











 English (pdf)
English (pdf)
 Article in xml format
Article in xml format Article references
Article references
 Send this article by e-mail
Send this article by e-mail Cited by SciELO
Cited by SciELO  Cited by Google
Cited by Google  Similars in
SciELO
Similars in
SciELO  Similars in Google
Similars in Google 
 Permalink
PermalinkThe decline of the under-5 mortality rate (U5MR) worldwide has been one of the public health successes of the last five decades 1,2. Despite this, some countries have experienced stepped increases in the U5MR, making it an important source of inequity in countries worldwide 1,2.
Acute respiratory infections (ARI) are a major cause of morbidity and mortality in children, especially in low-income countries 2-4. Around 1.9 million children die annually as a result of ARI, 70% of them in Africa and Southeast Asia 5. ARI is among the top three causes of mortality in children under-5 years 6-8.
In Colombia, as in most Latin American countries, the infant mortality rate (MR) has declined in recent years 9: while in 2005 the infant MR was 20.4 per 1,000 live births, in 2013 it was 17.5. Although the recent gains in overall health are encouraging, some Colombian regions have not benefitted, and inequality remains a major concern. For example, in Amazonas, a rural department, the rate of death in infants has increased 4-fold compared to the department with the lowest mortality (Quindío) 10.
The Instituto Nacional de Salud reported in all age groups 5.5 million ARI outpatient and emergency consultations in 2015, 200,000 hospitalizations for severe ARI, and 13,000 critical care admissions 11. The U5MR for ARI in Colombia was 12.1 per 100,000 children in 2015 7.
Over the last decades, the socioeconomic conditions of Colombia have improved and, therefore, the evaluation of the effects on inequality in mortality and its main causes is useful 12. The World Bank reported poverty, measured as populations living with less than $1.9 a day (purchasing power parity dollars), as 16.4% in 2000 and 5.7% in 2013. Also, the Gini index has gone from 58.7 to 52.9, during the same time frame 12.
Several studies have estimated the impact of socioeconomic inequalities as determinants of population health, including some theoretical approaches that have sought to explain the potential effect of inequalities on various health outcomes 13-15. Infant mortality rate, as a main health outcome, has been traditionally used as an indicator to measure human development 16,17.
Most of the research on health inequalities in Colombia has not analyzed the relationship between inequalities in child mortality due to ARI and socioeconomic status. Thus, the aim of the present study was to explore the inequalities in the U5MR due to ARI by sex for the years 2000, 2005, 2010, and 2013 according to some of the socioeconomic characteristics of the Colombian population.
Materials and methods
Study design and population
We designed and carried out an ecological analysis to describe the inequalities at the national and municipal level in ARI-related U5MR in Colombia. Colombia has 32 departments, one capital district, 1,101 municipalities, and 21 non-municipalized areas 18. The country has high social and economic inequalities 19. Between 2002 and 2012 the incidence of poverty at the national level decreased from 49.7 to 32.7%, and the Gini coefficient fell from 0.572 to 0.539 20.
Variables
We obtained data from official death records of the Departamento Administrativo Nacional de Estadística (DANE), which collects, cleans and disposes vital statistics in Colombia 21. We gathered death data in the under-5-year-old population with the International Classification of Diseases (ICD-10) codes J09-J11, J12, J13, J14, J15-J22, J85, and P23, stratified by sex. We excluded from the analysis deaths with no information about sex, age or geographical location. We did not adjust for underreporting of mortality. The population data was extracted from projections based on the 2005 Colombian census 22.
We included the Unmet Basic Needs Index (UNI) and the Multidimensional Poverty Index (MPI), both reported by municipalities in the DANE’s records for 2011. The NBI is a proxy of poverty in the population including inadequate housing, overcrowded housing, substandard housing, economically highly dependent housing, and homes with school-aged children who do not attend school, and it is reported as the percentage of households in poverty 23. The MPI measures different aspects of households living conditions and it is a complementary measure to obtain an overview of poverty in the country (educational conditions of the home, conditions of children and youth, health, work and access to public services and housing conditions) 24. The MPI is also reported as the percentage of households living in poverty.
Data analysis
Data gathering and analysis were done in Microsoft Excel™, Stata 12™ (Stata Corporation, College Station, TX, USA) and the R programming software. All analyses were stratified in boys and girls.
