










Services on Demand
Journal
Article
 text in
text in  English (pdf)
English (pdf)
 Article in xml format
Article in xml format Article references
Article references
 Send this article by e-mail
Send this article by e-mailIndicators
-
 Cited by SciELO
Cited by SciELO -
 Access statistics
Access statistics
Related links
-
 Cited by Google
Cited by Google -
 Similars in
SciELO
Similars in
SciELO -
 Similars in Google
Similars in Google
Share

 Permalink
PermalinkInvestigación y Educación en Enfermería
Print version ISSN 0120-5307
Invest. educ. enferm vol.31 no.1 Medellín Jan./Apr. 2013
ORIGINAL ARTICLE / ARTÍCULO ORIGINAL/ ARTIGO ORIGINAL
The nursing image and professional identity. The future of a construction
A imagem e identidade profissional de enfermagem. o devir de uma construção
Virginia Corina Samaniego1; Silvia Cárcamo2
1 Psychologist, Ph.D, Professor. Universidad Nacional de Lanús -UNLA-, Argentina. email: corina.saman@gmail.com.
2 RN, Specialist, Professor. UNLA, Argentina. email: scarcamo@unla.edu.ar.
Receipt date: November 21st 2011. Approval date: February 4th 2013.
Article associated with the research: Imagen profesional de enfermería entre los profesionales de la salud, entre pares y en la comunidad.
Subventions: Agencia Nacional de Promoción Científica y Tecnológica, Argentina.
Conflicts of interest: None.
How to cite this article: Samaniego VC, Cárcamo S. The nursing image and professional identity. The future of a construction. Invest Educ Enferm. 2013;31(1): 54-62
ABSTRACT
Objective. This study sought to describe the image nurses, physicians, and other healthcare professionals have of nurses. Methodology. We performed a descriptive study conducted in 2010 on a probabilistic sample of 308 participants (100 nurses, 103 physicians, and 105 other professionals) from Buenos Aires, Argentina. The study used questionnaires with multiple choice closed questions. Results. Among the main results, we found a perception of the working conditions that imply wear, helplessness, and conflicts within the work group with greater frequency among nurses than in other study groups. Likewise, discrepancies were found between what nurses and the rest of professionals consider 'specific nursing functions'. Conclusion. Tension exists between the role prescribed by the medical model and that defined by nursing. It is necessary to conceive how the professional identity is constructed as of identifying strategies resulting from objective and subjective strategies.
Key words: nursing; physicians; professional practice.
RESUMO
Objetivo. Descrever a imagem que enfermeiros, médicos e outros profissionais da saúde têm dos enfermeiros. Metodologia. Estudo descritivo realizado em 2010 numa mostra probabilística de 308 participantes (100 enfermeiros, 103 médicos e 105 outros profissionais) de Buenos Aires, Argentina. Empregaram-se questionários com perguntas fechadas de opção múltipla. Resultados. Entre os principais resultados se encontrou uma percepção das condições trabalhistas que implicam desgaste, impotência, conflitos no grupo de trabalho com mais frequência entre enfermeiros que nos outros grupos de estudo. Assim mesmo se encontraram discrepâncias entre o que os enfermeiros consideram como suas 'funções específicas' e o que consideram os outros profissionais. Conclusão. Existe tensão entre o papel prescrito pelo modelo médico e o que define enfermagem. é necessário conceber como a identidade profissional se constrói a partir de estratégias indenitárias resultantes de estratégias objetivas e subjetivas.
Palavras chaves: enfermagem; médicos; prática profissional.
INTRODUCTION
The quality of healthcare services received by the population turns out to be a priority in all societies because it is a social right to which the state must respond. One of the essential resources of the services are the healthcare workers and among them that of nursing has been internationally recognized as fundamental. Distinct national and international healthcare organisms have sought to analyze the situation around the problem of nursing human resources, their professional profile and their qualitative and quantitative characteristics.1-3
In diverse countries the problem has involved investigations inquiring on profiles, functions, image, and subjective perceptions of the workers in the field.4-9 In Cuba, for example, a study proposed the need to discriminate nursing profiles and functions at the university and technical levels within the nursing team and with other professionals, bearing in mind that the lack of definition of the functions bears an important repercussion for the profession because it makes it more difficult to consolidate accomplishing their professional identity.10 In Argentina, no prior studies exist addressing this particular issue.
