










Services on Demand
Journal
Article
 text in
text in  English (pdf)
English (pdf)
 Article in xml format
Article in xml format Article references
Article references
 Send this article by e-mail
Send this article by e-mailIndicators
-
 Cited by SciELO
Cited by SciELO -
 Access statistics
Access statistics
Related links
-
 Cited by Google
Cited by Google -
 Similars in
SciELO
Similars in
SciELO -
 Similars in Google
Similars in Google
Share

 Permalink
PermalinkInvestigación y Educación en Enfermería
Print version ISSN 0120-5307
Invest. educ. enferm vol.32 no.1 Medellín Jan./Apr. 2014
ARTÍCULO ORIGINAL / ORIGINAL ARTICLE / ARTIGO ORIGINAL
Perception of quality of life of a group of individuals subjected to bariatric surgery
Percepción de calidad de vida de un grupo de personas operadas de cirugía bariátrica
Percepção de qualidade de vida de um grupo de pessoas operadas de cirurgia bariátrica
Ángela María Salazar-Maya1; Teresa Nury Hoyos-Duque2; Lucas Bojanini-Acevedo3
1RN, Ph.D. Professor, Universidad de Antioquia, UdeA. Calle 64 #53-09, Medellín; Colombia. email: amsalazar@udea.edu.co.
2RN, Master. Professor, Universidad de Antioquia, UdeA. Calle 64 #53-09, Medellín; Colombia. email: nuryhoyos@udea.edu.co.
3Bariatric surgeon. Member of Comité Consultor de Cirugía Bariátrica de la Sociedad Colombiana de Cirugía. email: lucas.bojanini@gmail.com.
Receipt date: Jul 23, 2013. Approval date: Oct 7, 2013.
Article linked to research: Estado de salud y calidad de vida de las personas sometidas a cirugía bariátrica.
Subventions: Facultad de Enfermería de la Universidad de Antioquia y Grupo de Investigación La Práctica de Enfermería en el Contexto Social.
Conflicts of interest: none.
How to cite this article: Salazar-Maya AM, Hoyos-Duque TN,Bojanini-Acevedo L. Perception of quality of life of a group of individuals subjected to bariatric surgery. Invest Educ Enferm. 2014;32(1): 22-32.
ABSTRACT
Objective. The study sought to identify the state of health and quality of life of post-bariatric surgery patients. Methodology. This was a cross-sectional study conducted in 2012 with the participation of 338 individuals attending the private practice of a bariatric surgeon from Medellín (Colombia). With prior signed informed consent, the survey was filled out by each patient. The information gathered was sociodemographic in nature along with the World Health Organization's Quality of Life Brief Questionnaire (WHOQoL-Bref). Results. It was found that 82.2% were women and mean age was 41±12 years. Gastric bypass was practiced on 79.6% of the cases. Mean weight before surgery was 106.3±17.5 Kg and after surgery it was 73.2±13.4 Kg. Nine of every 10 participants classified their quality of life and state of health between extremely well and quite well. Quality of life was better in men, in those younger than 40 years of age, in those from socio-economic levels 4 to 6, and in those with educational level above the secondary (high school). Conclusion. As a consequence of the important and rapid weight loss occurring during the first months after surgery, most of the participants perceived having a good quality of life and were satisfied with their health status. For nursing, it is a challenge to implement educational programs and projects, bearing in mind the sociocultural diversity of the individuals and communities, through interdisciplinary and inter-sector work, which contributes to the well-being of obese individuals subjected to bariatric surgery and their families.
Key words: bariatric surgery; quality of life; health status; obesity, morbid.
