










Services on Demand
Journal
Article
 English (pdf)
English (pdf)
 Article in xml format
Article in xml format Article references
Article references
 Send this article by e-mail
Send this article by e-mailIndicators
-
 Cited by SciELO
Cited by SciELO -
 Access statistics
Access statistics
Related links
-
 Cited by Google
Cited by Google -
 Similars in
SciELO
Similars in
SciELO -
 Similars in Google
Similars in Google
Share

 Permalink
PermalinkInvestigación y Educación en Enfermería
Print version ISSN 0120-5307
Invest. educ. enferm vol.30 no.3 Medellín Sept./Dec. 2012
ARTÍCULO ORIGINAL / ORIGINAL ARTICLE/ ARTIGO ORIGINAL
Coping and adaptation and their relationship to the spiritual perspective in patients with HIV/AIDS
Afrontamiento y adaptación y su relación con la perspectiva espiritual en el paciente con VIH/SIDA
Afrontamento e adaptação e sua relação com a perspectiva espiritual no paciente com HIV/AIDS
Beatriz Pérez-Giraldo1;Mónica del Mar Veloza-Gómez2; Jorge Eduardo Ortiz-Pinilla3
1 RN, M.Sc., Faculty of Nursing and Rehabilitation, Universidad de La Sabana, Colombia. email: beatriz.perez@unisabana.edu.co.
2 RN, M.Sc., Faculty of Nursing and Rehabilitation, Universidad de La Sabana, Colombia. email: monica.veloza@unisabana.edu.co.
3 Statistician, Faculty of Statistics, Universidad Santo Tomás, Colombia. email: jorgeortiz@usantotomas.edu.co.
Receipt date: June 10th 2011. Approval date: March 23rd 2012.
Subventions:Dirección de Investigación de la Universidad de La Sabana.
Conflicts of interest: none.
How to cite this article: Pérez-Giraldo B, Veloza-Gómez MM, Ortiz-Pinilla JE. Coping and adaptation and their relationship to the spiritual perspective in patients with HIV/ AIDS. Invest Educ Enferm. 2012;30(3):330-338
ABSTRACT
Objective. To identify the coping and adaptation process and its relationship to the spiritual perspective in patients with HIV/AIDS. Methodology. Cross-sectional descriptive study in which 100 patients participated and who were applied instruments like Roy's coping and adaptation measurement scale and Reed's Spiritual Perspective Scale. The study was conducted in 2009, at a state healthcare institution in Bogotá (Colombia). Results. Five patient subgroups were identified (Recursive and Centered, Physical and Focused, in warning process, in systematic processing, and knowing and relating) who presented different dynamics regarding the greater or lesser use of coping strategies. In most patients a high spiritual perspective was identified upon the experience of the disease. A weak, but significant correlation was found between the coping and adaptation processes and the components of the spiritual perspective. Conclusion. A relationship exists between the spiritual perspective and the coping and adaptation process to the HIV/AIDS disease; the aforementioned must be considered in the therapeutic relationship as a relevant component of caretaking.
Key words: spirituality; psychological adaptation; HIV.
RESUMEN
Objetivo. Identificar el proceso de afrontamiento y adaptación y su relación con la perspectiva espiritual en el paciente con VIH/SIDA. Metodología. Estudio descriptivo transversal en el que participaron 100 pacientes a quienes se les aplicaron los instrumentos Escala de Medición del Proceso de Afrontamiento y Adaptación de Roy, y la Escala de Perspectiva Espiritual de Reed. El estudio se realizó en 2009, en una institución estatal de salud en Bogotá (Colombia). Resultados. Se identificaron cinco subgrupos de pacientes (recursivo y centrado, físico y enfocado, en proceso de alerta, en procesamiento sistemático y conociendo y relacionando) quienes presentaron diferentes dinámicas en cuanto al mayor o menor uso de las estrategias de afrontamiento. En la mayoría de pacientes se identificó una alta perspectiva espiritual ante la vivencia de la enfermedad. Una débil pero significativa correlación se encontró entre los procesos de afrontamiento y adaptación y los componentes de la perspectiva espiritual. Conclusión. Existe relación entre la perspectiva espiritual y el proceso de afrontamiento y adaptación a la enfermedad del VIH/SIDA. Lo anterior debe ser tenido en cuenta en la relación terapéutica como componente relevante del cuidado.
Palabras clave: espiritualidad; adaptación psicológica; VIH.