The term profession has been analyzed from the sociology of the professions. One of the approaches of the field, the functionalist approach, has maintained that 'professions imply a specialized intellectual technique, acquired through a broad and formalized formation that permits offering efficient service to the community';11 in its developments, one of most analyzed professions has been the medical profession. Likewise, professionalization turns out to be a functionalist concept whose operational concretion from this approach must be given as of traversing a regular series of steps designed to bring about change within an occupation to raise it to professional status and which implies elevating the status of those who practice it, namely:12:28 1) presentation of an occupational group in an activity that demands exclusive dedication on a set of given problems. Previously, the group must have narrowed the field of activity, surely opposed by bordering occupations; 2) establishment of instruction and selection procedures, normally in specialized institutions (universities) where access paths are institutionalized; 3) constitution of a professional association, normally of national nature. This stage establishes and defines its occupational function, besides instituting models and norms at the core. It also serves to set apart relationships with other groups, especially competing groups; 4) the fourth phase carries out the movements of the profession to obtain legal protection, concretized in the public recognition and legal support to control, within a monopoly regime, its exercise, as well as access to the profession; and, finally, 5) the profession is provided with a code of ethics. However, compliance of said steps is far from bringing about synchronous social recognition as noted in multiple professions currently in existence, above all within the healthcare field, among them nursing.
From another vantage point, like that of symbolic interactionism,12 Hughes proposes that a profession or trade must be considered less as a set of activities and more as systems of activities in permanent evolution, where the evolution of a trade must be understood as a career. This author holds that professions have established a pact with society where in exchange for access to their knowledge on issues of vital human importance, society has conceded them a license to determine who will be part of its professional field, a high degree of autonomy in regulating its practice, and a special mandate on social control within its specialization areas.
Real12 analyzes another perspective, which is the analysis of knowledge and power. This author, citing Freidson and his analysis of the medical profession, indicates how by the end of the 19th century that profession, seeking to monopolize the healthcare market by joining prestige and expert authority, stops being an intellectual profession to become a consultation profession. This type of profession implies testing the solution of practical problems proposed by the lay person. Freidson, according to Real,12 takes into consideration another one of the issues that emerge in the medical profession, that of the internal monopoly of professional control. These professionals, with the growing imposition of their conceptions of health and disease, become determinant experts in health policies. Citing Real:12:38 for Freidson, the step from competence limited within a technical domain to general expertise in a social field constitutes a characteristic of modern professionalism. This would be a consequence of self-regulation of the professional autonomy that upon protecting the profession is incapable of 'assuming the self-regulation it promises'.
This last difficulty of the medical profession has to do directly with the case of nursing being one of the professions closest to the medical profession and which tries, as other healthcare professions, to define its field of action based on its own conceptions and theoretical development and not by those adjudicated from outside. This is how the International Nurses Council (INC) has issued an official document that establishes that the definition of the practice environment transmits to others the competencies and the professional responsibility of the nurse. Nursing is responsible for defining the nurse's functions and the practice environment of nursing. Nonetheless, even when it is incumbent on nurses, through professional and job relations and of regulatory organisms, the primary responsibility of periodically defining, supervising, and evaluating the functions and practice environment, must request and consider the opinions of other individuals from society in the definition of the practice environment.13
Within this framework in which the nursing professional identity must emerge, where retaking ideas by Dubar;14 identities at work do not derive mechanically from the 'situations' defined from outside as of objective criteria. (...) Above all, these identities depend on the relationships maintained with other players (bosses, colleagues, clients) of this 'work experienced'; that is, from a subjectively constructed and defined situation.