RESUMEN
Objetivo. Identificar el estado de salud y calidad de vida (CV) de los pacientes posoperados de cirugía bariátrica. Metodología. Estudio cross-sectional realizado en 2012 en el que participaron 338 personas que asistieron a la consulta particular de un cirujano bariátrico de Medellín (Colombia). Previo consentimiento informado firmado, se aplicó una encuesta que fue diligenciada por cada paciente. La información recolectada fue de tipo sociodemográfica y el cuestionario abreviado de calidad de vida de la Organización Mundial de la Salud (WHOQoL-Bref). Resultados. El 82.2% pertenecía al sexo femenino, la edad media fue 41±12 años. Les practicaron Bypass gástrico al 79.6% de los casos. El peso medio antes de la cirugía fue de 106.3±17.5 Kg y después de ella de 73.2±13.4 Kg. 9 de cada 10 participantes calificaron entre extremadamente bien y bastante bien su calidad de vida y el estado de salud. Aquella fue mejor en los hombres, en los menores de 40 años, en quienes pertenecían a estratos socioeconómicos 4 a 6 y en los que tenían estudios superiores a los secundarios. Conclusión. Como consecuencia de la rápida pérdida de peso ocurrida durante los primeros meses tras la cirugía, la mayor parte de los participantes percibe tener una buena calidad de vida y está satisfecha con su estado de salud. Para la enfermería es un reto implementar programas y proyectos educativos, teniendo en cuenta la diversidad sociocultural de las personas y las comunidades, a partir de un trabajo interdisciplinar e intersectorial, que contribuya al bienestar de las personas obesas sometidas a cirugía bariátrica, así como al de su familia.
Palabras clave: cirugía bariátrica; calidad de vida; estado de salud; obesidad mórbida.
RESUMO
Objetivo. Identificar o estado de saúde e qualidade de vida (CV) dos pacientes pós-operados de cirurgia bariátrica. Metodologia. Estudo cross-sectional realizado em 2012 no que participaram 338 pessoas que assistiram à consulta particular de um cirurgião bariátrico de Medellín (Colômbia. Prévio consentimento informado assinado se aplicou uma enquete que foi diligenciada por cada paciente. A informação coletada foi de tipo sócio-demográfica e o questionário abreviado de qualidade de vida da Organização Mundial da Saúde (WHOQoL-Bref). Resultados. 82.2% foram mulheres, a idade média foi 41±12 anos. Praticaram-lhes Bypass gástrico ao 79.6% dos casos. O peso médio antes da cirurgia foi de 106.3±17.5 Kg e depois dela de 73.2±13.4 Kg. 9 de cada 10 participantes qualificaram entre extremamente bem e bastante bem seu CV e o estado de saúde. A qualidade de vida foi melhor nos homens, nos menores de 40 anos, nos que pertenciam a estratos socioeconômicos 4 a 6 e nos que tinham estudos superiores aos secundários. Conclusão. Como consequência à importante e rápida perda de importância ocorrida durante os primeiros meses depois da cirurgia, a maior parte dos participantes percebem ter uma boa qualidade de vida e estão satisfeitos com o estado de saúde. Para a enfermagem é um repto implementar programas e projetos educativos, tendo em conta a diversidade sociocultural das pessoas e as comunidades, através de um trabalho interdisciplinar e intersetorial, que contribua a bem-estar das pessoas obesas, suas famílias que são submetidas a cirurgia bariátrica.
Palavras chaves: cirurgia bariátrica; qualidade de vida; nível de saúde; obesidade mórbida.
INTRODUCTION
Obesity is an important risk factor for numerous chronic diseases, including diabetes, cardiovascular disease, and cancer. This ailment, which has become one of the epidemics of the 21st century, causes impairment and its complications represent a public health problem in almost all the countries in Latin America.1 In Colombia, in 2010, at least one in every two individuals from 18 to 64 years of age had excess weight, with the prevalence of obesity at 11% in men and 20% in women.2 Weight loss through medical and nutritional treatment does not always produce significant weight loss, which is why surgical techniques to control morbid obesity are currently considered the therapy of choice.
