











 Spanish (pdf)
Spanish (pdf)
 Article in xml format
Article in xml format Article references
Article references
 Send this article by e-mail
Send this article by e-mail Cited by SciELO
Cited by SciELO  Cited by Google
Cited by Google  Similars in
SciELO
Similars in
SciELO  Similars in Google
Similars in Google 
 Permalink
PermalinkFrom 1984 to 2008, overall cancer mortality rates decreased slightly in both sexes in Colombia 1. Around this same period (1985-2005), substantial demographic changes occurred in the country, including population growth (from 30.8 million to 42.9 million inhabitants) and a rapidly increasing life expectancy: 4.3 years for men and 4.8 years for women 2. Many societal changes also occurred: a large healthcare reform led to greater health insurance coverage, which passed from 59% around year 2000 to 92% in 2012 3, and security levels increased as violent deaths substantially reduced 4.
This combination of population growth and ageing of the population usually leads to a growing cancer burden, even with relatively stable or slightly decreasing cancer mortality rates 1,5. Although age-standardized mortality rates for cancer as a whole decreased slightly, the total annual number of cancer deaths among males increased between 1984 and 1988 and between 2004 and 2008, from 8,791 to 15,417 (175% increase), and among females from 9,624 to 15,847 (165% increase) 1. This apparent discrepancy between stable or even decreasing mortality rates with increasing number of cancer deaths can be explained by to population growth and ageing. Considering only the total number of cancer deaths, irrespective of age and cancer type, overlooks the fact that some cancers have a much heavier burden on society compared to others, because they occur more frequently among younger people.
Years of life lost (YLL) is a useful measure to take the age at death as well as the deaths at each age into account. The measure results from the sum of years of potential life lost by individuals in the population because of death by a certain disease, given their remaining life expectancy estimated by age and sex. The average years of life lost (AYLL) is the average number of years of life lost by each person dying from the disease under study.
Approximately 25-30% of YLL in western countries are attributed to cancers 6. While YLL depend strongly on absolute frequency of deaths, AYLL are mostly determined by the age at which the deaths occur. Together, these measures provide meaningful indicators for decisions regarding resource allocations and design of prevention programs 7-9. They are also a useful base for comparison with other countries, and show the relative importance of different causes of death, taking into account the life expectancies of each population 10. Previous national and local Colombian studies used external life expectancy data from Japan or the Global Burden of Disease reports, considered as the "potential" life expectancy for other countries 11-13). While using a standard "ideal life expectancy" provides a useful comparison with other countries, a major limitation is that it does not reflect the actual situation of years of life lost in a given country.
The purpose of this paper was to quantify YLL and AYLL due to cancer in general and to the most important cancer types in Colombia for the most recent periods with available data (up to 2012), and to evaluate how this burden changed between 1997 and 2012 using the country's life expectancy data.
Materials and methods
Data and corrections to the data
We used Colombia's official mortality data and population denominators retrieved from the Departamento Administrativo Nacional de Estadística, DANE, and we analyzed the following cancer types as listed in the International Classification of Diseases, ICD-10: All cancers (C00-C96), oral cavity and pharynx (C00-C14), oesophagus (C15), stomach (C16), colorectum (C18-C20), pancreas (C25), bronchus and lung (C32-C34), breast (C50), cervix uteri (C53), ovary (C56), prostate (C61), brain and central nervous system (CNS) (C70-C72), leukemia (C91-C95), lymphomas (C81-C85, C96), melanoma (C43), kidney (C64-C65) and bladder and urinary tract cancer (C66-68). We also considered all deaths combined, regardless of the cause of death.
We redistributed deaths without information on age proportionally by sex based on the age distri-bution of the other cases in the same cause of death category during the corresponding period. Similarly, we redistributed deaths from unspecified uterine cancer (C55) according to the proportions of deaths for cervical cancer (C53) and cancer of the corpus uteri (C54) (14).
Analysis
We calculated annual YLL for the general population (all ages) by period and sex summing up the number of cancer deaths in a certain age group with the remaining life expectancy in that age for all age groups according to the method previously explained by Brustugun, et al.6, using the following formula:

To provide an estimate of the YLL due to cancer as a fraction of total YLL, we also calculated a hypothetical total YLL, based on the sum of the products of the total number of deaths per age group, multiplied by the estimated length of life on each age level. We applied this same method for childhood cancers (0- 14 years).
