










Services on Demand
Journal
Article
 English (pdf)
English (pdf)
 Article in xml format
Article in xml format Article references
Article references
 Send this article by e-mail
Send this article by e-mailIndicators
-
 Cited by SciELO
Cited by SciELO -
 Access statistics
Access statistics
Related links
-
 Cited by Google
Cited by Google -
 Similars in
SciELO
Similars in
SciELO -
 Similars in Google
Similars in Google
Share

 Permalink
PermalinkBiomédica
Print version ISSN 0120-4157
Biomédica vol.33 no.3 Bogotá july/Sept. 2013
https://doi.org/10.7705/biomedica.v33i3.832
ARTÍCULO ORIGINAL
doi: http://dx.doi.org/10.7705/biomedica.v33i3.832
1 Departamento de Farmacología y Toxicología, Facultad de Medicina, Universidad de Antioquia, Medellín, Colombia
2 Escuela de Medicina, Universidad de La Frontera, Temuco, Chile
3 Instituto de Efectividad Clínica y Sanitaria (IECS), Buenos Aires, Argentina
4 Escuela de Salud Pública, Facultad de Medicina, Universidad de Buenos Aires, Argentina
Author contributions:
All authors contributed equally to design, analysis and writing of this manuscript
Author contributions:
Jefferson Antonio Buendía, Departamento de Farmacología y Toxicología, Facultad de Medicina, Universidad de Antioquia, Carrera 51D N° 62-83, Medellín, Colombia. Telefax: (574) 219 6022
Recibido: 02/10/12; aceptado:23/04/13
Objective: Trastuzumab (Herceptin®), a recombinant, humanized, monoclonal antibody targeting HER2 is well established as an effective treatment for HER2-positive breast cancer. Evidence from developed countries showed that trastuzumab was cost-effective; but there are few evidences in developing countries. This study assesses the cost-effectiveness of adjuvant trastuzumab treatment in Colombia.
Methods: A Markov health-state transition model was built to estimate clinical and economic outcomes in HER2-positive breast cancer with or without 12 months trastuzumab adjuvant chemotherapy over a lifetime perspective with annual transition cycles. The model incorporated five health states (diseasefree, local recurrence, distant recurrence, cardiac failure, and death). Baseline event rates and 3-year hazard ratio (HR=0.51, IC 95% 0.44–0.59; p<0.0001) were derived from 4-year follow up of the N9831 and NSABP B-31 trial. Costs and utility weights were obtained from the literature and were discounted by 5% annually.
Results: The model showed that the utilization of adjuvant trastuzumab treatment in early breast cancer can prolong 0.80 quality-adjusted life-years (QALY), compared with standard chemotherapy, an incremental cost-effectiveness ratio (ICER) of US$ 71,491 per QALY gained.
Conclusion: The results suggest that 1-year adjuvant Trastuzumab treatment is not cost-effective in Colombia, using the definition of WHO cost-effectiveness threshold of 3 times GDP per capita.
Key words: breast cancer, Human Epidermal Growth Factor Receptor 2–Positive, Colombia
doi: http://dx.doi.org/10.7705/biomedica.v33i3.832
Evaluación económica del trastuzumab como tratamiento adyuvante en cáncer de mama HER2- positivo en Colombia
Introducción. El trastuzumab es un anticuerpo monoclonal de reconocida efectividad para el tratamiento en mujeres con cáncer de mama positivo para HER2. Sin embargo, la mayoría de estudios de costo-efectividad se han llevado a cabo en países desarrollados.
Objetivo. Determinar el costo-efectividad del tratamiento adyuvante con trastuzumab en mujeres con cáncer de mama HER2+ en Colombia.
Materiales y métodos. Se construyó un modelo de Markov, con ciclos de transición anuales y desde la perspectiva del pagador, para estimar los resultados clínicos y económicos derivados de la administración de trastuzumab en mujeres con HER2 positivo. El modelo incorpora cinco estados de transición: libre de enfermedad, recurrencia local, metástasis, falla cardiaca y muerte. La tasa de eventos y la razón de tazas instantáneas (0,51; IC 95% 0,44-0,59; p<0,0001) se derivaron del reporte a cuatro años de los ensayos clínicos controlados N9831 y NSABP B-31. Los costos y las utilidades se estimados a partir de la literatura científica, utilizando una tasa de descuento del 5 % anual.