One of the aspects of growing interest in the research on obesity and bariatric surgery is the quality of life of patients subjected to this procedure, mostly performed in Anglo-Saxon countries.3,4 In Colombia, the studies are related to measuring the prevalence of complications;5 anesthetic techniques for bariatric surgery;6 and perioperative nutritional management7 among others. Improving the quality of life of individuals subjected to bariatric surgery is one of the main goals in healthcare; recognizing it permits carrying out nursing interventions that will impact upon the increase or maintenance of adherence to treatment and on decreasing morbidity and preventable mortality. This study sought to assess the quality of life of individuals who had been subjected to bariatric surgery in a group of patients from the city of Medellín.
METHODOLOGY
This was a cross-sectional study with the participation of 338 post-bariatric surgery patients from the private medical practice of a bariatric surgeon from the city of Medellín - Colombia. The information was gathered from February to August 2012. With prior informed consent signed, the self-reported survey was applied containing sociodemographic information, type of surgery, prior and current weight through clinical history and the World Health Organization Quality of Life Bref (WHOQoL-Bref) scale;8 this instrument is the reduced version of the WHOQoL-100, which evaluates quality of life as a multidimensional concept that incorporates the individual perception of the state of health, the psycho-social state, and other aspects of life. The abbreviated version has 26 items and two general questions on quality of life and health in general.
The domains comprising it are: Domain I Physical health (physical pain, need for medical treatment, energy for daily life, capacity for displacement, satisfaction with sleep, satisfaction with the ability to perform daily life activities, and satisfaction with the work capacity); Domain II Psychological Health (enjoyment of life, sense of life, capacity to concentrate, acceptance of physical appearance, satisfaction with oneself, and presence of negative feelings), Domain III Social relationships (satisfaction with personal relationships, satisfaction with sexual life, and satisfaction with friends); and Domain IV Environment (assuredness in daily life, healthy physical environment, enough money to cover needs, information necessary for daily life, opportunity to conduct leisure activities and leisure time, satisfaction with living conditions, access to health services and transportation). Each item has five Likert-type ordinal response options, the total score is the sum of the scores of the 26 items transformed according to the authors' indications until converting them into scores from 1 to 100 for the complete scale and by domain, which makes the results of investigations using the abbreviated instrument comparable to those used in the WHOQoL-100. The interpretation of the classification of the scale is that a higher score means better quality of life. The WHOQoL-BREF is validated into Spanish, having a Cronbach's alpha of 0.88 for the scale total.9
This study defined obesity as a BMI ≥ 30 kg/m2 and morbid obesity as BMI ≥ 40 kg/m10 and assumed quality of life as ''the perception individuals have of their place in existence, within the context of culture, and of the system of values in which they live and in relation to their expectations, norms, questionings. It is a very broad concept influenced in complex manner by the subjects' physical health, their psychological status, level of independence, and social relationships, as well as their relationship with the essential elements of their environment''.8
The SPSS software (version 21) was used to analyze the information. A descriptive analysis was conducted, including the description of frequencies, central tendency measures, and dispersion measurements. The one-factor ANOVA test was used to evaluate differences of scores per domain and total of the WHOQoL-Bref according to selected variables. Probability values <0.05 were considered statistically significant. To evaluate the consistency of the WHOQoL-Bref scale, the Cronbach's alpha was analyzed. The project was approved by the Ethics Committee in the Faculty of Nursing at Universidad de Antioquia in 2011.
RESULTS
General characteristics of the study sample
Table 1 shows that of the 338 individuals surveyed, 82.2% were females, with a mean age of 41.1±11.6 years (46.8% were younger than 40 years of age), 45.9% were married, 71.8% were from socio-economic level 3 and less, and 49.4% had secondary education as the maximum educational level. The most frequent type of surgery was gastric bypass with 79.6%, with 14±10 the average number of months since the surgery at the moment in which the information was gathered for this research.