Life expectancy among Colombian population was calculated by age group, sex and time period according to DANE's five-calendar year periods from 1997 to 2005, and from 2005 to 2015 (2). We calculated the number of deaths by cancer type, sex and age groups for the same periods based on the national mortality databases for the 1997-2012 period as provided by DANE (1997-1999; 2000-2004; 2005-2009; 2010-2012).
We calculated the AYLL by dividing the total YLL per cause by the total number of deaths due to this cause, and for each sex and period separately. We determined the changes in YLL and AYLL percentages over time as the percentage increase or decrease between 2010 and 2012 compared to the reference period (1997-1999).
Results
Overall number of cancer deaths
The total annual number of cancer deaths increased for both sexes in about 33%, from 12,292 in 1997-1999 to 16,376 in 2010-2012 in males, and from 12,687 to 17,001 in females. In the first period of the series (1997-1999), cancer comprised 12% of all male and 10% of all female deaths, while in the last period (2010-2012) it accounted for 15% and 20% of male and female deaths, respectively.
Around 3-4% of all deaths occurring in children up to 14 years of age, was due to cancer, and this proportion was stable over time. The total number of cancer deaths in children (0 to 14 years) was 1,749 in the period 1997-1999, which decreased to 1,510 in 2010-2012.
Overall years of life lost and average years of life lost
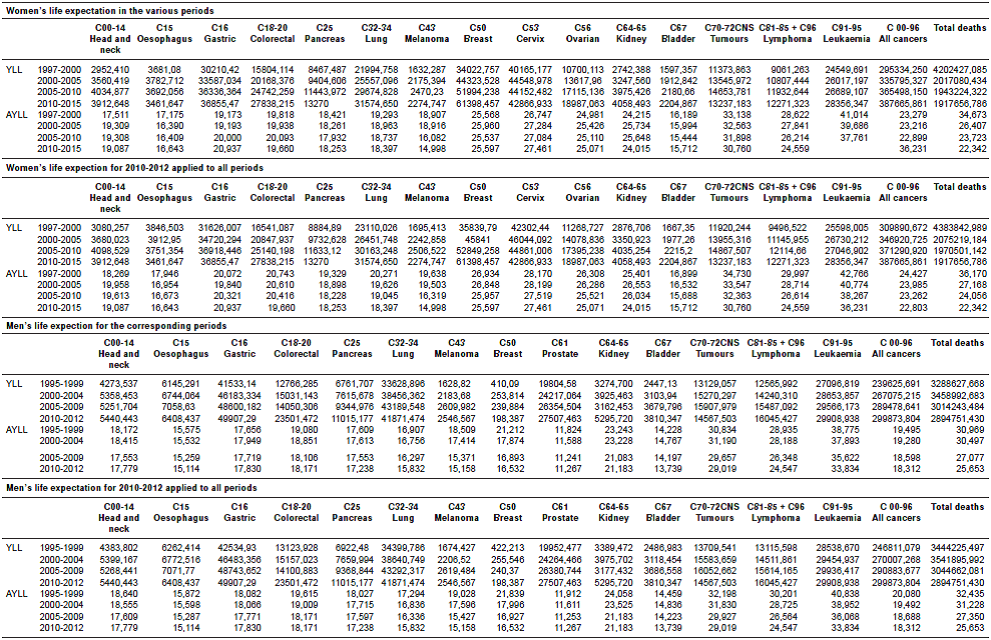
In 1997-1999, a hypothetical 534,960 (239,626 males; 295,334 females) years of life were lost due to cancer annually, and this figure increased to 687,540 (299,874 males; 387,666 females) in 2010-2012 representing an overall increase of 28.5%: 25.1% in males and 31.1% in females. In the same period, the Colombian population grew by 24,8% (from 38.6 million in 1997 to 48.2 million in 2012) (2).
Years of life lost and average years of life lost by cancer types
Whereas YLL for any cause of death decreased markedly between 1997 and 2012 (-12% for males, and -54% for females), in this same period they increased for cancer, with 25% in males and 31% in females. For the 2010-2012 period the three most common cancer causes of YLL in men were stomach cancer (49,907), lung cancer (41,871), and leukemia (29,908), while in women they were breast cancer (61,398), cervical cancer (40,165), and stomach cancer (30,210) (figure 1). In this same period, one cancer death in Colombia represented on average 25.7 years of life lost for men and 22.8 for women, though these estimates vary significantly between cancer types.