Resultados. El modelo revela que la utilización de trastuzumab como tratamiento adyuvante prolonga la expectativa de vida ajustada por calidad en 0,8 años, en comparación con la quimioterapia sin trastuzumab; a una razón de costo efectividad incremental (sic.) de US$ 71.491 por año de vida ganado ajustado por calidad de vida.
Conclusión. El tratamiento con trastuzumab durante un año no es costo-efectivo en Colombia, utilizando la definición de costo-efectividad de la OMS de menos de dos a tres veces el PIB per cápita por año de vida ganado ajustado por calidad de vida.
Palabras clave: evaluación de costo-efectividad, neoplasias de la mama, factor de crecimiento epidérmico, Colombia
doi: http://dx.doi.org/10.7705/biomedica.v33i3.832
Introduction
Breast cancer is the first leading cause of cancer death in women in Colombia .The adjusted mortality rate of breast cancer was 9.5 per 100,000 females and there was an uptrend either in the morbidity and mortality during the last years. Breast cancer has become in the most common cancers for women in Colombia, and other developing countries.
Trastuzumab (Herceptin®), a recombinant, humanized, monoclonal antibody targeting HER2 is well established as an effective treatment for HER2-positive breast cancer. It was notable that trastuzumab significantly reduced the risks of cancer local recurrence and metastasis and can prolong survival. Though the cost of trastuzumab treatment is high; and this drug has been recommended as adjuvant treatment for HER2-positive breast cancer. Evidence from other countries showed that trastuzumab was cost-effective in adjuvant treatment for early breast cancer; but there are few evidence of cost-effectiveness analyses in developing countries based on the 4-year followup data of the North Central Cancer Treatment Group (NCCTG) N9831 and the National Surgical Adjuvant Breast and Bowel Project (NSABP) and HERA trial where the magnitudes of improvement in disease-free survival were decreased and cost effectiveness of adjuvant trastuzumab remains uncertain.
This drug has a relative high treatment cost respect to others current drugs in breast cancer and there are concerns whether trastuzumab have an adequate equilibrium between cost and it´s benefits especially in developing counties where cost-effectiveness and outcomes evidence tend to be vital for policymakers to make a tradeoff between limited financial resources and equitable access. Therefore, this cost-effectiveness analysis is designed to increase the economic evidence, of adjuvant trastuzumab therapy, to support decisionmaking from the perspective of health-care payers.
Patients and methods
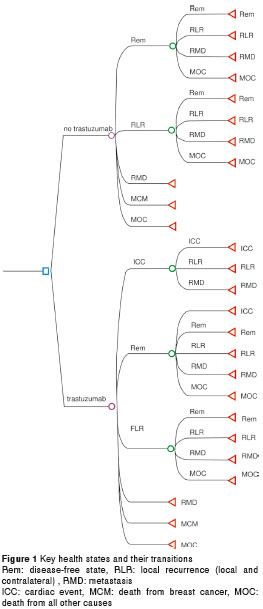
A Markov model chain, programmed in a TreeAge Pro 2009®, was developed to estimate the costs and outcomes of 12 months of adjuvant trastuzumab after chemotherapy for HER2-positive breast cancer, compared to standard chemotherapy in a hypothetical cohort of typical'' patient enrolled in the NCCTG and NSABP trials a 50-year-old woman. Patients were eligible if they had invasive breast cancer resected by lumpectomy or mastectomy and axillary dissection with pathologically involved axillary nodes (amended in NCCTG N9831 to allow patients with high-risk, node-negative disease). The tumor had to be HER2-positive (immunohistochemistry score of 3+ or fluorescence in situ hybridization [FISH]-positive) and had to be verified centrally [NCCTG N9831] or by an approved laboratory [NSABP B-31]). Patients had to have normal hematologic, hepatic, and renal function, and normal left ventricular ejection fraction, as assessed by multigated acquisition scan or echocardiogram. Patients were excluded when they had locally advanced or distant disease, had received prior anthracycline or taxane therapy, had significant sensory or motor neuropathy,or had past or active cardiac disease. Clinical data and the treatment protocol were based on the results of the NCCTG N9831 and NSABP B-31 and HERA trial. Five health states were defined in the progression of breast cancer: disease-free state (DFS), local recurrence (local and contralateral), metastasis, cardiac event, and death (see Fig. 1). The analysis was run from a lifetime perspective. The cycle length was 1 year. Costs and QALYs were both discounted in the base case analysis by 5% annually. All assumptions used in the model are outlined in table 1.
