










Services on Demand
Journal
Article
 text in
text in  English (pdf)
English (pdf)
 Article in xml format
Article in xml format Article references
Article references
 Send this article by e-mail
Send this article by e-mailIndicators
-
 Cited by SciELO
Cited by SciELO -
 Access statistics
Access statistics
Related links
-
 Cited by Google
Cited by Google -
 Similars in
SciELO
Similars in
SciELO -
 Similars in Google
Similars in Google
Share

 Permalink
PermalinkInvestigación y Educación en Enfermería
Print version ISSN 0120-5307
Invest. educ. enferm vol.31 no.3 Medellín Sept./Dec. 2013
ARTÍCULO ORIGINAL / ORIGINAL ARTICLE/ ARTIGO ORIGINAL
Stress in mastectomized women
Estrés en mujeres mastectomizadas
Estresse em mulheres mastectomizadas
Candida Canicali Primo1; Maria Helena Costa Amorim2; Denise Silveira de Castro3; Thais Cordeiro Paraguassú4; Tonyara Patricia Nogueira5; Georgia Bianca Martins Bertolani6; Franciele Marabotti Costa Leite7
1RN, Master. Professor Universidade Federal do Espírito Santo UFES, Vitória (ES), Brazil. email: candidaprimo@gmail.com.
2RN, Ph.D. Professor UFES, Vitória (ES), Brazil. email: mailto:mhcamorim@yahoo.com.br.
3RN, Ph.D. Professor UFES, Vitória (ES), Brazil. email: dsmcastro@terra.com.br.
4RN. UFES, Vitória (ES), Brazil. email: thais_paraguassu@hotmail.com.
5RN. UFES, Vitória (ES), Brazil. email: tonyara_nogueira@hotmail.com.
6Psychologist, Mestre. Professora UFES, Vitória (ES), Brazil. email: geobianca@hotmail.com.
7RN, Master. Professor UFES, Vitória (ES), Brazil. email: emaildafran@ig.com.br.
Receipt date: Oct 8, 2012. Approval date: May 8, 2013.
Subventions: none.
Conflicts of interest: none.
How to cite this article: How to cite this article: Primo CC, Amorim MHC, Castro DS, Paraguassú TC, Nogueira TP, Bertolani GBM, Leite FMC. Stress in mastectomized women. Invest Educ Enferm. 2013;31(3): 385-394.
ABSTRACT
Objective. To evaluate the stress level in women who have had mastectomy and analyze the relationship between stress and sociodemographic, clinical, and social support variables. Methodology. Descriptive study carried out at Hospital de Santa Rita de Cássia, Vitória/Espírito Santo (Brazil) among 84 mastectomized women. We used a questionnaire to elicit sociodemographic information and instruments to evaluate stress (Lipp's Stress Symptom Inventory for Adults) and anxiety (State-Trait Anxiety Inventory]). Results. A total of 69% of women had stress. Stress in the exhaustion phase was found in 57% of women, the resistance phase in 39%, alarm in 2%, and the near-exhaustion phase in 2%. Physical symptoms predominated (56%) over psychological symptoms (44%). Only 25% of participants had some type of social support. Of investigated variables, only the relationship of stress with anxiety traits was statistically significant. Conclusion. An important proportion of mastectomized women experienced stress. Nursing follow-up is essential to help these patients deal with the stress associated with breast cancer.
Key words: breast neoplasms; mastectomy; stress, psychological; anxiety.
RESUMEN
Objetivo. Evaluar el nivel de estrés en mujeres mastectomizadas y examinar la relación del mismo con variables sociodemográficas, clínicas y de apoyo social. Metodología. Estudio descriptivo realizado en el hospital de Santa Rita de Cássia en Vitória/Espírito Santo (Brasil), con una muestra de 84 mujeres mastectomizadas. Se utilizó un formulario que contenía información sociodemográfica e instrumentos para la evaluación del estrés (Inventario de Síntomas de Estrés de Lipp) y de la ansiedad (Inventário de Ansiedade Traço e Estado - IDATE-). Resultados. Del total de mujeres estudiadas, un 69% presentó estrés. De estas, el 57% se encontraba en las fases de agotamiento; el 39%, en la de resistencia; el 2%, en alerta, y otro 2% en casi agotamiento; los síntomas físicos (56%) predominaron sobre los psicológicos (44%). Tan solo el 25% de las participantes recibía algún tipo de apoyo social. De las variables investigadas, tan solo la relación de estrés con rasgos de ansiedad presentó asociación estadísticamente significativa. Conclusión. Una proporción importante de las mujeres mastectomizadas sufre de estrés. Es esencial el acompañamiento de enfermería a estas pacientes que conduzca a afrontar mucho mejor esta enfermedad.
