measures which demand a high expenditure (2.1%), as compared with households with higher incomes (15.4%).
Note that those households in the Huila study who practiced no control measures were not limited by their economic status (which was relatively high). Instead, it would appear that they had less reason to practice control, as they experienced relatively low sandfly nuisance. Hence, it appears that low cost control measures (smoke or house spraying with non-insecticidal substances) are accessible to all householders in the region, who wish to reduce sandfly nuisance. Smoke was certainly the most commonly used control measure (62%), and had the longest history of use by the householders. Use of smoke as the main control measure (88%) by householders against sandfly vectors of cutaneous leishmaniasis has also been reported in Bahia state, Brazil (12). In Peru too, in some cutaneous leishmaniasis endemic areas households commonly generate smoke indoors during the periods of high density of sandflies as a measure of protection (18). The question remains whether this low cost control activity (or the spraying of non-insecticidal substances) is effective.
In spite of the wide use of repellent and insecticide components extracted (or synthesized) from many plants for commercial purposes, there are limited reports of the effectiveness of traditional formulations (i.e. smoke) on sandflies. In China, indoor smoking with tobacco, pyrethrum or artemisia reportedly kept sandflies away for 1–2 days (19). In Ethiopia, the absence of Phlebotomus longipes in some buildings was attributed, in part, to the smoke indoors (mainly from cooking fires), and their abundance in bedrooms to the absence of smoke (20). A 2-fold reduction in indoor P. martini abundance was also associated with the burning of an indoor fire during the night in a recent risk factor study in Pokot, Uganda (C. Davies & J. Stephenson, unpublished). If such findings can be confirmed by intervention trials, the attractions of this control measure are considerable, i.e. it is easily available, inexpensive and is already widely used. However, it remains unclear whether any health advantages that may ensue from reduced indoor biting insects using smoke outweigh the health disadvantages due to the respiratory effects of indoor pollution.
The potential health advantages of using bednets are less controversial. For example, the use of untreated bednets was identified as a protective factor against visceral leishmaniasis transmitted by P. argentipes in both Nepal and Bangladesh (21, 22). In the present study, the relatively high ownership of untreated bednets by households who practiced any form of control (36.5%, reflecting 0.41 bednets/person/house) indicates that a bednet intervention could have high acceptance by the community. However, 43% of these bednets were wide mesh (>1 mm), which would not provide a complete physical barrier, and so should be treated with insecticide for optimal performance. In a recent lambdacyhalothrin treated bednet (LTN) field trial in this region, LTNs were found to reduce landing rates of L. longiflocosa both inside and outside the bednets, as well as the percentage of bloodfeds, the size of blood meals and the human blood index (HBI) amongst sandflies collected in light traps in houses using LTNs as compared with control houses (Pardo R, Ferro C, Davies C. Efficacy and effectiveness of insecticide treated bednets in Colombia. 5th International Symposium on Phlebotominae sandflies, ISOPS 5, Tunisia, 2005). In the same trial, the impact of insecticide house spraying was less clear.
In conclusion, despite the relatively low "integral understanding" of cutaneous leishmaniasis and its transmission amongst the surveyed population, householders had a good knowledge of some of the different components of the disease and its control. The significant association between the knowledge of sandflies role in transmission and the practice of cutaneous leishmaniasis control provides evidence that there is scope for impacting control activities by health educational campaigns. However, the remarkably high level of sandfly control as compared to cutaneous leishmaniasis control practiced by the community shows how vector control promotion programmes need to account for community attitudes to both sandfly nuisance as well as the diseases they transmit.
Finally, based on the acceptability and its entomological effectiveness, it is possible that the introduction of LTNs could be used to control cutaneous leishmaniasis within the study area. Given the indications that economic status limits the choice of control measure, it may be worth considering bednet subsidies for the lowest economic status households within the context of social marketing campaigns. This could help widen bednet usage and reduce inequities in health status amongst cutaneous leishmaniasis endemic communities.
Acknowledgements
We thank Alcaldías Municipales de Baraya, Tello y Neiva, Secretaría de Salud Municipal de Neiva, hospital local de Baraya, and Centro de Salud de Tello, for logistic support. We thank Gladys Lozano for her support during all stages of the project. She and Álvaro Ruiz and César González provided valuable epidemiological background and they took part in planning field work activities. We thank Stella Pedraza who participated in the field survey and the generation of the data bases. We gratefully acknowledge the field support of the health workers from Tello, Baraya and Neiva municipalities. Finally, we would like to thank the inhabitants of the study localities, particularly La Troja, Brasilia, and El Cedral for their hospitality and kindness with the research team.
Conflicts of interest
The authors declare that they have no competing interests.
Financing
This study received financial support from Instituto Nacional de Salud and Organización Panamericana de la Salud (Contract OPS-ASC-00/00094-0); and from Secretaría de Salud Departamental del Huila (SSDH). Raúl Pardo was supported by a scholarship from Instituto Colombiano para el Desarrollo de la Ciencia y la Tecnología Francisco José de Caldas, COLCIENCIAS.