Clinical data
According to the 4-year follow up of N9831 and NSABP B-31 trials assessed the efficacy and safety of adding 52 weeks of trastuzumab to standard anthracycline/taxane-based chemotherapy (doxorubicin plus cyclophosphamide followed by paclitaxel). The adjusted hazard ratio for recurrence in the trastuzumab group, compared with the observation group, was 0.51; (95% confidence interval: 0.44–0.59; p<0 · 0001). The loading dose of Trastuzumab in the model was 4 mg per kilogram weight and 2 mg per kilogram weekly. The specific transition probabilities of disease progression were retrieved from the literature (see table 2). The clinical benefit of trastuzumab was assumed to last for the first 5 years . Thereafter, the risk for recurrent and metastatic disease in the trastuzumab group was assumed to be the same as in the observation group. The utilities associated with different health states were derived from published literature (see table 3). The baseline rate and the relative risk of cardiac toxicity with adjuvant trastuzumab were derived from the incidence of symptomatic congestive heart failure from the literature.
Costs
The analysis perspective was that of health-care payers, and we calculated only the direct medical costs (see table 4). Neither indirect costs (example: work loss) nor direct non-medical costs (example: transportation) were considered. Management costs for local and distant cancer recurrences (hormonal therapy, chemotherapy, radiotherapy, supportive care), costs of managing cardiotoxicity and costs of Trastuzumab in the adjuvant settingincluding HER2/neu screening, acquisition costs, drug administration, supportive medications, and patient management - were taken from earlier cost studies, adjusted for current inflation in Colombia (2010), and National Health Reference Price List (SOAT 2010).The cost impact of longer or shorter palliative Trastuzumab therapy was tested in a oneway sensitivity analysis. All costs were adjusted to 2010 US dollars (Currency rate: US$ 1.00 = COP$ 2,000).The primary result is indicated as the incremental cost per incremental quality adjusted life-year-gained (QALYs).
Sensitivity Analysis
We conducted sensitivity analyses with Monte-Carlo simulation method to understand the key drivers and general sensitivity of the model. We used this kind of analysis because it let us vary simultaneously, across 10,000 simulations, different variables of model according to specific probability distributions. The following variables were assessed: utility values, discounting rate, transition probabilities, total cost by health state; hazard ratio, drug price and, efficacy period of trastuzumab. Because the model is a synthesis of a number of data sources, the short-term overall survival estimates were compared with overall survival results reported by the clinical trials to assess the internal validity of the model. The discount-rate range for sensitivity was 0-10%. Because none of the cost studies reported the variance of their mean cost estimates, the probabilistic modeling assumed a log normal distribution with a standard deviation of 0.25 for all cost parameters.
Results
The mean of life years was 9.35 years with trastuzumab and 8.53 years without trastuzumab, an increment of 0.82 years. Incremental QALY of 0.80 years was generated with trastuzumab treatment (see table 5).

The discounted lifetime medical expenditure (discount rate of 5%) was US$ 132,361 per patient treated with trastuzumab and US$ 75,315 without trastuzumab treatment. This result in an incremental cost-effectiveness ratio (ICER) for trastuzumab treatment of US$ 71,491 per QALY gained.
Sensitivity analysis
One-way sensitivity analyses of parameters in the model showed that cost-effectiveness of trastuzumab was sensitive to the discount rate - ICER with discount rate of 0% of US$ 39,724 and US$ 115,132 with discount rate of 10%-; and duration of clinical benefit - ICER with 10 years of duration of clinical benefit of US$ 46,397.
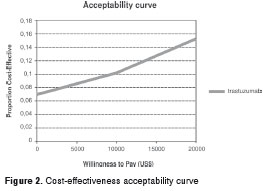
Other one-way sensitivity analyses for total cost by health state, utility by health state and transition probabilities, price and HR of trastuzumab, showed little change. The acceptability curve is shown in Figure 2. The probability that the ICER of 1-year Trastuzumab was less than US$ 15,000 was 12.4%. (Using the WHO cost-effectiveness threshold of 3 times GDP per capita: US$ 15,000 in Colombia, 2010.