RESUMO
Objetivo. Identificar o processo de afrontamento e adaptação e sua relação com a perspectiva espiritual no paciente com HIV/AIDS. Metodologia. Estudo descritivo transversal no que participaram 100 pacientes a quem se lhes aplicaram os instrumentos Escala de Medição do Processo de Afrontamento e Adaptação de Roy, e a Escala de Perspectiva Espiritual de Reed. O estudo se realizou em 2009, numa instituição estatal de saúde em Bogotá (Colômbia). Resultados. Identificaram-se cinco subgrupos de pacientes (recursivo e centrado, físico e enfocado, em processo de alerta, em processamento sistemático e conhecendo e relacionando) quem apresentaram diferentes dinâmicas quanto ao maior ou menor uso das estratégias de afrontamento. Na maioria de pacientes se identificou uma alta perspectiva espiritual ante a vivência da doença. Uma débil, mas significativa correlação se encontrou entre os processos de afrontamento e adaptação e os componentes da perspectiva espiritual. Conclusão. Existe relação entre a perspectiva espiritual e o processo de afrontamento e adaptação à doença do HIV/AIDS, o anterior deve ser tido em conta na relação terapêutica, como componente relevante do cuidado.
Palavras chaves: spiritualitye; adaptação psicológica; HIV.
INTRODUCTION
Human beings have the potential to develop their life projects, which can be affected by the experience of chronic diseases, where spirituality and the coping and adaptation process emerge as human expressions in search of balance or of improving quality-of-life conditions. Situations of chronic disease like HIV/AIDS affect the individual's integrity, influencing on his/her physiological processes, as well as on psychosocial aspects represented on the performance of their roles, in their interaction with the environment and on the concept of self.1,2 Thus, the individual endures uncertainty, vulnerability, fragility, anxiety, fear,
suffering, and pain, and wonders about a past, present, and future.2 The figures of this disease throughout the world show the great impact it has on the lives of patients and of their families: the number of people living with HIV/AIDS has gone from 8-million in 1990 to over 33-million cases in 2009, and it is on the rise.3
Roy's Adaptation Model4 suggests that individuals are holistic adaptative systems in constant interaction in a changing environment. The term coping4 refers to the los behavioral and cognitive efforts made by the individual to meet the environmental demand acting as a whole to maintain his/her vital processes and integrity. Through the development of the information cognitive process, people assign meanings to situations framed within their experience and knowledge, and based on them, elaborate responses that permit their facing the circumstances.
Reed5 defines the spiritual perspective as the personal vision to find meaning in life through a sense of interrelation with something greater than the very being, which transcends the self and enhances it in a way that empowers individuals without devaluating them. This interrelation can be intrapersonal (with oneself), interpersonal (with the world: others and nature), or transpersonal (with a transcendent being: God, or a greater power than the individual's common origin). Transcendence is present in these interrelations, seen as a faculty of the individual. Additionally, it alludes to the spiritual perspective as a behavioral and personal view (beliefs) that expresses a sense of transcendental relationship with someone superior, being a particularly important experience during the adult stage that is intensified with the nearness of death.
Spirituality can be identified by the nursing professional as a resource of great value for caregiving, given that it can be conceptualized as a component of the therapeutic relationship in favor of human health and well-being. Reed6 suggests that spirituality is part of the ontological basis of nursing, por ser una basic characteristic of humanity. Thus, the spiritual perspective and the coping and adaptation process can be considered integrally, as human expressions that intervene upon the experience of any disease, among them HIV/AIDS.
Now, most scientific literature related to nursing caregiving of these types of patients centers on interventions of physiological aspects, leaving aside the human being's integrality. This situation has repercussions on the very conceptualization of caregiving, given that it does not consider the person to be cared for as a holistic being, not considering his/her cognitive, spiritual, and social essence in the search for well-being. This study sought to identify the coping and adaptationprocess and its relationship to the spiritual perspective in patients with HIV/AIDS.
METODOLOGY
This was a cross-sectional descriptive study. A non-probabilistic sample was taken of 100 patients with at least six months of having been diagnosed with HIV/AIDS, who were not in the terminal phase, hospitalized, or in outpatient care in a public sector healthcare institution in the city of Bogotá (Colombia) between November 2008 and January 2009.
To gather the information, the following instruments were used: Roy's coping and adaptation measurement scale4 in its Spanish version (EsCAPS) and the Spiritual Perspective Scale (SPS) by Pamela Reed6.