The analysis of inequalities in the U5MR included: 1) Classification of the population in different poverty indexes (NBI), and 2) measurement of the degree of inequality 25,26. We used the ARIU5MR as an outcome measurement. The mortality rates were estimated at the national and municipal levels for the years 2000, 2005, 2010 and 2013 in order to show the change in inequality over time.
To measure the degree of inequality, we used simple and complex epidemiological measures based on methods developed by Mackenbach, et al. 27 and Schneider, et al. 28 mainly rate ratios (RR), rate differences (RD), and concentration curves 29. The ARI-related mortality RRs and RDs at municipal level were estimated according to NBI terciles. The RR compares the U5MR with high and low socioeconomic status 28,30, as well as the absolute variation of health results in U5MR in territories with high and low socioeconomic status 28,30.
Finally, we built concentration curves to visualize inequalities by ordering the outcome according to the socioeconomic status from the most to the least vulnerable. If the health outcome is equally distributed across the population, the concentration curve will coincide with a 45-degree diagonal 30. For the present study, ARI deaths were ordered according to the MPI from the poorest to the richest municipalities.
Results
In Colombia, 2,720,653 all-cause deaths occurred in all age groups between 2000 and 2013, 185,153 of them in children under-5 years and 9.7 % (18,012) of these were caused by ARI; 26 (0.5%) deaths were excluded for the years 2000, 2005, 2010, and 2013 because of the lack of information. Table 1 shows a breakdown of the characteristics of the population and the deaths in Colombia over the period.
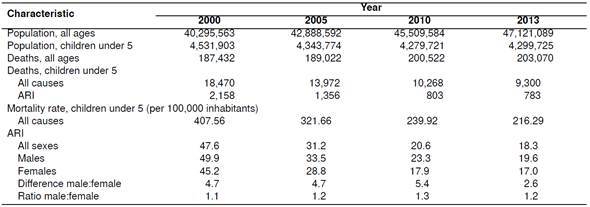
Figure 1 shows that the ARI-related U5MR was greater in boys than in girls. In 2000, ARI-related U5MR was 49.9 per 100,000 inhabitants (95% CI: 40.1-59.7) for boys and 45.2 (95% CI: 31.4-59.1) for girls. In 2013, a remarkable decrease was observed on U5MR by sex. The RD in ARI-related U5MR between boys and girls was 4.7 deaths per 100,000 inhabitants in 2000, decreasing to 2.6 deaths per 100,000 inhabitants in 2013 (table 1).
From 2000 to 2013, we observed an increase in the ARI-related U5MR mortality relative gap in boys and girls. Inequality gaps (i.e., ratios of mortality rates) and municipal ARI-related U5MR are shown in figure 2.
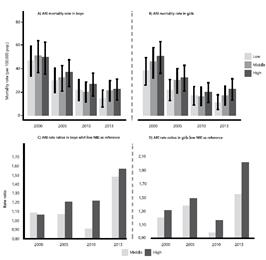
Figure 2 Children under 5 years mortality rate and ratios of mortality rates caused by ARI according to municipal terciles of poverty (NBI) and sex
In 2013, the risk of deathin boys under 5 years in municipalities with the highest poverty (high tercile) had an increase of 1.6, compared to those in municipalities with the lowest poverty (low tercile). In girls, for 2005 and 2013 the ARI-related U5MR in the poorest tercile (high tercile) was 1.5 and 2 times greater than the first tercile (low UNI tercile), respectively (figure 2).
When analyzing the distribution of ARI deaths in boys and girls with the concentration curves for the period 2011-2013 (figure 3), we found that 52% of ARI deaths in boys were concentrated in 15% of the population with the highest MPI (the poorest). In girls, 52% of deaths occurred in 22% of the poorest population measured by the MPI.

Discussion
The present study is one of the first to describe the socioeconomic inequalities in ARI-U5MR in Colombia. Studying infant mortality in developing countries is important and necessary, especially because infants are more vulnerable to suffering from ARI. Infant mortality is an indicator of the economic and social conditions of a country, as well as its health system’s efficiency 31,32. We observed how, in spite of a decrease in the national ARI-U5MR trend in both sexes, important inequalities persist in Colombia between the poorest and richest municipalities. However, a slight fall in the absolute gap of mortality rates due to ARI between boys and girls was also evident.