To test external validity, the model results for no Trastuzumab were compared with survival at 3 years in control arms of N9831 and NSABP B-31 and HERA trial. N9831 and NSABP B-31 and HERA trial reported survival of 92% and 91% respectively and our model predicted survival of 88%.
Discussion
The 1-year adjuvant trastuzumab treatment is not cost effective in Colombia. Since Colombia does not have a threshold that represents the willingness to pay (WTP) per unit of effectiveness (LYG or QALY), the ICER results per QALY were evaluated by using the reference corresponds to the World Health Organization (WHO) recommendation (three times the GDP per capita). The uncertainty of threshold levels in developing countries such as Colombia creates some controversies and 3 times the GDP per capita per QALY gained might differ from the real willingness to pay by decision makers to Colombia. Some authors recommends that the threshold for WTP should be treated as a range of cost and the probability of rejection should be determined based on the estimated acceptance curve. In our study trastuzumab treatment had only a 12.4% likelihood of meeting a $15,000 per QALY threshold in Colombia. Our model yielded similar results to other analyses in Colombia. Castillo using a Markov model with nine key health states in 2008, from the perspective of the Colombian National Cancer Institute (direct payer), found that adjuvant trastuzumab is not cost-effective based on the interim clinical data from N9831 and NSABP B-31, with an ICER per LYG (US$ 30,574). As well, our findings are similar to recent study of CE of Trastuzumab in seven countries in Latin-America, using four health states in 2011 from health care sector perspective, where incremental CE ratios ranged from US$ 42,104 to $ 110,283 per QALY with a 0% of probability that trastuzumab was CE if willingness-to-pay threshold is three GDP per capita.
Increasing medical costs are becoming a major issue in developing countries. The acquisition cost of trastuzumab, like many newer oncology drugs, is relatively high respect to other breast cancer drugs and this is particularly evident in developing countries with highest drug prices relative to their mean per capita income; increasing the gap between the cost of new and current therapies increasing probability of payment rejection based in QALY threshold. This drug have been included in National Essential Medicine List and national guidelines of breast cancer despite of previously and recent evidence of not cost effectiveness of this drug not only in Colombia and other countries of Latin-America using a WHO recommendation of willingness to pay (WTP) per unit of effectiveness (LYG or QALY), of three times the GDP per capita.
In our analyses, CE was particularly sensitive to the duration of carryover benefit for trastuzumab beyond the 5-year efficacy results reported by the updated trials. The CE for adjuvant trastuzumab, was US$ 60,246 and US$ 43,397 per QALY gained for the 6- and 10-year benefit scenarios, respectively. Skedgel applied efficacy estimates from the updated HERA study found a ICER of CDN$ 72,292 per QALY gained based on 5-year duration of benefit, and CDN$ 127,862 per QALY with 3-year duration of benefit over a 25-year analysis horizon. Also, a recent updated cost-effectiveness analysis from the UK perspective, found that the costeffectiveness of trastuzumab was highly sensitive to the estimated duration of treatment benefit assuming the hazard ratio for disease-free survival was 0.63. The difference in results between the 5- and 10-year benefit scenarios in our analysis, and before papers highlights the need for longer followup in clinical trials to define the true duration of adjuvant trastuzumab benefit. An especial attention must be placed on discount rate; in our study CE was particularly sensitive to discount rate .Since explicit stamens for Latin American countries were not available, we used parameters used and recommended by international literature . In this sense, in our analysis using a higher discount rate (10%) or lower discount rate (0%) could not change our results and trastuzumab is considered non-cost-effective using the threshold corresponds to the WHO recommendation (three times the GDP per capita).