The Spanish version of the EsCAPS7 comprises 47 items, with four Likert-type response options, (4 = always, 3 = sometimes, 2 = rarely, and 1 = never). The scale permits identifying the coping and adaptation strategies the person uses to face difficult or critical situations. Through factor analysis, Roy4 defined five subscales or factors corresponding to strategies interpreted by the middle range theory of the coping and adaptation process.
The first factor, Recursive and Centered, reflects behaviors that use own and external resources centered on expanding the information input phase, to be creative and seek results. The second, Physical and Focused, highlights the physical reactions and the information input phase to manage situations. The behaviors of the physical and personal self focused on the three phases of information processing (input, central processing, and output) are considered in the third factor denominated warning process. The personal and physical strategies used in the methodical management of situations make up the fourth factor known as systematic processing. The fifth factor, knowing and relating, describes own and other's strategies to manage situations by using memory and imagination4.
Regarding the EsCAPS psychometric capacity, the instrument has a good face or apparent value and a high test-retest correlation (0.90 for factor 1, 0.94 for factor 2, 0.91 for factor 3, 0.92 for factor 4, 0.92 for factor 5). The instrument's reliability, measured via Cronbach's alpha, was also high at 0.88.7 This scale has been validated in Spanish in groups of patients residing in Panama and Mexico.8
This study agreed to use the average by factor and total of the scale, to keep differences in the quantities of items from generating comparative difficulties. The second scale used was the SPS Reed,5 which comprises 10 items, with Likert-type response options going from 1 (less spiritual perspective) to 6 (greater spiritual perspective). The first four items refer to the person's behaviors and the last six to the spiritual beliefs. The total score corresponds to the sum of the scores of the ten items. The original scale has an internal consistency through a Cronbach's alpha of 0.91.6
In Colombia, a study was conducted with abused women, showing an internal consistency of 0.8.9 This research was approved by the Ethics Committee at Universidad de La Sabana. The ethical aspects considered were the informed signed consent and the confidentiality of the information furnished by the patients. The two instruments were used under authorization from the authors.
For the statistical analysis, Wilcoxon, Kruskal-Wallis, and Spearman non-parametric tests were used. To obtain information on the individual emphasis on aspects of the coping and adaptation process, the positions of the scores of the five EsCAPS factors were taken for each patient. With these, a cluster analysis was applied as an exploratory method to organize homogeneous groups with more than six patients from their profiles of relative responses. The resulting groups were subjected to analysis by the researchers to generate caregiving guidelines as a function of the characteristics identified.
As a response pattern, it was considered to transform the raw sores from the five factors of the EsCAPS scale into evaluative scores of the relative importance given to each factor in relation to the rest. This score consisted of assigning the range of the raw score for a specific factor like the amount of factors receiving from the patient a score below or equal to that of said factor. In case of equal scores, the middle ranges were considered. The items from the instrument organized into five factors were used as the cluster variables. With the relative score information was obtained on the importance each patient attributed to each factor with respect to the rest. The aforementioned permitted clearly establishing the personal emphasis for aspects evaluated of the coping and adaptation process. This managed to reduce, in part, the problems related to the results of the analysis of the internal consistency of the factors, given that the strict numerical score was not kept in mind but its relative value with respect to the other factors from the instrument.
RESULTS
The study group was made up of 100 patients, 14 women and 86 men, with mean ages of 31 ± 9.1 and 38 ± 9.3 years, respectively. A total of 92 patients were being cared as outpatients and eight were hospitalized. The average time elapsed after the diagnosis was of 56 ± 48.8 months until the moment of the interview. Of the total number of patients, 93 were in socioeconomic level 3 and less. Schooling conditions were of primary education for 17 of them, secondary for 64, university for 15, and graduate education for four. Of the participants, 62 were employed and 38 were unemployed. The most usual form of cohabitation for the patients was of atypical families (46), followed by nuclear families (28), modified nuclear (15), and extended (11). The religious affiliation was predominantly Catholic (66) or Christian (22); two were Evangelists and one Buddhist; four manifested believing in the existence of a supreme being, although they had no particular religion, and five did not profess any religion.