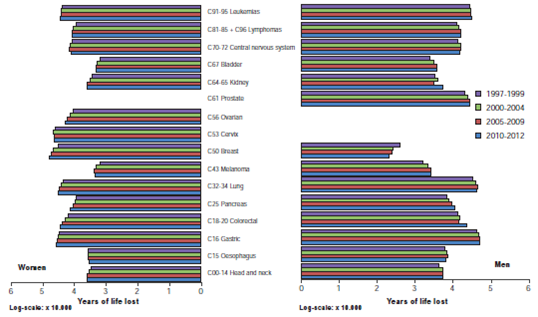
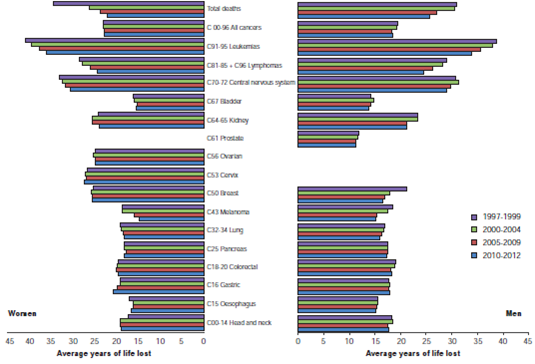
Virtually, all cancer types showed AYLL of 15 or more years, with the exception of prostate and bladder cancer in males. The highest AYLL in both sexes corresponded to cancers occurring predominantly at young ages: Leukemia (males: 33.8, females: 36.2), cancers of the brain and central nervous system (males: 29.0, females: 30.8) and lymphomas (2010-2012: males 24.5, females 24.6) (figure 2).
We observed the highest increase in YLL for both sexes in colorectal, pancreas and kidney cancers, all by more than 40%. For males, the most substantial increases corresponded to pancreas, melanoma and bladder cancer, while in females, breast, ovarian and colorectal cancers had the largest increases (table 1).
Table 1 Change in years of life lost (YLL) and average years of life lost (AYLL) between 1997 and 2012 by cancer type and sex
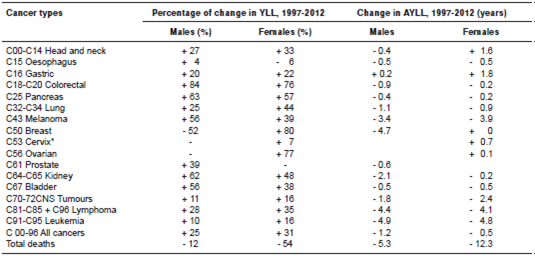
AYLL trends remained fairly stable, except for very rare cancers such as male breast cancer; the few changes observed were generally towards lower AYLL. The largest reductions in AYLL were observed for cancers of the brain and central nervous system, melanomas, lymphomas and leukemia, where two or more years of life expectancy were gained (table 1, figure 2).
Leukemia was the main cause of YLL for children (48-50% of YLL), followed by cancers of the central nervous system (15-16%), lymphomas (6-10%) and kidney cancers (3-4%), which were stable over time; these four cancer types explained 75% or more of childhood cancer deaths during the study period (figure 3). During this period, YLL for childhood cancers dropped substantially, mainly due to decreases in lymphoma- and leukemia-related YLL. YLL for childhood cancers of the central nervous system and kidney remained rather stable.
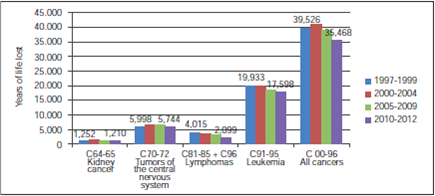
Figure 3 Years of life lost for cancers occurring during childhood (under 15 years of age), 1997-2012
The AYLL were very similar for childhood cancer, regardless of the cancer type, varying from 67.0 for colorectal cancer to 72.9 years for kidney cancer (results not shown).
Discussion
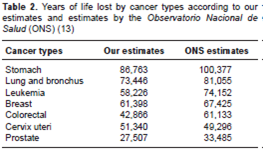
According to our results, the contribution of cancer to the total YLL in Colombia (15-20%) was lower than the one reported for western countries (25-30%) (6). Our estimates were also lower compared to the 2011 and 2015 Colombian studies produced by the Observatorio Nacional de Salud (ONS) (12,13) (table 2). Such differences are most likely due to the life expectancy tables of the Global Burden of Disease study used in ONS reports 12,13,15, which show higher life expectancy estimates, and, therefore, a higher number of YLL due to cancer. Although widely used and recommended, the disadvantage of Global Burden of Disease estimates is that they do not reflect the real number of years of life lost in local settings. Using optimal life expectancy gives a hypothetical number of life years lost, whereas in this study we were interested in the reality of the Colombian population. In addition, the ONS reports used 1998-2011 data, and did not apply redistribution of cases with unknown age or unspecified uterine cancer cases (14) as we did following international recommendations, wich could account for the higher YLL in our study.