Palabras clave: neoplasias de mama; mastectomia; estrés psicológico; ansiedad.
RESUMO
Objetivo. Avaliar o nível de estresse em mulheres mastectomizadas e examinar a relação do mesmo com variáveis sócio-demográficas, clínicas e de apoio social. Metodologia. Estudo descritivo realizado no hospital de Santa Rita de Cássia em Vitória/Espírito Santo (Brasil), com uma mostra de 84 mulheres mastectomizadas. Utilizou-se um formulário que continha informação sócio-demográfica e instrumentos para a avaliação do estresse (Inventário de Sintomas de Estresse de Lipp) e da ansiedade (Inventário de Ansiedade Traço e Estado - IDATE-). Resultados. Do total de mulheres estudadas, um 69% apresentou estresse. Destas, o 57% se encontrava nas fases de esgotamento; o 39%, na de resistência; o 2%, em alerta, e outro 2% em quase esgotamento; os sintomas físicos (56%) predominaram sobre os psicológicos (44%). Tão só o 25% das participantes recebia algum tipo de apoio social. Das variáveis pesquisadas, tão só a relação de estresse com rasgos de ansiedade apresentou associação estatisticamente significativa. Conclusão. Uma proporção importante das mulheres mastectomizadas sofre de estresse. É essencial o acompanhamento da enfermagem a estas pacientes que conduza a enfrentar muito melhor esta doença.
Palavras chaves: neoplasias da mama; mastectomia; estresse psicológico; ansiedade.
INTRODUCTION
Breast cancer is the most common neoplasia among women and the second most frequent overall worldwide. It is estimated that each year around 22% of new cases of cancer in women occur in the breast. In Brazil in 2012, about 52,860 new cases of breast cancer were expected, with an estimated risk of 52 cases/100 000 women. In the city of Espirito Santo, the estimate is 900 new cases of breast cancer with an incidence of 49.42 cases/100,000 women. For the city capital, Vitória, the expected incidence was 71.28 cases/100 000 women.1
A breast cancer diagnosis changes a woman's life and represents an emotional load that could trigger emotional-affective imbalances, such as depression, anxiety, or even psychosis; it could also generate stress in some patients.2 The term ''stress'' as a health concept was introduced in 1936 by Hans Selye. This author defines stress as an organism's nonspecific organic response to stressful situations.3 In 2001, other researchers4 defined stress as an organism's adaptive reaction to situations that require great emotional effort to be overcome (i.e., stressful situations).
Stress has three phases: alarm, resistance, and exhaustion. The alarm phase is considered a positive phase of stress; during this phase humans are energized by adrenaline production, survival is preserved, and feelings of plenitude are often experienced. In the resistance phase, the person automatically attempts to deal with stressors in a way that maintains internal homeostasis. If stressful factors persist in frequency and intensity, resistance is broken and the person moves on to the exhaustion phase. In this phase severe diseases could occur in more vulnerable organs, such as heart failure, ulcers, psoriasis, and depression.3
Although stress has been classified into three phases, researchers have identified and shown both clinically and statistically a new phase of stress process called near-exhaustion. The term has been so named because it is between resistance and exhaustion and is characterized by weakness in a person who is not able to adapt himself/herself to or resist the stressor. Diseases begin to appear, but they are not as severe as those seen in the exhaustion phase. Moreover, the person can work and function in society until a specific point, different from that which occurs in the exhaustion phase, when the individual stops ''functioning'' appropriately and is unable to work or concentrate.5
Over the long term, the stress, along with genetic predisposing factors, leads to vulnerability to depression and anxiety disorders. This situation can be even more acute in women; several sources indicate that women experience more stress than men.6,7 Researchers have been evaluating depression, anxiety, and somatic symptoms as indications of inadequate adjustment to stressful events because depression and anxiety are symptoms of stress. A woman diagnosed with breast cancer experiences a number of stressors that affect her at different phases of the disease.8-10 Thus, follow-up and treatment for not only cancer but also the causes of stress are essential. Evaluating stress in patients who have undergone mastectomy is important for identifying those at high risk for developing psychopathologic disorders while receiving treatment, and also contributing for management of nursing care delivered for these women. In this sense, our aim was to evaluate stress in mastectomized women and analyze the relationship of stress with sociodemographic, clinical and social support variables.