The decreasing trend in the national ARI mortality could be related to improvements in the health system and new public policies. Several initiatives sponsored by the Colombian Presidency have primarily targeted families living in poverty. For instance, the Familias en Acción program has improved nutrition status in poor children under 18 years by fostering nutritional and health care habits, as well as the nutritional monitoring of children by means of conditional transfers 9.
In terms of policies focused on improving and maintaining the health of children and reducing inequality gaps, Colombia has developed strategies to improve infant health, such as the National Health Plan for 2007-2010 33, which was followed by the Decennial Public Health Plan 2012-2021 9.The component of integral and differential care for children and adolescents in these plans is intended to reduce the adjusted national infant mortality rate and progressively reduce barriers to access health services for children and adolescents in order to reduce inequities 9. Also, pneumococcal, Haemophilus influenzae type b, and pertussis (for pregnant women) vaccines have been introduced in the expanded program of immunization since 2001 34-36, measures that may explain the reduction in the general national ARI-U5MR trend.
Social inequality is the new challenge for Colombian decision makers.The municipal ARI-U5MR analysis for poverty showed that the relationship between the socioeconomic level and ARI deaths is evident. The rate ratios analysis indicated how ARI-U5MR is higher in boys, but inequalities among girls increased during the study period. Previous studies have shown that boys die more than girls from a wide array of underlying conditions (RR=1.44; 95% CI: 1.44-1.45) 37. As stated in its Decennial Public Health Plan, Colombia aims at increasing the availability of information and evidence on social and economic inequalities and health inequities to guide policies and interventions in vulnerable territories and groups by 2021 38.
Mortality due to ARI is a tracer indicator of social inequalities. Epidemiological studies have shown that the population health presents a strong social gradient, invariably unfavorable to the socially less favored groups 39. Studies in Chile and Brazil on inequalities in infant mortality according to socioeconomic indicators have shown similar results to those from our study 40,41. For instance, in Chile, Frenz, et al., observed a clear gradient of infant mortality rates according to the number of years of maternal education taken as a socioeconomic variable from 1998 to 2000 and from 2001 to 2003 40. Also, in a multi-country analysis developed by McKinnon, et al., the wealth-related inequality increased by more than 1.5 neonatal deaths per 1,000 livebirths per year in Ethiopia and Cambodia 42.
Colombia is a country with very serious economic inequalities. However, it is not easy to show inequalities in health. In our study, we were able to explore ARI mortality inequalities in children under 5 using socioeconomic variables such as the NBI or the MPI. Even though our results should be interpreted with caution 43, they are important to study health inequities in one of the most unequal countries in Latin America.
This work poses great challenges for public policies aimed at reducing inequalities in ARI mortality in children under 5 in Colombia. It would be expected that management-aimed improvements to strengthen health institutions and services would prevent deaths in children. The ARI MR inequalities in the poorest municipalities compared with the richest continue to be a major public health challenge for the country.
Our analysis has limitations. First, the quality of the data: the DANE’s vital statistics should be used with caution because in some territories results are underestimated as they do not take into account possible omissions of vital events occurring outside the health system. Thus, our results could have also underestimated the mortality rates measured with inequality indexes, especially in the poorest municipalities, where under reported data are most likely.
Second, we did not consider the under-registration of births and deaths in some municipalities due to dispersion in the territory, or lack of reporting due to cultural factors, nor the fact that there are health institutions that do not regularly report the vital facts 44. Nevertheless, data on economic variables and deaths for the entire timeframe are available aggregated by municipalities. As in most ecological studies, we assumed that inferences made at the general level would apply to individuals 9,45.
The main strength of the study resided in the analysis of ARI mortality inequalities at the municipal level, which is more disaggregated than the usual mortality analyses in Colombia. Likewise, the time period analyzed allowed us to observe significant changes in mortality from ARI in children under 5.
In conclusion, although ARI mortality rates in children under 5 decreased during the study period, the ARI mortality gap has increased among Colombian municipalities and this continues to be a huge challenge for Colombian stakeholders. The next step in our work is to understand why ARIrelated U5MR inequalities have increased in some territories