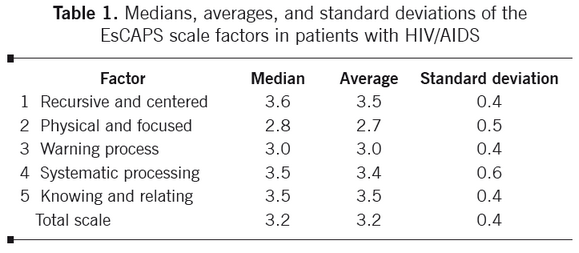
Coping and adaptation process. Table 1 contains the medians, averages, and standard deviations of the coping and adaptation factors. Three of the
five factors have averages and medians above 3.4 and the total of the scale at 3.2, which would indicate a frequency above 'sometimes'.
With the socio-demographic variables significant associations were only found among some of the coping and adaptation factors with gender and schooling, thus:
The medians of the EsCAPS total were 3.3 for women and 3.2 for men, without this difference being significant (Wilcoxon W = 710, p = 0.28). When comparing the average score per gender of factors 1, 2, 3, and 5, only in factor 4 - systematic processing, the women presented an average score above that of the men (3.8 and 3.5, respectively), which was statistically significant (W = 836, p = 0.02).
The Kruskal Wallis test for the education groups reveals as the only significant differences those corresponding to the Physical and Focused factor, with medians obtained in the primary, secondary, university, and graduate levels of 2.5, 2.7, 3.0, and 3.4, respectively (Kruskal-Wallis K = 13.8, p < 0.01). When Spearman's correlation coefficients were calculated among schooling variables and each of the factors of the coping and adaptation process and for the scale total, significant correlations were only noted in the Physical and Focused factor (Rho = 0.36, p = <0.001) and for the total scale (Rho = 0.22, p = 0.03).
Groups of characteristic profiles. Five groups were identified, denoted in Table 2 as profiles 3, 4, 6, 7, and 8. As a general pattern, the low relative score is identified, which is found in the Physical and Focused factor in most of the groups. The warning process is the following factor with lower scores, while for the Recursive and Centered, systematic processing, and knowing and relating there are higher average evaluations.
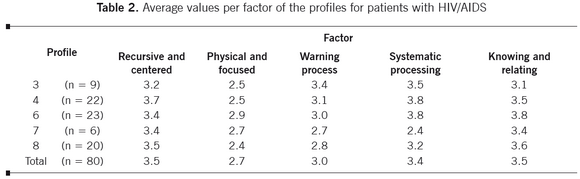
Group 3 is characterized by the highest evaluation of warning process and systematic processing and by the low score of Physical and Focused against the other factors as the most outstanding contrast of its profile. In group 4, the contrast of Physical and Focused is attenuated with the warning process, but it is accented with the remaining factors, especially with Recursive and Centered and systematic processing, which are the most highly evaluated by these patients. The profile of group 6 presents the highest averages in systematic processing and knowing and relating, contrasting with Physical and Focused and warning process, although the profile is slightly more balanced than in the other groups.
Group 7 is the only one where three factors are found below 3.0 (Physical and Focused, warning process, and systematic processing). The highest contrast of scores appears between the Recursive and Centered and knowing and relating factors, as those with the highest averages, and systematic processing as the one with the lowest average for these patients. Patients from group 8 assigned higher average scores to the Recursive and Centered and knowing and relating factors in contrast to a low score for Physical and Focused. Lastly, it is clarified that 20 patients presented profiles that could not be classified into groups of acceptable size.
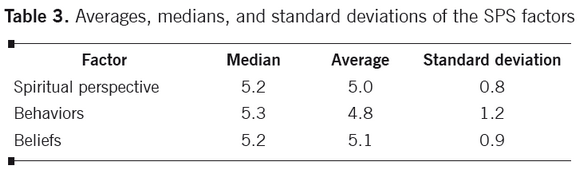
Spiritual perspective. Table 3 summarizes the classical descriptive measurements for the components from the SPS scale. The medians show that at least half the patients obtained scores above or equal to 5.2 and the averages were close to 5.0; considering that the maximum value possible in the spiritual perspective is of 6.0, we could speak of a high perspective.
The SPS median in women (5.3) was above that of men (5.1) in the spiritual perspective; additionally, the difference was statistically significant (W = 810, p = 0.04). In the behaviors, the median for women was 5.4 and that of men was 5.0 and their difference was not significant (W = 786.5, p = 0.07). Differences in spiritual beliefs were even lower: women had a median of 5.3 and men of 5.2 (W = 37.5, p = 0.18).