METHODOLOGY
This is a descriptive study of a qualitative approach performed in the Rehabilitation Program for Mastectomized Women (PREMMA; acronym in Brazilian Portuguese) located in the Ylza Bianco outpatient unit at Hospital Santa Rita de Cássia (HSRC) of Women's Association for Cancer Education and Control (AFECC; acronym in Brazilian Portuguese), which offers high-complexity oncology car in Vitória/Espírito Santo, Brazil.
The PREMMA was founded in partnership with the Nursing Department of Universidade Federal do Espírito Santo and the AFECC-HSRC with the goal of systematizing interdisciplinary care for mastectomized women that is based on the specific skills of each area of health knowledge. The patients seen at this clinic consisted of women who had undergone mastectomy and were referred to health professionals of HSRC, mainly from Espírito Santo State. After their clinical diagnosis, the women were included in the integral care process and engaged in several activities designed to help them reenter the work environment and thereby recover their self-esteem.
The study sample was composed of 84 mastectomized women enrolled in PREMMA. Inclusion criteria were women older than 20 years of age diagnosed with breast cancer without distant metastasis that underwent surgery and had no personal history of psychiatric disease or use of illicit drugs. Women were enrolled after providing written informed consent.
Information on the following variables was collected: socioeconomic data (age, marital status, formal education, occupation, contribution for Social Security, family income); clinical data (hospital where surgery was conducted, type of surgery, date of enrollment at PREMMA), and social support (support given by partner and family or friends). This information was obtained by interviewing the patients and recording their responses on a standardized form. Clinical information concerning date of surgery, date of PREMMA enrollment, and frequency of visits to PREMMA was collected from an active search of medical records and enrollment service files.
Economic class variables were identified using a formulary of economic classification of the Brazilian Association of Research Companies. Brazilian economy classification is obtained using an economic segmentation instrument that involves a home characteristics survey (presence and number of some comforting home items and formal education degree of head of the family) to differentiate the population. The levels of economic classification are defined by letters A, B, C, D, E.11
To assess stress, Lipp's Stress Symptoms Inventory for Adults (LSSI) was used. The instrument was validated in Brazil in 1994 and evaluates whether an individual has experienced stress and, if so, the stress phase according to physical or psychological symptoms. The LSSI identifies the three stress phases described above: alarm, resistance, and exhaustion. The LSSI has a total of 34 items regarding somatic symptoms and 19 for psychological symptoms; several symptoms are repeated several times and differ only by intensity and severity. The person is evaluated according to physical or psychological symptoms experienced in the last 24 hours, last week, and last month. The new phase proposed by Lipp during evaluation of the present instrument -- the near-exhaustion phase -- is identified by the frequency of items marked for the resistance phase. The instrument was analyzed by a psychologist and in research based on Lipp's recommendations.12
Variable trait and anxiety status were measured to evaluate the relationship between stress and anxiety by using the State Trait Anxiety Inventory (STAI). This inventory consists of two parts, with 20 affirmations each. The anxiety trait evaluates how often women perceived their own life, and the anxiety status evaluates anxiety in the moment of the interview.10 Data were collected through individual interviews from December 2009 to March 2010. For statistical analysis, SPSS software, version 15.0 (SPSS Inc, Chicago, Illinois), was used. We performed a descriptive analysis using frequency tables and graphics. To analyze the relationship between variables and stress, we applied the chi-square test. A ρ value <0.05 indicates the existence of a relation among variables.
This research project was approved by the Ethical and Research Committee of the Health Science Center at Universidade Federal do Espírito Santos (number 225/2009). After the end of the study patients received a letter containing the results achieved. Patients who presented with stress in the exhaustion and near-exhaustion phases were referred to our institution's psychological service.