Nursing is a critical resource, which is why it is essential to know its image to contribute to consolidating its identity and consequently increase its number and place among healthcare professionals and society. Given that the professional image is a product of the interaction, it is necessary to inquire into different possible lines of interaction because each of them will force nurses into specific behaviors, referring to the role they must play in each particular situation, that is, as member of a work team, as a peer, or as a healthcare provider. For this reason, the study's general objective was to describe the nurse's professional image within distinct groups, healthcare professionals, and peers, which perform in different subsectors of the healthcare services system.
METHODOLOGY
Ours was a cross-sectional descriptive research, which is the second phase of a prior qualitative study.15 A probability sampling was carried out in which 12 of the 24 zones of the Greater Buenos Aires area (Argentina) were selected (Almirante Brown, Avellaneda, Berazategui, Florencio Varela, Hurlingham, José Clemente Paz, Lanús, Malvinas Argentinas, Moreno, Quilmes, Tigre, Vicente López). Thereafter, a sampling framework was constructed of healthcare institutions belonging to these zones based on the 2000 Guide of Healthcare Establishments elaborated by the Direction of Health Statistics and Information of the Nation's Ministry of Health, which has 4897 public and private healthcare institutions. The sampling framework was comprised by 1060 healthcare institutions. We excluded those specific institutions where we felt we would not find the population sought in its whole diversity from the private subsector (clinical analysis laboratories, diagnostic centers and institutes, dental centers), as well as the public sector (dispensaries, dental centers, specialized centers), leaving 230 private institutions and 373 public institutions. Stratification of institutions per zone was not conducted, given that the distribution of these institutions is not similar. A sample size was proposed of 12 public institutions and 12 private institutions. The sample size was based on reaching around 50% of the general hospitals of the zones selected, taking an equal number of health units and equipping the final number (12) with private institutions. Thus, a simple random drawing was conducted also obtaining possible replacements. Thereafter, contacts with the institutions were made to obtain the corresponding authorizations.
The sample of Hospitals was completed in its totality, but not so for the healthcare centers and private institutions where we had to resort to replacements and then contacts via the snowball technique to complete a sample size of subjects estimated in 100 per subpopulation of nurses, physicians, and other professionals. The final sample was comprised by 61.7% of subjects from the public subsector (6 hospitals and 6 healthcare centers) and by 38.3% from the private subsector (8 clinics and private companies). The data collection was conducted from March to November 2010. The final sample obtained was of 100 nurses (32.5%), 105 other professionals, and 103 physicians (33.4%).
With respect to the data collection instrument, questionnaires were made for each of the subpopulations containing multiple choice closed questions corresponding to each of the main categories found in a prior qualitative study15 (humanization of the link and transformation of oneself, motivation in selecting the career, working conditions, specific nursing functions, negative-positive relationship with patients, differences in ways of acting and working according to professional nursing categories, relations perceived of nursing with physicians and that of physicians with nursing, and relationships among peers in nursing). A pilot test was conducted of the questionnaires with 30 subjects from the three subpopulations until reaching the definite versions. The results were processed in the SPSS 17.0 program.
RESULTS
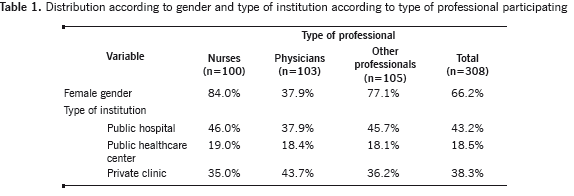
Table 1 shows that the female gender was the most frequent in the group of nurses (84.0%) and in the group of other professionals (77.1%) than in the group of physicians (37.9%), this difference was statistically significant (X2=56.77, p < 0.001). In the distribution per type of institution, the highest proportion of participants work in public hospitals (43.2%), followed by private clinics (38.3%) and healthcare centers (18.5%); without these differences being significant (X2 = 2.22, p = 0.69).
The proportion of positive responses to the questions, according to the study categories, can be seen in Table 2.
Humanization of the link and transformation of oneself. The three groups opted for the category understanding others better in higher proportion; rather, less than one in every three thinks of becoming more compassionate, with the lowest proportion being reported by nurses in this variable.