Table 1. General characteristics of 338 post-bariatric surgery patients
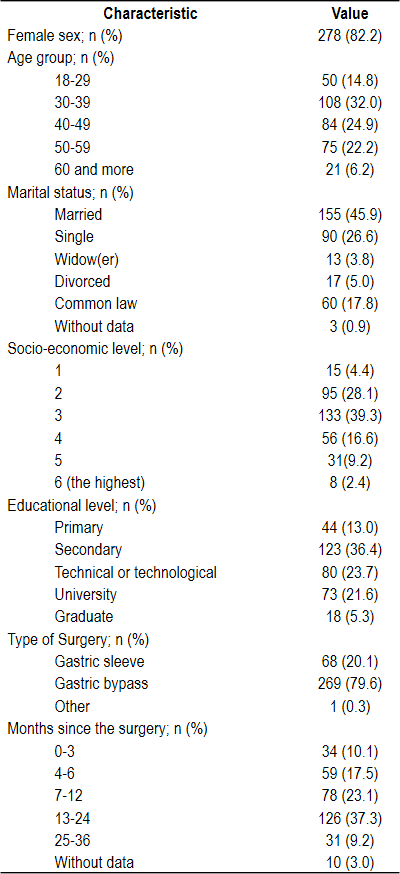
The BMI prior to the bariatric surgery was 41.2±4.5 and the current BMI was 28.4±4.0, with a difference of 12.8±3.7 (CI95%: 12.3-13.2), which is statistically significant (t=62.8, p<0.001).
Analysis of quality of life
As noted in Table 2, nine of every 10 individuals classified their quality of life and satisfaction with their state of health between extremely well and quite well.
Table 2. General quality of life and satisfaction with health of 338 post-bariatric surgery patients
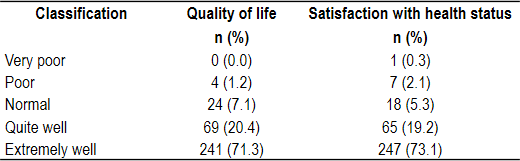
Table 3 shows details of the average score for each of the items in the WHOQoL-BREF scale. The best scores per domain were: Are you capable of moving from one place to another? in physical health (4.4); How much do you enjoy life? in psychological health (4.6); How satisfied are you with your personal relationships? in social relationships (4.2); and How satisfied are you with your living conditions? in environment (4.2). Rather, among the lowest per domain, there are: How satisfied are you with your sleep? in physical health (3.9); How often do you have negative feelings? in psychological health (3.6); How satisfied are you with your sexuality?, in social relationships (3.6); and, Do you have enough money to cover your needs?, in environment (3.0).
Table 3. Average scores of items from the WHOQoL-BREF scale of 338 post-bariatric surgery patients
The comparison of the total average and by domain of the WHOQoL-BREF scale according to some of the study variables can be seen in Table 4. By sex, it was found that men had higher scores with respect to women with said difference being statistically significant for the total and domains I, II, and III. An inversely proportional relationship of the score on quality of life and age group was noted, without this difference being significant only in domain IV.
Regarding marital status, only domain III (social) showed a statistically significant difference, given that single individuals had higher scores than the other groups. With respect to socioeconomic level, an inverse relationship of this variable with the score was found, with this difference not being significant only in domain I (physical health). A directly proportional and statistically significant relationship was noted between educational level and the total score in the four domains. By type of surgery and months since the surgery no differences were found with the total scores or per domains.
Table 4. Average scores of the WHOQoL-BREF scale by total and domains according to study variables of 338 post-bariatric surgery patients
The reliability of the WHOQoL-BREF scale in the study population was measured with Cronbach's alpha was 0.89.