RESULTS
After application and interpretation of data from ISSL, we found that 69% of patients met criteria for stress and 31.0% did not. Among all patients, 56.9% were at the exhaustion stress phase, 39.7% were at the resistance phase, 1.7% were at the alarm phase, and 1.7% were at the near-exhaustion phase. Of the women who were experiencing stress, 56.2% had physical symptoms and 43.7% had psychological symptoms. Among women in the exhaustion phase, more had developed psychological symptoms (59.0%) than physical symptoms (41.0%). As shown in Table 1, the most frequent symptoms were distress/daily anxiety, nervousness, excessive tiredness, thinking/speaking about a single subject, and eagerness to run away from everything. Fifty-eight percent of women in the resistance phase presented physical symptoms; the most frequent were lack of memory, constant physical fatigue, and constant tiredness.
Table 1. Characterization of the predominant symptoms among 84 women with exhaustion- and resistance-phase stress, Vitória/ES, December 2009 - March 2010
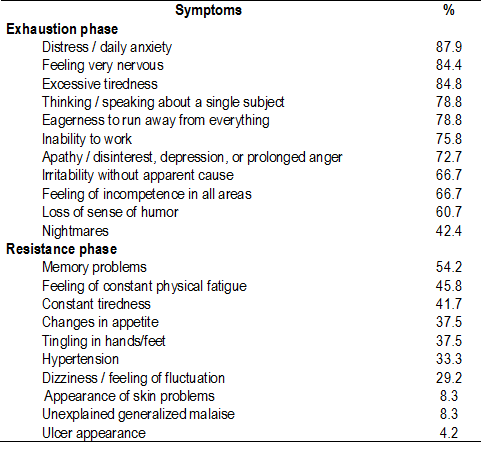
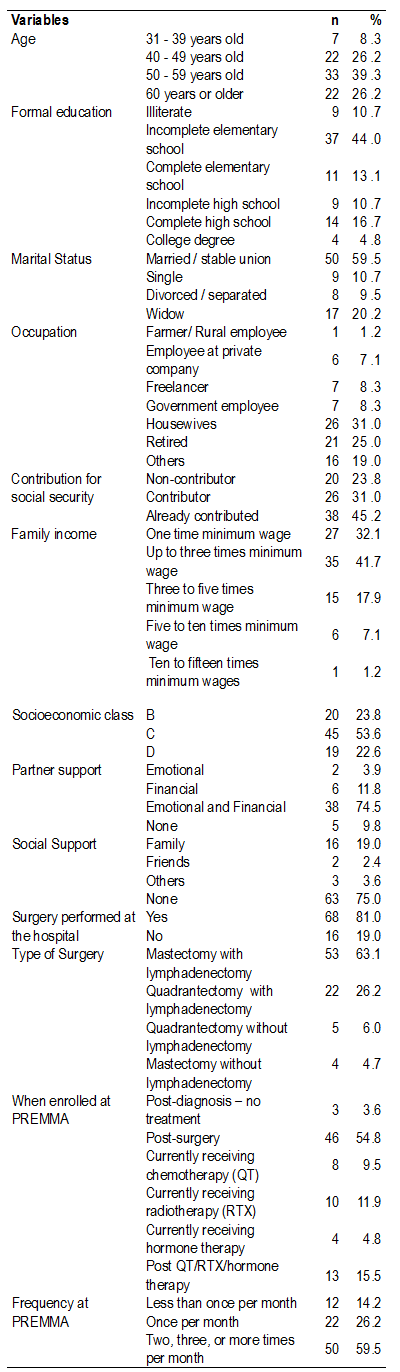
Table 2 describes sociodemographic, clinical, and social support variables. Ages ranged from 31 to 80 years; the mean age was 45.5 years. In addition, 39.3% of these women were 50 to 59 years of age, 59.5% were married, and 44% had an incomplete elementary school education.
Thirty-one percent of women were housewives and 25% were retired; 45.2% had contributed to Social Security and 31.0% were active contributors. Women with family income was one to three times minimum wage, and of these women 53.6% were from socioeconomic class C.
Of the 50 women who had a partner, 74.5% received emotional or financial support from the partner. However, 75% of women did not receive any type of social support. Eighty-one percent of women underwent the surgery at the hospital where the study was conducted; 63.1% underwent mastectomy with lymphadenectomy, 54.8% were enrolled at PREMMA after surgery, and 59.5% frequented PREMMA three or more times a month.
The chi-square test showed no associations between stress and the following variables: age, marital status, formal education, occupation, contribution to Social Security, family income, socioeconomic class, partner support, social support, hospital where the surgery was performed, type of surgery, date of enrollment at PREMMA, and anxiety status. On the other hand, stress and anxiety trait showed a significant relationship (ρ= 0.013).