Motivation in choosing the career. For the three groups of professionals, the motives of personal fulfillment and service vocation appear in the first places. Statistically significant difference was found per type of professional for the variables possibility of rapid labor insertion (most important in nurses and other type of personnel), while curing had the third motive among physicians.
Working conditions. Wear is the predominant condition among the three groups of professionals with highest proportion among nurses. Regarding the other variables from this category, differences are noted in the first places: absenteeism is second among nurses and third among physicians and other professionals; while for helplessness due to lack of material resources, the previous situation is inverted. Optimism in the task appears in lower proportion among nurses; although, not so with conflicts in the work group.
Specific functions of nursing. The main specific nursing function, according to this trade group and the group of other types of professionals is to perform body care, while for physicians is for their therapeutic indications to be followed precisely. With respect to this last function, the difference of proportions per type of professional is statistically significant, with nurses having the lowest proportion of acceptance, with respect to the two other study groups.
Statistical significance was also found in the difference among the proportions of acceptance of the function of performing interventions without need of medical indication, where nurses had double the percentage estimated in physicians and other professions.
Relationship of nursing with patients. Nurses privilege their function de contention de patient demands, setting in second place their role of being a link between the physician and patient, a question in which physicians and the other professions occupy the first place. The three types of professionals coincided in the order of relationships, with the action of accompaniment taking third place, the fourth place was being translator of medical indications, and - lastly - contention of the patient's family demands.

Differences in ways of acting and working among the professions. Some 28.2% of the nurses, 3% of other professions, and 41.8% of the physicians perceive differences in ways of acting and working, this difference was not statistically significant (X2 = 5.02, p = 0.081).
Relationships between physicians and nurses. Important differences were observed between the groups. Nurses considered they have good and bad relations with physicians (51%), and perform team work with them (33%), although they do not value their capacities (26%). They think that nursing is only available to perform whatever physicians order (27%), and that some tasks requested have nothing to do with their profession (17.0%). In addition, they are not recognized in the specific nursing functions (16%). They accept to work in a team when it is clear that physicians are in charge (16%). One of every 10 nurses (16%) stated that physicians value them as peers. For their part, physicians also considered that they had good and bad relations with nursing (35.3%) and do team work (34.4%); but, rather, physicians do consider that they are recognized in the specific functions (32.4%) and that both professions work in the same direction (32.4%). Physicians recognize in nurses a good disposition for work (23.5%) and enthusiasm for learning and improving (21.6%); they also state that nurses do not always do what is indicated of them (21.6%) and that, to a lesser extent, they do not respect medical indications (14.7%).
Relations among peers in nursing. Nurses feel they are under heavy requirement because they are few (40.0%), they think they are exceeded because not everyone works equally (38.0%), and recognize conflicts among nurses (35.0%). The positive aspects in the relationships among nurses were enthusiasm for learning and improving (33.0%), good disposition to work among colleagues (28.0%), defending their position within the healthcare team (24.0%), and working in the same direction (23%).
DISCUSSION
The study of the professional image in nursing is central inasmuch as it involves a contribution to establishing its identity. The process of constructing this image turns out difficult, as evidenced, given that it is a theme of reiterated reflections.16,17
From the present study emerges that humanization of the involvement with the under their care continues being an important category for nursing, as found in the qualitative study. The main attribute within that category is better understanding others, but not necessarily involving a personal transformation (e.g., becoming more compassionate). It may be interpreted that the defense mechanisms against pain and anguish triggered by the disease of others is structured over time in healthcare professionals, as has been asserted,18 which diminishes the levels of empathy these professionals can manifest. This finding has been constantly expressed in literature in spite of the empathy that should be one of the characteristics present in the aid and care relations these healthcare professionals offer given that it is one of the factors that contribute to curing.19
In nurses, personal fulfillment and service vocation appear as important aspects that guide choosing a career at similar levels as the other healthcare professionals, but in their case rapid labor insertion also emerges as a weight factor. The precarious working conditions in nursing have been an issue of importance in several international investigations and reports, having been evaluated through objective indicators.1,20 The results of the current study warn how said precarious conditions present subjective aspects (perception by the nursing workers themselves with respect to wear in the task, helplessness due to lack of material resources, the task is not always done right, conflicts within the work group), which are most often experienced by nurses than by other healthcare professionals. Among the first, positive aspects of the task appear more relegated (good working climate and optimism). Discomfort in the professional group studied presents an important weight which deserves attention. The perception of the relations among peers in nursing again expresses that discomfort, given that they mostly appear upon feeling overly required and overwhelmed with tasks and soon after positive aspects emerge like enthusiasm for learning and improving or the good disposition for work.