DISCUSSION
This research permitted inquiring, from the nursing meta-paradigm, on three of its important concepts: the first two, the person and the environment, confirmed the perceptions on the quality of life of the bariatric surgery post-operative participants in relation to the dimensions of physical health, psychological health, social relationships, and environment; additionally, presenting the needs for care. The third concept inquired on the interventions upon which nursing should focus. Obesity, as a chronic disease, intervenes negatively on the quality of life and health of individuals who endure it. Rubio et al.,10 recommend that patients with morbid obesity who have not managed to lose weight in the long run with conventional therapy, should be offered surgical treatment, given that it provides superior results regarding weight loss, diminished co-morbidities and improved quality of life.10
In this study, the sociodemographic characteristics of the patients subjected to bariatric surgery were similar to others with respect to distribution by sex11 and age;11-13 regarding socio-economic level, most of those operated (67%) belonged to socio-economic levels 2 and 3, being low levels unlike the study by Maza et al., where the higher levels predominated.14 This group of patients had a mean weight loss of 33 Kg, which is similar to that found by González and Arriagada in Chilean patients.15 In eight out of every 10 of the study participants, gastric bypass was practiced, without statistical significance in the difference with respect to quality of life between this procedure and the gastric sleeve, agreeing with other similar research.16-18
A total of 92% of the participants scored quality of life as extremely and quite well after the procedure, which agrees with other similar studies.13,15,19 As per the dimensions of the WHOQoL-Bref, it was noted that in order from the greatest to the least, the dimensions with the best scale classification were: psychological health, physical health, social relationships, and environment; and the items with the best scores in this instrument were: enjoyment of life, mobility capacity, personal relationships, and satisfaction with home environment. These findings are comparable to those reported by other studies that manifest post-bariatric surgery improvement in functional capacity, mobility,13 in physical, social, and emotional aspects13 and self-esteem.15
Conversely, the items with the lowest scores in the WHOQoL-Bref were: satisfaction with sleep, having frequent negative feelings, satisfaction with sexuality, and having enough money to cover needs. One of the main co-morbidities after the bariatric surgery is sleep apnea and its prevalence in this population is estimated from 50 to 23%.20 Negative feelings in these patients remain present after surgery and the literature reports risk of anxiety and depression, associated to distorted bodily image.21 This also occurs with depression and suicidal thoughts.13 Instead, another study reports that after surgery negative feelings diminish, but not anxiety.22
Regarding lack of satisfaction with sexual life, the study by González et al.,15 describes that the sexuality of patients with morbid obesity improved in only half of the cases intervened surgically. This could be explained because sexuality in the obese is closely related to self-esteem and bodily image and to the relationship existing with the partner prior to the surgery. Additionally, it has been reported that up to 12% of the patients operated can worsen their sexuality or even suffer rejection from the partner.23 With respect to the item of having enough money to cover needs, this could be related to the fact that many of our patients were from socioeconomic levels 2 and 3, low and medium. Another important matter shown by this study is the relationship between educational level and quality of life, which was also described by Sarwer et al.,24 who also found association to greater mental health and physical health of the social function and better social function.
By sex, men scored the WHOQoL-Bref better for domains I, II, and III and the total. When comparing these results to those from the study by Tessierv et al.,25 it was found that both men and women had similar scores during the pre-operative period with respect to their mental health in the SF-36 instrument; during the post-operative period men improved their quality of life by week 20 and continued improving when assessed at week 40. On the contrary, women improved by week 20, but then experienced decreased scores during the rest of the study period. Regarding marital status, single individuals presented better scores for social relationships. The study by Mamplekou et al.,26 found that married participants with morbid obesity experienced more aggressive feelings than single or divorced patients, both before and after the operation. On the contrary, the study by Sarwer et al.,24 presents that over time, married individuals have higher scores in the SF- 36 regarding their social functioning, physical health, and mental health.
A limitation of this study was that in the literature review no publications were found related to the use of the WHOQoL-Bref applied to measuring quality of life after bariatric surgery, which hindered the comparison of the study's results. This instrument is easily understood and applied to measure quality of life and it would be important to validate it in our realm, specifically for individuals subjected to bariatric surgery.
The conclusion of this study is that as a consequence of the important and rapid weight loss occurring during the first months after surgery, the majority of the participants subjected to bariatric surgery perceive having a very good quality of life. For the researchers the results of this research have shown multiple care needs that go beyond the hospital context and which imply for the healthcare staff, and specially for nursing professionals, the establishment of interventions to promote health to satisfy the needs of post-bariatric patients, according to the individual characteristics, related to accompaniment and education that influence the understanding of their situation, adherence to treatment, diminished complications, and adoption of healthy lifestyles.