Table 2. Socioeconomic and clinical variables among 84 women, Vitória/ES, December 2009 - March 2010
DISCUSSION
This study found most of the study participants met the criteria for stress. Patients who have cancer or are facing the possibility of a malignant tumor become desperate, distressed, fearful, hopeless, sad, and nervous. 13
A study conducted to delineate possible relationships between emotional reactions to breast cancer and psychological morbidity in mastectomized women evaluated stress in 10 patients and reported that 80% of participants were stressed.9 Another investigation evaluated the presence of stress in 16 women after treatment for breast cancer and found that 37.5% experienced stress.14 These findings reflect the hopelessness that women undergoing mastectomy feel as a result of breast removal; their diagnosis, the procedure, and the potential side effects involved affect their emotions and self-image.13
The scarcity of studies comparing stress and breast cancer limit our ability to compare our results with the literature; in addition, most existing studies considered stress as a causal factor for cancer rather than stress as a process of adaptation to cancer and related issues. Moreover, the previous studies we identified included small samples.
Some studies that included women with psychological imbalance after breast cancer treatment report that it affects 5% to 50% of women. They also affirm that women with a psychiatric history and had low expectations of treatment benefits (due to their lack of support or previous experience with family members) have higher risk for developing psychological imbalance.15,16
Most of the women in our study with stress had a higher frequency of physical symptoms than psychological symptoms. The most frequent stress phase was exhaustion, followed by resistance. Among women in the exhaustion phase, psychological symptoms were prevalent, particularly the following symptoms: daily distress/anxiety, nervousness, excessive fatigue, thinking/speaking about a specific subject, and eagerness to run away from everything. In this phase, people experience excess of activities and high consumption of energy, and are more susceptible to any organic diseases that might appear.3
In the resistance phase physical symptom predominate, particularly memory problems, feelings of constant physical fatigue, and constant tiredness. Women in this phase were trying to deal with stress, for which they were seeking homeostasis. Soon, these women could become vulnerable to infections and diseases as a result of cortical suprarenal hyperactivity and high consumption of energy.5
A study of stress in women who had mastectomy, performed in Minas Gerais, verified the prominence of psychological symptoms in the resistance phase, followed by the near-exhaustion phase.9 In São Paulo, a study that evaluated the presence of stress in women after breast cancer treatment verified that 100% of stressed patients were at the resistance phase and had more psychological symptoms than physical symptoms.14
A study of stress and social ability in patients with laryngeal cancer found that most presented with stress at any phase; the resistance phase was most common, followed by the exhaustion phase. No patients were at the alarm or near-exhaustion phase. Almost all patients had psychological symptoms. The most common psychological symptoms of stress were self-doubt, thinking constantly about a specific subject, and excessive tiredness.8
A study of mastectomized women showed that during treatment with tamoxifen, patients's stress level increased; the most-reported stress symptoms were distress, insomnia, back pain, and thoughts that provoked anxiety.10 An investigation on the stress of labor magistrates found that most of the sample had symptoms typically found in stress, primary during the resistance phase. This population reported feeling constant physical fatigue, suffered from muscle tension, and experienced excessive irritability; these physical symptoms occurred more often than psychological symptoms, results that agree with our findings.6
An important result found in our study was the significant association of stress and anxiety trait. Thus, it is reasonable to ask whether stress is related to intrinsic characteristics of the patients - not only aspects associated with the disease itself and its consequences but also history and life habits, because the study instrument determined how women normally felt about their life. Stress situations that last for a long time result in body imbalance; for this reason, the defense mechanism against cancer become weak from exhaustion. Therefore, an important point is how to strengthen defense mechanisms against cancer and increase defense efficacy after appearance of a malignant tumor; the defense is necessary to improve life satisfaction, hopefulness about survival, and the ability to resist and self-heal from cancer.17
By using an analysis of variable frequency, we found that most patients went to PREMMA three or more times a month. This regular attendance might be explained by the patients' need for a place where they can speak freely about their doubts, uncertainty, and distress and the effects on their daily activities. Considering the age of women included in this study, we observed similar findings in a study of 170 patients with breast cancer in London; the mean age in that study was 48.4 years, similar to that in ours.18 Several studies conducted in Vitória/ES also reported that most patients were of this age.14,19-21
In our study, most women were married and had limited formal education. Similar results were seen in other studies of mastectomized women19-21 conducted in Espirito Santo. The family income in our study was similar to that reported in other research22 among patients with breast cancer, which reported a total of no more than three times minimum wages. Other studies21 carried out in Vitória with mastectomized women showed that most of them had family income up to 3 minimal wages.