There were several limitations to our analysis. First, we used UK utilities because in Colombia there are no health-related quality of life data for breast cancer patients. Nevertheless, one-way sensitivity analyses for utilities associated with different health states showed little change. Second, our analysis was based on estimates of efficacy under controlled conditions rather than effectiveness in actual clinical practice. It is likely that the observed clinical benefit of adjuvant trastuzumab in routine clinical practice will be less favorable than that observed in clinical trials. We took a direct payer rather than a societal cost perspective that would include costs such as lost productivity and caregiver time. Cardiac event was modeled as one of the five mutually exclusive health states similar to other studies. We assumed that medical treatment for cardiac events was carried out for 1 year, as trastuzumab cardiotoxicity is usually reversible. To date, in all available studies with adjuvant T treatment, no death due to heart failure occurred; hence, mortality due to side-effects was assumed to be zero. In conclusion 1-year adjuvant trastuzumab treatment is not cost-effective in Colombia, using the definition of WHO costeffectiveness threshold of 3 times GDP per capita.
None
No funding was received
1. Pardo C, Cendales R. Incidencia estimada y mortalidad por cáncer en Colombia, 2002-2006. Bogotá, D.C.: Instituto Nacional de Cancerología; 2010. [ Links ]
2. Robles S, Galanis H. El cáncer de mama en América y el Caribe. Rev Panam Salud Pública 2002;12:142-3. http://dx.doi.org/10.1590/S1020-49892002000800016 [ Links ]
3. Bosetti C, Malvezzi M, Chatenoud L, Negri E, Levi F, La Vecchia C. Trends in cancer mortality in the Americas, 1970-2000. Ann Oncol. 2005;16:489-511. http://dx.doi.org/10.1093/annonc/mdi086 [ Links ]
4. Hernández G, Cantor LF. Análisis de las tendencias de mortalidad por cáncer de mama en Colombia y Bogotá, 1981-2000. Rev Colomb Cancerol. 2007;32:32-9. [ Links ]
5. Lewis R, Bagnall AM, Forbes C, Shirran E, Duffy S, Kleijnen J, et al . The clinical effectiveness of trastuzumab for breast cancer: A systematic review. Health Technol Assess. 2002;6:1-71. [ Links ]
6. Viani GA, Afonso SL, Stefano EJ, De Fendi LI, Soares FV. Adjuvant trastuzumab in the treatment of her-2- positive early breast cancer: A meta-analysis of published randomized trials. BMC Cancer. 2007;7:153. http://dx.doi.org/10.1186/1471-2407-7-153 [ Links ]
7. McKeage K, Lyseng-Williamson KA. Trastuzumab: A pharmacoeconomic review of its use in early breast cancer. Pharmacoeconomics. 2008;26:699-719. http://dx.doi.org/10.2165/0042310-200824120-00002 [ Links ]
8. Carlson RW , Allred DC , Anderson BO , Burstein HJ, Carter WB, Edge SB, et al . Breast cancer. Clinical practice guidelines in oncology. J Natl Compr Canc Netw. 2009;7:122-92. [ Links ]
9. Kurian AW, Thompson RN, Gaw AF, Arai S, Ortiz R, Garber AM. A cost-effectiveness analysis of adjuvant trastuzumab regimens in early HER2/neu-positive breast cancer. J Clin Oncol. 2007;25:634-41. http://dx.doi.org/10.1200/ JCO.2006.06.3081 [ Links ]
10. Garrison LP, Jr., Lubeck D, Lalla D, Paton V, Dueck A, Pérez EA. Cost-effectiveness analysis of trastuzumab in the adjuvant setting for treatment of HER2-positive breast cancer. Cancer. 2007;110:489-98. http://dx.doi.org/10.1002/cncr.22806 [ Links ]
11. Fagnani F, Colin X, Arveux P, Coudert B, Misset JL. Cost/effectiveness analysis of adjuvant therapy with trastuzumab in patients with HER2 positive early breast cancer. Bull Cancer. 2007;94:711-20. [ Links ]