One of the findings yielded by the qualitative study was a strong tension existing between physicians and nurses with respect to the functions and to the role prescribed by the medical model that differs from the model that defines nursing.15 This was again supported by the current study with consistent differences in the conceptions on the nursing functions conceived by nurses and physicians, manifested in that nurses place greater emphasis, for example, on the possibility of performing interventions without the need for medical indication and, conversely, physicians hold as the main nursing function that of following the physician's precise therapeutic indications. It is worth emphasizing that this last conception is shared by the other professionals.
This tension between conceptions is also reflected upon observing that nursing privileges in its relation with patients its function of contention of the patients, while physicians and other professionals privilege the function that they are a link between the physician and the patient. The place of the patient's family is relegated to a last term among all the healthcare professionals, evidencing the individualist conception of the medical model. Likewise, the model's biologist bias appears clearly in the three subpopulations assigning primacy to caring for the body.
Upon bearing in mind the perceived relations of nursing with physicians, again contradicting perceptions emerge: nurses consider that physicians do not value their capacities; that they are available to do what they order; or that they do not recognize their specific functions; and to a lesser extent that they are valued as peers. In contradistinction, physicians do consider that they recognize their specific functions and that they have good disposition for work, and that good enthusiasm exists for learning and improving. Then, the aspect appears that they don't always do what is indicated of them and, in a lower proportion, that they do not respect medical indications. These results again show contradicting views on how the relations are perceived, which surely leads to conflicting interactions within the healthcare team.
Regarding the image we have of a profession, Leibovich de Figueroa and Schufer de Paikin21 consider that it is conditioned by behaviors and expectations facing it, both for lay people and professionals. Image and identity appear intimately related. At this point, it is worth returning to that indicated by Dubar14 with respect to identity strategies, which would result from the articulation of objective and subjective transactions. The objective transactions would be on the relational axis; the subjective transactions concern the transactions from the subject's internal world, crossed by the conflict between inherited identities and purported identities.
Ramírez,22:28 retaking Dubar, states that identity is an articulation of these two heterogeneous identity processes, each of us is identified by another, this identification is based on social categories legitimized in two different levels: the first, called actions of attribution that define the type of individual you are, that is, the identity given by another (virtual identity); the second, are membership actions, which express the type of individual you want to be, that is, identity for oneself (real identity). This articulation is understood by Dubar14 as a negotiation between identity claimants and identity offers to propose. This identity negotiation constitutes a complex communicative process; it is not an authoritarian process of predefined identity labeling. In nursing, the need to construct a professional image appears linked to a professional identity and to the individual identity within a conflictive space and not always clearly defined within a field of social interaction where the monopoly is precisely held by the medical profession from a social consensus. Because of what has been exposed, it is not strange that the tension and contraposition found emerge, deriving into difficulties associated to the construction of the image and identity; making this scenario visible, permits working to consolidate that identity.