A study in Paraná23 that analyzed the socioeconomic profile of women undergoing treatment of breast cancer found that most women belonged to socioeconomic class C, a finding that corroborates the result in the present study. The same study from Paraná23 showed results similar to ours in relation to the women' s occupation: Most of the interviewed women were housewives, and a minority were retired.
Concerning Social Security, a study in post-mastectomy women agrees with results found in our study. 21 An earlier study reported that around 44% of women treated for breast cancer received emotional and financial support from their partners,24 which also corroborates our results. In addition, a study of mastectomized women conducted in Campinas showed the importance of support to women with breast cancer; women who have a partner present better scores on psychological and social relations domains. Presence of a partner may indicate that women have a greater chance of receiving social and psychological support and having better living conditions.25
Our study results concerning social support agree with those observed in women diagnosed and treated for breast cancer at a teaching hospital; at that hospital, most women seek and receive social and family support through relatives and friends, but support is not always provided by all.24
In our study, most women underwent surgery in the same hospital where this study was conducted. This fact probably explains why women were referred to PREMMA after breast cancer diagnosis; this did not occur when treatment was carried out at different hospital. A previous study found that most women with breast cancer underwent conservative treatment, a finding that differs from the situation in our study.19
It is important to analyze the point at which women in our study enrolled in PREMMA. We observed that the evaluation effects of PREMMA implementation, such as nursing intervention before surgery among women diagnosed with breast cancer, showed that those enrolled in PREMMA before surgery had a low level of anxiety compared with those who enrolled after the surgery.25 Enrolling in PREMMA before mastectomy benefited the patient psychologically. Although the program was initially created with the goal to perform postoperative interventions, the results of this study led the rearrangement of the referral flowchart for women just after diagnosis. It is believed that the results of this study have led to early referral to PREMMA for some women. It is critical that nurses incorporate into their daily practice the use of instruments that allow them to identify normal stress behavior. Doing so could facilitate and support nursing interventions.13
Our study suggests that most of patients fulfilled all stress criteria. Stress was not significantly related to most variables, but the association of stress with trait variables of anxiety was significant. We found that breast cancer could generate stress events. Thus, applying the instrument used in this study during interdisciplinary care for women with cancer can help evaluate stress more frequently and identify patients who need psychological support.
We emphasize the importance of interdisciplinary and holistic care delivery to mastectomized women, with the goal of reducing the effect of stress from cancer, improving the way patients face problems, and, consequently, improving their response to emotional stress.
Further studies on stress in women with breast cancer that feature larger samples are recommended to enable extrapolation of the results and increase the validity of our conclusions. In addition, future research on the relationship between stress and previous life activities may help elucidate cancer genesis.
REFERENCES
1. Ministério da Saúde (BR). Secretaria de Atenção à saúde. Instituto Nacional do Câncer. Coordenação de prevenção e vigilância de câncer. Estimativas 2010: incidência de Câncer no Brasil [Internet]. Rio de Janeiro; 2010 (cited 2012 Dec 9). Available from: http://www.inca.gov.br/estimativa/2010 [ Links ]
2.Cantinelli FS, Camacho RS, Smaletz O, Gonsales BK, Braguittoni É, Rennó JA. Oncopsiquiatria no câncer de mama: considerações e respeito de questões do feminino. Rev Psiquiatr Clín. 2006; 33(3):124-33. [ Links ]
3. Selye H. The stress of life. New York: Mc Graw Hill; 1956. [ Links ]
4. Lipp MEN, Malagris LEN. O stress emocional e seu tratamento.In: Rangé B. Pisicoterapias cognitivo-comportamentais: um diálogo com a Psiquiatria. 2nd Ed. Porto Alegre: Artméd; 2001. P. 475-90. [ Links ]
5. Lipp MEN. O modelo quadrifásico do stress. In: Lipp MEN. (Editors). Mecanismos neuropsicofisiológicos do stress: teorias e aplicações clínicas. São Paulo: Casa do psicólogo; 2003. [ Links ]
6. Lipp MEN, Tanganelli MS. Stress e Qualidade de Vida em Magistrados da Justiça do Trabalho. Psicol Reflex Crít. 2002; 15(3):537-48. [ Links ]
7. Ferreira LRC, Martino MMF. Stress no cotidiano da equipe de enfermagem e sua correlação com o cronótipo. Estud Psicol. 2009; 26(1):65-72. [ Links ]
8. Calais SL, Andrade LMB, Lipp MEN. Diferenças de Sexo e Escolaridade na Manifestação de Stress em Adultos Jovens. Psicol Reflex Crít. 2003; 16(2):257-63. [ Links ]
9. Grun, TB. Stress e habilidades sociais em pacientes com câncer de laringe [Dissertation]. Campinas: Pontifícia Universidade Católica de Campinas - Mestrado em Psicologia do Centro de Ciências da Vida; 2009. [ Links ]
10. Olympio PCAP. Níveis de imunoglobulina A salivar, ansiedade, estresse e depressão de mulheres mastectomizadas em uso de tamoxifeno [Dissertation]. Vitória: Universidade Federal do Espírito Santo - Mestrado em Saúde Coletiva; 2008. [ Links ]
11. ABEP - Associação Brasileira de Empresas de Pesquisa. Critério de Classificação Econômica Brasil, 2010. Disponível em: < http://www.abep.org> [ Links ].