12. Elkin EB, Weinstein MC, Winer EP, Kuntz KM, Schnitt SJ, Weeks JC. HER-2 testing and trastuzumab therapy for metastatic breast cancer: A cost-effectiveness analysis. J Clin Oncol. 2004;22:854-63. http://dx.doi.org/10.1200/JCO.2004.04.158 [ Links ]
13. Liberato NL, Marchetti M, Barosi G. Cost effectiveness of adjuvant trastuzumab in human epidermal growth factor receptor 2-positive breast cancer. J Clin Oncol. 2007;25:625-33. http://dx.doi.org/10.1200/JCO.2006.06.4220 [ Links ]
14. Lidgren M, Wilking N, Jonsson B, Rehnberg C. Costeffectiveness of HER2 testing and trastuzumab therapy for metastatic breast cancer. Acta Oncol. 2008;47:1018-28. http://dx.doi.org/10.1080/02841860801901618. [ Links ]
15. Macedo A, Andrade S, Cirrincione JR. Custo efectividad de trastuzumab no tratamento de doentes com cancro da mama em estádios iniciais em Portugal. Acta Med Port. 2010;23:475-82. [ Links ]
16. Gianni L, Dafni U, Gelber RD, Azambuja E, Muehlbauer S, Goldhirsch A, et al . Treatment with trastuzumab for 1 year after adjuvant chemotherapy in patients with HER2-positive early breast cancer: A 4-year follow-up of a randomized controlled trial. Lancet Oncol. 2011;12:236-44. http://dx.doi.org/10.1016/S1470-2045(11)70033-X [ Links ]
17. Pérez EA, Romond EH, Suman VJ, Jeong JH, Davidson NE, Geyer CE, Jr., et al . Four-year follow-up of trastuzumab plus adjuvant chemotherapy for operable human epidermal growth factor receptor 2-positive breast cancer: Joint analysis of data from NCCTG N9831 and NSABP B-31. J Clin Oncol. 2011: 29:3366-73. http://dx.doi.org/10.1200/JCO.2011.35.0868. [ Links ]
18. Pichon-Riviere AA, Garay OU, Buendía JA, Rodríguez A, Vallejos C, Huayanay L, et al . CN1 Cost-effectiveness of trastuzumab in the adjuvant treatment of early breast cancer in six Latin American countries. Value Health. 2011;14:a538. http://dx.doi.org/10.1016/j.jval.2011.08.1537 [ Links ]
19. Augustovski F, Iglesias C, Manca A, Drummond M, Rubinstein A, Martí SG. Barriers to generalizability of health economic evaluations in Latin America and the Caribbean region. Pharmacoeconomics. 2009;27:919-29. http://dx.doi.org/10.2165/11313670-000000000-00000. [ Links ]
20. Piccart-Gebhart MJ, Procter M, Leyland-Jones B, Goldhirsch A, Untch M, Smith I, et al . Trastuzumab after adjuvant chemotherapy in HER2-positive breast cancer. N Engl J Med. 2005;353:1659-72. http://dx.doi.org/10.1056/NEJMoa052306 [ Links ]
21. Clarke M, Darby S. Effects of radiotherapy and of differences in the extent of surgery for early breast cancer on local recurrence and 15-year survival: An overview of the randomized trials. Lancet. 2005;366:2087-106. http://dx.doi.org/10.1016/S0140-6736(05)67887-7 [ Links ]
22. Tan-Chiu E, Yothers G, Romond E, Geyer CE, Jr, Ewer M, Keefe D, et al . Assessment of cardiac dysfunction in a randomized trial comparing doxorubicin and cyclophosphamide followed by paclitaxel, with or without trastuzumab as adjuvant therapy in node-positive, human epidermal growth factor receptor-2 overexpressing breast cancer: NSABP B31. J Clin Oncol. 2005;23:7811-9. http://dx.doi.org/10.1200/JCO.2005.02.4091 [ Links ]
23. Tengs TO, Wallace A. One thousand health-related qualityof- life estimates. Med Care. 2000;38:583-637. [ Links ]
24. Chen W, Jiang Z, Shao Z, Sun Q, Shen K. An economic evaluation of adjuvant trastuzumab therapy in HER2-positive early breast cancer. Value Health. 2009;12(Suppl.3):S82-S4. http://dx.doi.org/10.1111/j.1524-4733.2009.00634.x. [ Links ]
25. Sánchez-Castillo JO. Estudio de costo-efectividad del uso de trastuzumab como tratamiento adjuvante del cáncer de mama temprano HER 2 positivo en el Instituto Nacional de Cancerología,desde el punto de vista del pagador (tesis). Bogota, D.C.: Universidad Nacional de Colombia; 2008. [ Links ]