Specifically, for nursing it is highly important to continue research in this area, to contribute to the enhancement of care that responds to the true needs of individuals subjected to bariatric surgery. It is fundamental to include qualitative approaches that permit determining other aspects of the experience of undergoing bariatric surgery and which are part of the quality of life perceived by some of the users. In the same sense, develop research related to the complications and co-morbidities confronted by individuals after the procedure, given that these can influence on their quality of life and on its negative perception.
The results obtained in this research show the need to implement and intensify aid measures for the population with obesity aimed at education as the most effective strategy to transmit knowledge related to obesity and its effects on the damage to quality of life.
Acknowledgments. We thank Dr. María de los Ángeles Rodríguez Gázquez for contributions made to improve the article and Dr. Gloria Margarita Alcaraz López (RIP) for the encouragement to conduct this research.
REFERENCES
1. Kain J, Vio F, Alba C. Tendencias en la obesidad y factores determinantes en América Latina. Cad Saúde Pública. 2003; 19(suppl.1).S77-S860. [ Links ]
2. Fonseca Z, Heredia AP, Ocampo PR, Forero Y, Sarmiento OL, Álvarez MC, et al. Encuesta nacional de la situación nutricional. Bogotá: Instituto Colombiano de Bienestar Familiar; 2011. [ Links ]
3. vanNunen AMA, Wouters EJM, Vingerhoets JJM, Hox JJ, Geenen R. The Health-Related Quality of Life of Obese Persons Seeking or Not Seeking Surgical or Non-surgical Treatment: a Meta-analysis. Obes Surg. 2007; 17(10):1357-66. [ Links ]
4. Sutton D, Raines DA. Health-Related Quality of Life: Physical and Mental Functioning after Bariatric Surgery. Bariatr Nurs Surg Patient Care. 2008; 3(4):271-7. [ Links ]
5. Muñoz MN, Cepeda AM, Mosquera MS. Prevalencia de complicaciones en cirugía bariátrica en una clínica privada de la ciudad de Cali (Colombia). Cult Cuid. 2012; 9(1):6-16. [ Links ]
6. Gempeler FE, Díaz L, Sarmiento L. Manejo de la vía aérea en pacientes llevados a cirugía bariátrica en el Hospital Universitario de San Ignacio, Bogotá, Colombia. Rev Colomb Anestesiol. 2012; 40(2):119-23. [ Links ]
7. Savino P, Zundel N, Carvajal C. Manejo nutricional perioperatorio en pacientes con cirugía bariátrica. Rev Colomb Cir. 2013; 28(1):73-83 [ Links ]
8. World Health Organization WHO. Programme on Mental Health. WHOQoL–Bref. Introduction, administration, scoring and generic version of the assessment. [Internet]. Geneva: WHO; 1996 (cited Nov 12 2012). Available from: http://www.who.int/mental_health/media/en/76.pdf [ Links ]
9. Espinoza I, Osorio P, Torrejón MJ, Lucas-Carrasco R, Bunout D. Validación del cuestionario de calidad de vida (WHOQOL-BREF) en adultos mayores chilenos. Rev Méd Chile. 2001; 139(5):579-86. [ Links ]
10. Salas-Salvadó J, Rubio MA, Barbany M, Moreno B, Grupo Colaborativo de la SEEDO. Consenso SEEDO 2007 para la evaluación del sobrepeso y la obesidad y el establecimiento de criterios de intervención terapéutica. Med Clin (Barc) 2007;128(5):184-96. [ Links ]
11. Lier1 HØ, Biringer E, Hove O, Stubhaug B, Tangen T. Quality of life among patients undergoing bariatric surgery: associations with mental health- A 1 year follow-up study of bariatric surgery patients. Health Qual Life Out. 2011; 9(9):79-89. [ Links ]