12. Lipp MEN. Manual do Inventário de Stress para adultos de LIPP. São Paulo: Casa do Psicólogo; 2000. [ Links ]
13. Amorim MHC. A enfermagem e a psiconeuroimunologia no câncer de mama [Dissertation]. Rio de Janeiro: Universidade Federal do Rio de Janeiro - Escola de Enfermagem Ana Nery; 1999. [ Links ]
14. Silva G. Processo de enfrentamento no período pós-tratamento do câncer de mama [Dissertation]. Ribeirão Preto: Universidade de São Paulo - Mestrado em Psicologia; 2005. [ Links ]
15. Griffin IS, Fentiman M. Psychosocial problems following a diagnosis of breast câncer. Int J Clin Pract. 2002; 56(9):672-5. [ Links ]
16. Thewes B, Butow P, Pendlesbury S. The psychosocial needs of breast cancer survivors: a qualitative study of shared and unique needs of younger versus older survivors. Psycho Oncol. 2004; 13(3):177-89. [ Links ]
17. LeShan L. O câncer como ponto de mutação: um manual para pessoas com câncer, seus familiares e profissionais de saúde [Traduction: Bolanho D] São Paulo: Summus Editorial; 1992. [ Links ]
18. Burguess C, Cornelius V, Love S, Graham J, Richards M, Ramirez A. Depression and anxiety in women with early breast cancer: five year observational cohort study. BMJ. 2005; 330(7493): 702-5. [ Links ]
19. Leite FMC, Bubach S, Amorim MHC, Castro DS, Caniçali CP. Mulheres com diagnóstico de câncer de mama em tratamento com tamoxifeno: perfil sociodemográfico e clínico. Rev Bras Cancerol. 2011; 57(1):15-21. [ Links ]
20. Caniçali RA, Figueiredo GB. A inserção de mulheres com diagnóstico de câncer de mama em um programa de reabilitação. Vitória: Universidade Federal do Espírito Santo, Curso de Enfermagem, Departamento de Enfermagem; 2006. [ Links ]
21. Mai Junior AAM, Pereira JR. Depressão em mulheres mastectomizadas. Vitória: Universidade Federal do Espírito Santo, Curso de Enfermagem, Departamento de Enfermagem; 2009. [ Links ]
22. Souza FGM, Ribeiro RA, Silva MSB, Ivo PSA, Lima Jr. VS. Depressão e ansiedade em pacientes com câncer de mama. Rev de Psiquiatr Clín. 2000; 27(4): 207-14. [ Links ]
23. Campana HCR. Perfil de mulheres com câncer de mama [Dissertation]. Maringá: Universidade Estadual de Maringá - Mestrado em Enfermagem; 2007. [ Links ]
24. Sales CACC, Scandiuzz LPD, Anjos, ACY. Qualidade de vida de mulheres tratadas de câncer de mama: Funcionamento Social. Rev Bras de Cancerol. 2001; 47(3):263-72. [ Links ]
25. Huguet PR, Morais SSS, Osis MJD, Pinto-Neto AM, Gurge MSC. Qualidade de vida e sexualidade de mulheres tratadas de câncer de mama. Rev Bras Ginecol Obstet. 2009; 31(2):61-7. [ Links ]