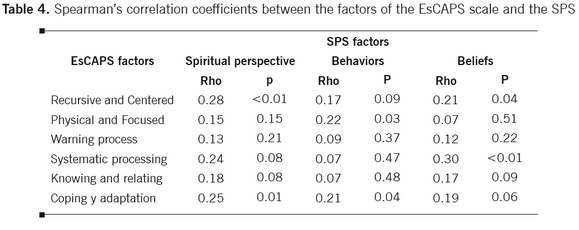
Relationship between the spiritual perspective and the coping and adaptation process.Table 4 shows that all the Spearman's correlation coefficients between the components of the two tests are positive, indicating that, in general terms, the coping and adaptation process and the spiritual perspective are directly related. Thus, it is shown by the significant correlation among the total scores of the instruments and, particularly,the total score of the EsCAPS with the spiritual behaviors.
In turn, the total score of the SPS scale presents significant correlations with the la EsCAPS Recursive and Centered and systematic processing factors and these with the beliefs from the SPS. The Physical and Focused factor was only significantly correlated with the behaviors component, but not with the total of spiritual perspective.
None of the coefficients among the factors from the EsCAPS of warning process and knowing and relating with the spiritual perspective from the SPS was significant. Seven of the 18 correlations presented in Table 4 are significant, but only two of them are slightly above 0.28, indicating weak correlations.
DISCUSSION
The coping and adaptation process presented by the patients in the study upon the HIV/AIDS experience is evidenced through the use of the coping strategies posed by Roy, represented in the behavioral and cognitive efforts made by the individuals to meet the demands of the environment, which act as a whole to maintain their vital processes and their integrity.4
Each of the five groups of patients identified in the study presents its own dynamics regarding a greater and lesser stability in using these strategies represented through the factors or subscales that are part of the EsCAPS (Factor 1: Recursive and Centered; Factor 2: Physical and Focused; Factor 3: Warning process; Factor 4: Systematic processing; Factor 5: Knowing and relating). 4,10
These strategies are the result of the person's management process of the situation, by using the three phases of the information cognitive process: input - central processing - output, which is manifested through the generation of thoughts, feelings, and actions to accomplish coping with the situation, agreeing with the study by González8 conducted with patients suffering from coronary heart disease.
The socio-demographic variable referring to a high educational level is associated to greater stability in the use of coping strategies. This increasing tendency makes higher educational levels to be seen as associated to greater protection of the los patients against interferences that generate crisis in their activities and everyday worries; as suggested by Roy,4 individuals use their knowledge and prior experiences to process information to manage coping to adapt upon the situation. Hence, greater education is associated to higher levels of protection of the patients against interferences that generate crisis in their activities and everyday worries.
In the study, the spiritual perspective plays an important role regarding the HIV/AIDS experience; patients allude to it as an important aspect highly present and deeply rooted in their behaviors and in their beliefs. Some studies11,12 coincide with this appreciation by patients with HIV/AIDS. Also, the spiritual perspective of patients represented by their spiritual beliefs is supported by that posed by Emblen13 when considering that these emerge from within, may emerge from their intellect and are influenced by their conduct, serve as a guide to aspects of daily living, become sources of support and inner strength that promote the individual toward an optimal level of well-being.
Patients consider spiritual issues as quite important and influencing in their lives and frequently evoke them in their conversations with friends, during moments they share with others, and in their readings, besides having a regular habit of prayer or meditation. Additionally, within the patients' spiritual perspective, forgiveness is manifested as a spiritual belief and it is supported by that posed by Reed inasmuch as it is an important aspect to highlight related to spirituality, both in the religious and non-religious sense, upon promoting the sense of connection with oneself, with other people, and with a God or a superior power. It bears a therapeutic value represented in facilitating the connection through the dissolution of excessive guilt felt within oneself, expectations of criticism from others, of criticism from others and the solution of hostility toward the rest.6
As part of the patients' spiritual perspective, the socio-demographic variable, religious affiliation, are shown as a spiritual behavior where Catholicism and Christianity translate into aspects that motivate sharing spiritual aspects with others where reference is also made of reading spiritual material, meditation, and praying as behaviors that intervene in managing the difficult situation. Catholics, but more so Christians, manifest their religious affiliation in more rooted manner than those patients who manifest other religious affiliations or those who state having no religious affiliation. These results are related to the studies conducted by Kudel et al.,14 and Hsiao et al.15
This study permitted knowing the dynamics of the spiritual perspective and of the coping and adaptation process, variables that in spite of presenting a weak correlation can be identified as complementary and significant dimensions regarding the HIV/AIDS experience.