REFERENCES
1. Organización Panamericana de la Salud-Organización Mundial de la Salud. Enfermería en la Región de las Américas. Washington: OPS-OMS; 1999. Publicación Científica No. 571. [ Links ]
2. Organización Mundial de la Salud. Organización Panamericana de la Salud. Formar para Transformar. Experiencia estratégica de profesionalización de auxiliares de enfermería en Argentina. 1990 - 2000. Washington: OPS-OMS; 2002. Publicación Científica N° 54. [ Links ]
3. Pan American Health Organization. Nursing and midwifery services contributing to equity, access, coverage, quality, and sustainability in the health services. Mid Term Plan 2002-2005. Washington: PAHO; 2002. [ Links ]
4. Pérez A, Alameda A, Albéniz C. La formación práctica en enfermería en la Escuela Universitaria de Enfermería de la Comunidad de Madrid. Opinión de los alumnos y de los profesionales asistenciales. Un estudio cualitativo con grupos de discusión. Rev Esp Salud Pública. 2002;76 (5):517-30. [ Links ]
5. Bartels JE. Creating meaningful accreditation practices for the next millenium. J Prof Nurs. 1997; 13(3):140. [ Links ]
6. Gomes AM, Oliveira DC. A auto e heteroimagem profissional do enfermeiro em saúde pública: um estudo de representações sociais. Rev Latino-Am. Enfermagem. 2005;13(6):1011-8. [ Links ]
7. Lawrence J, Wearing A, Dodds A. Nurse's representations of the positive and negative features of nursing. J Adv Nurs. 1996; 24(1):375-84 [ Links ]
8. Netto LFSA, Ramos FRS. Consideraciones finales sobre el proceso de construcción de la identidad del enfermero en el trabajo cotidiano. Rev Latino-Am Enfermagem. 2004; 12(1) 50-7. [ Links ]
9. Wainerman C, Binstock GP. Ocupación y Género. Mujeres y varones en enfermería. Buenos Aires: Centro de Estudios de Población (CENEP);1993. Cuaderno Nro 48. [ Links ]
10. Torres Esperón, J. M. (2004). Reflexiones sobre funciones del personal de enfermería. Rev Cubana Salud Pública [Internet]. 2004 (Cited 2010 Jul 15); 30 (4). Available from: http://bvs.sld.cu/revistas/spu/vol30_4_04/spu09404.htm [ Links ]
11. Carr AM, Wilson PA. The professions. Oxford: Clarendon Press; 1933. P. 284 [ Links ]
12. Real MA. Sociología de la profesión de Graduado Social. [Dissertation]. Alicante: Facultad de Ciencias Económicas y Empresariales, Universidad de Alicante; 2002. [ Links ]
13. Madden-Syles M, Affara FA. El Consejo Internacional de Enfermeras y la reglamentación: modelos para el siglo XXI. Ginebra: CIE; P. 21-4. [ Links ]
14. Dubar C. El trabajo y las identidades personales y profesionales. Rev Latinoam Estud Trab. 2001; 7(13):5-16. [ Links ]
15. Samaniego VC, Cárcamo S, Frankel D. La imagen profesional de enfermería en su contexto de trabajo. Hologramática. 2011; 7(14):59-92. [ Links ]
16. Maya MC. Identidad profesional. Invest Educ Enferm. 2003; 21(1):98-104. [ Links ]
17. Irigibel X. Enfermería disciplinada, poder pastoral y racionalidad medicalizadora. Index Enferm. 2008; 17(4):276-9 [ Links ]
18. Benbunan-Bentata Bm, Cruz-Quintana F, Roa-Venegas JM, Villaverde-Gutiérrez C, Benbunan-Bentata BR. Afrontamiento del dolor y la muerte en estudiantes de Enfermería: una propuesta de intervención. Int J Clin Health Psychol. 2007; 7 (1):197-205. [ Links ]
19. Reynolds W J, Scott B. Do nurses and other professional helpers normally display much empathy? J Adv Nurs. 2002; 31:226-34. [ Links ]
20. Guevara E, Mendias E. A comparative analysis of the changes in nursing practice related to health sector reform in five countries of the Americas. Pan Am J Public Health. 2002; 12(5):347-53. [ Links ]
21. Leibovich de Figueroa N, Schufer de Paikin M. Imagen profesional del psicólogo clínico. BAP. 1992; 5(1):9-11. [ Links ]
22. Ramírez V. La construcción de la identidad profesional de las normalistas tlaxcaltecas.Un estudio sobre los imaginarios y los procesos sociodiscursivos que definen el ser maestra en dos contextos culturalmente diferenciados: la Normal Urbana 'Lic. Emilio Sánchez Piedras' y la Normal Rural 'Lic. Benito Juárez'. [Dissertation]. México DF.: Universidad Autónoma Metropolitana; 2008. [ Links ]