Table 2 Years of life lost by cancer types according to our estimates and estimates by the Observatorio Nacional de Salud (ONS) (13)
YLL among the Colombian female population decreased, but the AYLL by cancer type was higher, largely because of women's longer life expectancy (78.5 years at birth in 2010-2012 versus 72.1 for males) (2). This is in line with the latest ONS study reporting neoplasms among the top three causes contributing to most YLL in females alone 12.
Breast and cervical cancer were very important contributors to female cancer mortality. Despite efforts to improve early detection and treatment of these cancers, YLL due to breast cancer increased substantially, with no reductions in AYLL; this indicates increasing number of breast cancer deaths with minimal improvements in age of death, as female life expectancy at birth increased by 3.6 years (from 74.95 in 1997-99 to 78.54 in 2010-12).
Virtually all cancer types showed AYLL of 15 or more years, with the exception of prostate and bladder cancer, which for 2010-12 contributed 11.3 and 13.7 years to the AYLL, respectively. In general, our results for AYLL were high when compared to international reports, which inform of less than 7 years AYLL for colorectal and breast cancer (USA), 1.8 for prostate cancer, and 13.8 for lung cancer (6,7,16). In a Polish study, only male brain cancer and cervical cancer showed more than 10 years of life lost per death (AYLL 10.7 and 10.2, respectively) 16.
Our figures, although not comparable with those from other countries due to differences in overall life expectancy and in the calculating methodologies, evidence the great disparity between estimates (less than 13.5 AYLL in the US compared to more than 15 years in Colombia, except for prostate and male bladder cancer), and confirm that cancer prognosis in our country is relatively poor. Breast cancer in the USA was responsible for 6.3 years of life lost per death, in Colombia this figure was 25.6 years, illustrating the combined effect of a usually very late diagnosis of breast cancer and/or its more frequent occurrence. Indeed, there is evidence that in Bogotá only 12-30% of women with breast cancer were diagnosed at the early stages, and that delays are substantial both for diagnosis and initiation of treatment 17,18.
Despite a high prostate cancer incidence in Colombia 19, the AYLL due to this cancer was relatively low compared to other cancer types, though high when compared to other countries, which could be attributed to the advanced age at diagnosis, and to its relatively good prognosis.
Leukemia frequently occurs amongst children and has a poor prognosis in Colombia, explaining the very high AYLL encountered for this cancer type. Not surprisingly, all childhood cancer deaths (all cancer types) had an AYLL of around 70 years, because of the very similar remaining life expectancy during childhood.
The YLL of leukemia increased among children and among all age groups, while AYLL of all cancers decreased substantially, indicating more deaths or later ages of death. However, AYLL in childhood leukemia slightly increased (64.6 to 67.8 among girls, 72.0 to 73.9 among boys), possibly due to increases in life expectancy, which indicates that no much progress has been achieved despite the special efforts displayed by the government since 2008 to reduce administrative delays 20-22. On the other hand, it could be attributed to an increase in the number of cases, as population-based survival estimates for childhood cancer show improvements in survival even if it still remains poor in Colombia 20,22,23. Indeed, long-term data from Cali show slight increases in childhood incidence of leukemia and central nervous system cancers (24). We observed no progress at all regarding childhood cancers of the brain and central nervous system, or for kidney cancers. YLL for childhood leukemia were higher than for brain and central nervous system cancers, although this difference is decreasing; it is conceivable that if the actions to improve leukemia prognosis in Colombia are successful, these two other type of cancers will be the main cause of cancer deaths amongst children, similar to the situation observed in the USA 10.
Despite the fact that good methods exist for early detection of breast, cervical, prostate and colorectal cancer, all of these cancer types showed stable or increasing YLL and AYLL, reflecting the great potential for improvements in their early detection in Colombia.