As a relevant component of caregiving, the therapeutic relationship becomes an important reference for the expression of these resources of human nature upon the HIV/AIDS experience. The conclusion of this study is that a weak, but significant relationship exists between the spiritual perspective and the coping and adaptation process, becoming resources of human nature of great relevance upon caring for the person living with HIV/AIDS.
Acknowledgments: the authors specially thank Dr. Callista Roy, author of the Coping and Adaptation Process Measuring Scale, and Dr. Pamela Reed, author of the Spiritual Perspective Scale (SPS), for their kind authorization for the use of the tests in the Spanish versions. We thank the Ethics Committee from the Health Institution for their collaboration in the development of the research. Gratitude is also expressed to nursing students Alba Luz Urrego, ángela Morales, Karen Martínez, and Miriam Patiño for their active participation in the research and to the patients who accepted to participate in spite of their particular health circumstances.
REFERENCES
1. Richardson C, Poole H. Chronic pain and coping: a proposed role for nurses and nursing models. J Adv Nurs. 2001 34(5):659-67. [ Links ]
2. Arrivillaga M, Correa D. Abordaje integral de la enfermedad crónica. Psicología de la salud. Madrid: Manual Moderno; 2007. [ Links ]
3. Naciones Unidas. Declaración Política sobre el VIH/SIDA. Intensificación de nuestro esfuerzo para eliminar el VIH/SIDA. New York: Naciones Unidas; 2001. A/65/L.77. [ Links ]
4. Roy C. The Roy Adaptation Model. 3th ed. London: Prentice Hall; 2008. [ Links ]
5. Kim SS, Reed PG, Hayward RD, Kang Y, Koenig HG. Spirituality and psychological well-being: testing a theory of family interdependence among family caregivers and their elders. Res Nurs Health. 2011; 34(2):103-15 [ Links ]
6. Jesse DE, Reed PG. Effects of spirituality and psychosocial well-being on health risk behaviors in Appalachian pregnant women. J Obstet Gynecol Neonatal Nurs. 2004; 33(6):739-47. [ Links ]
7. Gutiérrez C, Veloza MM, Moreno ME, Durán MM, López C, Crespo O. Validez y confiabilidad de la versión en español del instrumento 'Escala de medición del proceso de afrontamiento y adaptación' de Callista Roy. Aquichan. 2007; 7(1):54-63. [ Links ]
8. González Y. Evaluación de la Eficacia del Cuidado como Intervención Terapéutica en Personas que Padecen Cardiopatía Isquémica a partir del Modelo de Adaptación y la Teoría del Proceso de Afrontamiento y Adaptación de Roy. [Dissertationl] . Bogotá: Facultad de Enfermería, Universidad Nacional de Colombia; 2007. [ Links ]
9. Jaramillo D, Ospina D, Cabarcas G, Humpreys J. Resiliencia, espiritualidad, aflicción y tácticas de resolución de conflictos en mujeres maltratadas. Rev Salud Publica. 2005; 7(3): 281-92. [ Links ]
10. Roy C, Andrews H. Altered cognition: An information processing approach. In: MitchellP H, Hodges L, Muwases M, Walleck CA. American Association of Neuroscience Nurses' neuroscience nursing: Phenomena and practice. Norwalk: Appleton & Lange; 1988. [ Links ]
11. Cotton S, Puchalski CM, Sherman SN, Mrus JM, Peterman A, Feinberg J, et al. Spirituality and Religion in Patients with HIV/AIDS. J Gen Intern Med. 2006; 21(S5) S5-S13. [ Links ]
12. Tuck I, McCain N. Elswick R. Spirituality and psychosocial factors in persons living with HIV. J Adv Nurs. 2001; 33(6):776-83. [ Links ]
13. Emblen JD. Religion and spirituality defined according to current use in nurse literature. J Prof Nurs 1992; 8(1):41-47. [ Links ]
14. Kudel I, Cotton S, Szaflarski M, Holmes W, Tsevat J. Spirituality and Religiosity in Patients with HIV: A Test and Expansion of a Model. Ann Behav Med. 2011; 41(1): 92-103. [ Links ]
15. Hsiao AF, Wong MD, Miller MF, Ambs AH, Goldstein MS, Smith A, Ballard-Barbash R, Becerra LS, Cheng EM, Wenger NS. Role of religiosity and spirituality in complementary and alternative medicine use among cancer survivors in California. Integr Cancer Ther. 2008; 7(3): 139-46. [ Links ]