12. Leiva MJ, Fuentealba C, Boggiano C, Gattás V, Barrera G, Leiva L, et al. Calidad de vida en pacientes operadas de bypass gástrico hace más de un año: Influencia del nivel socioeconómico. Rev Méd Chile 2009; 137: 625-33. [ Links ]
13. Grans R, Warth CF, Mattos Farah JF, Bassitt DP. Qualidade de vida e prevalência de dor osteoarticular em pacientes submetidos à cirurgia bariátrica. Einstein. 2012; 10(4):415-21. [ Links ]
14. Maza MP, Leiva L, Barrera G, Boggiano C, Herrera T, Pérez Y, et al. Evaluación a largo plazo del estado nutricional, composición corporal y densidad mineral ósea en mujeres operadas de bypass gástrico: impacto del nivel socioeconómico. Rev Méd Chile. 2008; 136(11):1415-23. [ Links ]
15. González P, Gómez G, Arriagada G. Evaluación mediante score BAROS de los resultados del bypass gástrico en el tratamiento de la obesidad mórbida. Rev Chil Cir. 2006; 58(5): 365-70. [ Links ]
16. Müller MK, Wenger C, Schiesser M, Clavien PA, Weber M. Quality of Life After Bariatric Surgery—A Comparative Study of Laparoscopic Banding vs. Bypass. Obes Surg. 2008; 18(12):1551–7. [ Links ]
17. Yip S, PlankLD, Murphy R. Gastric bypass and sleeve gastrectomy for type 2 diabetes: a systematic review and meta-analysis of outcomes. Obes Surg. 2013; 23(12): 1994-2003. [ Links ]
18. Mohos E, Schmaldienst E, Prager M. Quality of life parameters, weight change and improvement of co-morbidities after laparoscopic roux y gastric bypass and laparoscopic gastric sleeve resection—comparative study. Obes Surg. 2011; 21(3): 288–94. [ Links ]
19. Ocón Bretón J, Pérez Naranjo S, Gimeno Laborda S, Benito Ruesca P, García Hernández R. Eficacia y complicaciones de la cirugía bariátrica en el tratamiento de la obesidad mórbida. Nutr Hosp. 2005; XX(6): 409-14. [ Links ]
20. Sjostrom L. Lifestyle, Diabetes, & cardiovascular risk factors 10 years after bariatric surgery. N Engl J Med. 2004, 35(26): 2683–93. [ Links ]
21. Khawali C, Ferraz MB, Zanella MT, Ferreira SRG. Evaluation of quality of life in severely obese patients after bariatric surgery carried out in the public health care system. Arq Bras Endocrinol Metab. 2012; 56(1):33-8. [ Links ]
22. Aasprang A, Andersen J R, VÅge V, Kolotkin RL, Natvig GK. Five-year changes in health-related quality of life after biliopancreatic diversion with duodenal switch. Obes Surg. 2013; 23(10):1662–8. [ Links ]
23. Kinzl JF, Trefalt E, Fiala M, Hotter A, Biebl W, Aigner F. Partnership, sexuality, and sexual disorders in morbidly obese women: consequences of weight loss after gastric banding. Obes Surg. 2004; 14(4):455-8. [ Links ]
24. Sarwer DB, Wadden TA, Moore RH, Eisenberg MH, Raper SE, Williams NN.Changes in Quality of Life and Body Image Following Gastric Bypass Surgery. Surg Obes Relat Dis. 2010; 6(6):608–14. [ Links ]
25. TessiervA, Zavorsky GS, Kim DJ, Carli F, Christou N, Mayo NE. Understanding the determinants of weight-related quality of life among bariatric surgery candidates. J Obes. 2012; 12(1):1-9. [ Links ]
26. Mamplekou E, Komesidou V, BissiasCh, Papakonstantinou A, Melissas J. psychological condition and quality of life in patients with morbid obesity before and after surgical weight loss. Obes Surg. 2005; 15(8):1177-84. [ Links ]