Correspondencia:
Raul H. Pardo, Laboratorio de Entomología, Instituto Nacional de Salud, Bogotá, D.C., Colombia
Teléfono: (571) 220 0923
raulpardopuentes@yahoo.co.uk
References
1. Davies CR, Reithinger R, Campbell-Lemdrum D, Feliciangeli D, Borges R, Rodriguez N. The epidemiology and control of leishmaniasis in Andean countries. Cad Saude Publica 2000;16:925-50. [ Links ]
2. Reithinger R, Aadil K, Kolaczinsli J, Mohsen M, Hami S. Social impact of leishmaniasis, Afghanistan. Emerg Infec Dis 2005;11:634-6. [ Links ]
3. Moreira RC, Revelo JM, Gama ME, Costa JM. Knowledge level about of American tegumentary leishmaniasis (ATL) and use of alternative therapies in an endemic area in the Amazon region in the state of Maranhao, Brazil. Cad Saude Publica 2002;18:187-95. [ Links ]
4. Weigel MM, Armijos RX. The traditional and conventional medical treatment of cutaneous leishmaniasis in Ecuador. Rev Panam Salud Publica 2001;10:395-404. [ Links ]
5. Arana BA, Rizzo NR, Navin TR, Klein RE, Kroeger A. Cutaneous leishmaniasis in Guatemala: people´s knowledge, concepts and practices. Ann Trop Med Parasitol 2000;94:779-86. [ Links ]
6. Gamea MEA, Barbosa JS, Pires B, Cunha AKB, Frietas AR, Ribeiro IR et al. Evaluation of the level of knowledge about visceral leishmaniasis in endemic areas of Maranhao, Brazil. Cad Saude Publica 1998;14:381-90. [ Links ]
7. Dobles-Ulloa A, Perriard C. Representaciones, actitudes y prácticas respecto a la leishmaniasis cutánea en la población del Cantón de Acosta, provincia de San José, Costa Rica. Estudio antropológico exploratorio. Cad Saude Publica 1994;10:181-9. [ Links ]
8. Weigel MM, Armijos RX, Racines RJ, Zurita C, Izurieta R, Herrera H et al. La leishmaniasis cutánea en la región subtropical del Ecuador: percepciones, conocimientos y tratamientos populares. Bol Ofi Sanit Panam 1994;117:400-13. [ Links ]
9. Isaza DM, Restrepo BN, Arboleda M, Casas E, Hinestroza H, Yurgaqui T. La leishmaniasis: conocimientos y prácticas en poblaciones de la costa del Pacífico de Colombia. Rev Panam Salud Pública 1999;6:177-84. [ Links ]
10. Vásquez ML, Kroeger A, Lipowsky R, Alzate A. Conceptos populares sobre la leishmaniasis cutánea en Colombia y su aplicabilidad en programas de control. Bol Ofi Sanit Panam 1991;110:402-15. [ Links ]
11. Koirala S, Parija SC, Karki P, Das ML. Knowledge, attitudes, and practices about kala-azar and its sandfly vector in rural communities of Nepal. Bull World Health Organ 1998;76:485-90. [ Links ]
12. Santos JB, Lauand L, Sousa GS, Macedo VO. Factores socio-economicos e actitudes en relacion a prevencao domiciliar da leishmaniose tegumentaria americana, em uma area endemica do sul da Bahia, Brasil. Cad Saude Publica 2000;16:701-8. [ Links ]
13. Sudia WD, Chamberlain RW. Battery-operated light trap, an improved model. Mosq News 1962;22:126-9. [ Links ]
14. Young DG. A review of the bloodsucking Psychodid flies of Colombia (Diptera: Phlebotominae and Psycoracinae). Gainesville: Department of Entomology, University of Florida; 1979. p.266. [ Links ]
15. Young DG, Duncan MA. Guide to the identification and geographic distribution of Lutzomyia sand flies in Mexico, The West Indies, Central and South America (Diptera: Psychodidae). Mem Amer Entomol Inst 1994;54:1-881. [ Links ]
16. Alexander B, Oliveira EB, Haigh E, Almeida LL. Transmission of Leishmania in coffee plantations of Minas Gerais, Brazil. Mem Inst Oswaldo Cruz 2002;97:627-30. [ Links ]
17. Degallier N, Vilarinhos PT, de Carvalho MS, Knox MB, Caetano J Jr. Peoples knowledge and practice about dengue, its vectors, and control means in Brasilia (DF), Brazil: its relevance with entomological factors. J Am Mosq Control Assoc 2000;16:114-23. [ Links ]
18. Llanos-Cuentas A. Risk factors associated with the transmission of Andean cutaneous leishmaniasis (thesis). London: London School of Hygiene and Tropical Medicine, London University; 1994. [ Links ]
19. Lu CC, Chung HL, Ling CC, Wu CC, Wang CC, Chiang YT. New Chinas achievements in the treatment and prevention of kala-azar. Chin Med J 1955;73:91-9. [ Links ]
20. Foster WA. Studies on leishmaniasis in Ethiopia. 3: Resting and breeding sites, flight behavior, and seasonal abundance of Phebotomus longipes (Diptera: Psychodidae). Ann Trop Med Parasitol 1972;66:313- 8. [ Links ]
21. Bern C, Hightower AW, Chowdhury R, Ali M, Amann J, Wagatsuma Y et al. Risk factors for Kala-Azar in Bangladesh. Emerg Infec Dis 2005;11:655-62. [ Links ]
22. Bern C, Joshi AB, Jha SN, Das ML, Hightower A, Thakur GD et al. Factors associated with visceral leishmaniasis in Nepal: bed-net use is strongly protective. Am J Trop Med Hyg 2000;63:184-8. [ Links ]