26. Martínez J, Díaz J, Díaz S, Ballesteros M, Perry F, Quintero A. Costos del uso de trastuzumab para cáncer de mama metastásico en el Instituto Nacional de Cancerología. Serie de casos. Rev Colomb Cancerol. 2007;11:189-92. [ Links ]
27. Banco Mundial. PIB per cápita 2012. Fecha de consulta: 23 de marzo del 2013. Disponible en: http://datos.bancomundial.org/indicador/NY.GDP.PCAP.CD [ Links ]
28. WHO. Cost-effectIveness thresholds. Ginebra: WHO; 2013. Fecha de consulta: 23 de marzo del 2013. Disponible en: http://www.who.int/choice/costs/CER_thresholds/en/index.html [ Links ]
29. Shiroiwa T, Sung YK, Fukuda T, Lang HC, Bae SC, Tsutani K. International survey on willingness-to-pay (WTP) for one additional QALY gained: What is the threshold of cost effectiveness? Health Econ. 2010;19:422-37. http://dx.doi.org/10.1002/hec.1481. [ Links ]
30. Romond EH, Pérez EA, Bryant J, Suman VJ, Geyer CE. Jr., Davidson NE, et al . Trastuzumab plus adjuvant chemotherapy for operable HER2-positive breast cancer. N Engl J Med. 2005;353:1673-84. http://dx.doi.org/10.1056/NEJMoa052122 [ Links ]
31. Buendía-Rodríguez JA, López-Gutiérrez JJ, García-Vega OA, Díaz-Rojas J, Sánchez-Villamil JP. Prescripción de medicamentos en pacientes atendidos en instituciones de mediano y alto nivel de complejidad. Rev Salud Pública. 2008;10:605-14. http://dx.doi.org/10.1590/S0124-00642008000400010 [ Links ]
32. Rubinstein A, Pichon-Riviere A, Augustovski F. Development and implementation of health technology assessment in Argentina: Two steps forward and one step back. Int J Technol Assess Health Care. 2009;25(Suppl.1):260-9. [ Links ]
33. Minsalud. Guía de atención integral para la detección temprana, tratamiento integral, seguimiento y rehabilitación del cáncer de mama 2012. Fecha de consulta: 23 de marzo 2012. Disponible en: http://www.cancer.gov.co/documentos/Gu%C3%ADas/GAI%20Guia_corta_2_10-09-2012.pdf [ Links ]
34. Skedgel C, Rayson D, Younis T. The cost-utility of sequential adjuvant trastuzumab in women with her2- neu-positive breast cancer: An analysis based on updated results from the hera trial. Value Health. 2009;12:641-8. http://dx.doi.org/10.1111/j.1524-4733.2009.00511.x [ Links ]
35. Hall PS, Hulme C, McCabe C, Oluboyede Y, Round J, Cameron DA. Updated cost-effectiveness analysis of trastuzumab for early breast cancer: A UK perspective considering duration of benefit, long-term toxicity and pattern of recurrence. Pharmacoeconomics. 2011;29:415-32. http://dx.doi.org/10.2165/11588340-000000000-00000 [ Links ]
36. van Vlaenderen I, Canon JL, Cocquyt V, Jerusalem G, Machiels JP, Neven P, et al . Trastuzumab treatment of early stage breast cancer is cost-effective from the perspective of the Belgian health care authorities. Acta Clin Belg. 2009;64:100-12. [ Links ]
37. Neyt M, Huybrechts M, Hulstaert F, Vrijens F, Ramaekers D. Trastuzumab in early stage breast cancer: A costeffectiveness analysis for Belgium. Health Policy. 2008;87:146-59. http://dx.doi.org/10.1016/j.healthpol.2007.11.003. [ Links ]
38. Smith I, Procter M, Gelber RD, Guillaume S, Feyereislova A, Dowsett M, et al . 2-year follow-up of trastuzumab after adjuvant chemotherapy in HER2-positive breast cancer: A randomized controlled trial. Lancet. 2007;369:29-36. http://dx.doi.org/10.1016/S0140-6736(07)60028-2 [ Links ]
39. Ewer MS, Vooletich MT, Durand JB, Woods ML, Davis JR, Valero V, et al . Reversibility of trastuzumab-related cardiotoxicity: New insights based on clinical course and response to medical treatment. J Clin Oncol. 2005;23:7820-6. http://dx.doi.org/10.1200/JCO.2005.13.300 [ Links ]