Our AYLL for breast and cervical cancer were much higher (around 25 years) than previous national estimates for 2007 (with 14.4 YLL for breast and 14.6 for cervical cancer), probably due to differences in the life expectancy information used 25. In a study estimating the burden of disease for the Colombian department of Santander, stomach cancer appeared as the first cause of "healthy" life years lost in men, followed by leukemia and colorectal cancer, while for females the first causes were cervical, breast and stomach cancers 12. In contrast, in our study lung cancer was among the first causes in males, while in females the top causes were the same as in Santander. As smoking habits and lung cancer mortality vary heavily within Colombia (smoking prevalence was lower in Santander than the Colombian average) 26,27, regional YLL estimates will vary substantially as well. Moreover, the Santander study reported healthy life expectancy using life tables from Japan as source for remaining life expectancy, which are not comparable to those we used, and this resulted in different life expectancies and, therefore, different YLL.
The observed YLL trends, with more than 40% increase in certain cancer types, are in line with the increasing life expectancy, and, perhaps, the recent efforts to diminish poverty rates in Colombia. This is in line with the fact that cancer types with increasing YLL (breast, colorectal, pancreas, kidney, bladder cancer and melanomas) are mostly related to a more "western" lifestyle and slowly replace the traditionally high burden of infection- and poverty-related cancers, such as gastric and cervical cancers. The increasing proportion of cancer deaths in the total death toll in Colombia is due to population ageing, but also to diminishing number of deaths due to violence (from 0.1% to 0.03% over the study period).
Even though gastric cancer mortality rates have significantly decreased (1), YLL and AYLL have increased, implying that their diagnosis is very late. Anti-tobacco measures should be strengthened to further reduce the burden of lung- and other tobacco-related cancers. Early detection and screening efforts, with a close and direct access to diagnosis and treatment of abnormal results, should be able to reduce breast, cervical and colorectal cancer mortality substantially. Even though interventions to improve survival in children with leukemia seem to be successful, survival rates are still very poor. In Cali, for example, population-based data from the cancer registry showed rates of only 55% in the most recent diagnostic period 23.
We used national mortality data, generally considered to have acceptable quality and to be among the best within Central and South America 28, particularly after redistributing the cases of unknown age and "uterus, not specified" cases. The quality of the coding in death certificates has improved over time and, therefore, misclassification may have been a larger problem in earlier periods. Indeed, the proportion of deaths with unknown age reduced over time, supporting this hypothesis. However, stable estimates or trends allow us to conclude that misclassification has been relatively minor, and it does not hinder deriving general conclusions such as those arrived at in our study.
Contrary to several previous studies, we did not use an external population to provide the expected remaining years of life at death (life expectancy from life tables), but rather the period and sex-specific life tables provided for Colombia by DANE. The advantage of this method is that it provides the most realistic YLL and AYLL estimates, as they are based on the local real life tables for the corresponding periods. In this respect, we took into account the substantial increases in life expectancy among Colombian population in calculating the trends. However, these improvements in life expectancy may hide other improvements also achieved. If deaths in recent periods occurred at the same ages as before, more potential years of life would be lost and, therefore, the trend would be negative.
Consequently, the stable trends observed may suggest an improvement, which is not apparent because of overall life expectancy improvement. Similarly, YLL increases in this study may not be so much a deterioration as a stabilization of the status quo, due to this increased general life expectancy, while AYLL decreases, mainly in leukemia, lymphomas, cancers of the central nervous system and melanomas (cancers ideally occurring at relatively young ages), actually mean even larger improvements regarding the average age at death. Indeed, in sensitivity analyses using 2010-2012 life expectancy for all periods, AYLL increased in earlier periods (i.e., more years lost given higher life expectancy). Tendencies, however, remained the same (supplementary table, available in: doi: http://dx.doi.org/10.7705/biomedica.v36i4.3207)
Together with cancer incidence, mortality and survival statistics, YLL and AYLL provide information on the burden of disease in a population. With increasing life expectancy and population size, the burden of cancer in Colombia is unsurprisingly also increasing. The AYLL was very high for many cancer types, and although comparisons with other countries are difficult given their different population structures, it is clear that primary or secondary prevention, early detection and more timely and adequate treatment can prevent many cancer deaths. The marked increases in YLL observed for colorectal, breast, ovarian and pancreatic cancer are worrisome and call for urgent preventive measures. Melanoma is another largely avoidable cause of death, while the lack of progress in AYLL for childhood leukemia also gives large room for improvement. Given population growth and aging in the country, there is need of more health workers specialized in oncology and preventive medicine.

