










Services on Demand
Journal
Article
 text in
text in  English (pdf)
English (pdf)
 Article in xml format
Article in xml format Article references
Article references
 Send this article by e-mail
Send this article by e-mailIndicators
-
 Cited by SciELO
Cited by SciELO -
 Access statistics
Access statistics
Related links
-
 Cited by Google
Cited by Google -
 Similars in
SciELO
Similars in
SciELO -
 Similars in Google
Similars in Google
Share

 Permalink
PermalinkInvestigación y Educación en Enfermería
Print version ISSN 0120-5307
Invest. educ. enferm vol.32 no.2 Medellín May/Aug. 2014
ARTÍCULO ORIGINAL / ORIGINAL ARTICLE/ ARTIGO ORIGINAL
Most Important Needs of Family Members of Critical Patients in Light of the Critical Care Family Needs Inventory
Necesidades más importantes de los familiares del paciente crítico a la luz del instrumento Critical Care Family Needs Inventory
Necessidades importantes dos familiares do paciente crítico à luz do instrumento Critical Care Family Needs Inventory
Cristóbal Felipe Padilla Fortunatti1
1RN. Hospital Clínico UC, Pontificia Universidad Católica de Chile, Chile. email: cristobalfelipe@gmail.com.
Receipt date: Oct 16, 2013. Approval date: Feb 10, 2014.
Article linked to research: none.
Subventions: none.
Conflicts of interest: none.
How to cite this article: Padilla CF. Most Important Needs of Family Members of Critical Patients in Light of the Critical Care Family Needs Inventory. Invest Educ Enferm. 2014;32(2): 306-316.
ABSTRACT
Objective.This work sought to identify the most important needs for family members of adult critical patients as described in the literature pursuant to the dimensions established in the "Critical Care Family Needs Inventory" (CCFNI) by Molter and Leske. Methodology.A literature review was carried out by using the CCFNI instrument. The databases used were: Pubmed, CINAHL, Proquest Nursing & Allied Health Source, Proquest Psychology Journals, LILACS, Science Direct, Ovid SP, PsyicINFO, and SciELO. The following limitations for the search were identified: adult patients, articles in English and Spanish, with abstract and complete text available and which had been published from 2003 to June 2013; 15 articles were included. Results.The family's hope on desired results and sincere communication with the healthcare staff turned out to be the most relevant needs, while the least important were related to comfort and having support structures or systems. Most of the studies were conducted in Asia and North America revealing differences in the order of importance assigned to each necessity. Certain sociodemographic and cultural characteristics impact upon how family members rank their needs; this also occurs with the nature of the most important needs for the family and the factors determining their prioritization. Conclusion.The articles included in this review mention the frequent interaction with the family and their holistic view of the person beyond the illness, determine that nurses are the most appropriate professionals to know and satisfy the family needs of critical patients.
Key words:intensive care units; needs assessment; family.
RESUMEN
Objetivo.Identificar las necesidades más importantes de los familiares del paciente crítico adulto descritas en la literatura conforme a las dimensiones establecidas en el "Critical Care Family Needs Inventory" (CCFNI) de Molter & Leske. Metodología.Se revisó la literatura en la cual se utilizó el instrumento CCFNI. Las bases de datos empleadas fueron: Pubmed, CINAHL, Proquest Nursing & Allied Health Source, Proquest Psychology Journals, LILACS, Science Direct, Ovid SP, PsyicINFO, y Scielo. Dentro de los límites de la búsqueda se tuvieron: pacientes adultos, artículos en idioma inglés y español, con resumen y texto completo disponible y que hubieran sido publicados desde el año 2003 a junio de 2013, de los cuales fueron incluidos 15 artículos. Resultados.Como las necesidades más relevantes se destacaron: la esperanza de la familia en los resultados deseados y la comunicación sincera con el personal de salud; mientras que las menos importantes se relacionaron con la comodidad y el contar con estructuras o sistemas apoyo. La mayor parte de los estudios fueron realizados en Asia y Norteamérica, en los cuales se observaron diferencias en el orden de importancia asignado a cada necesidad. Por otra parte, determinadas características sociodemográficas y culturales influyen en el modo en que los familiares jerarquizan sus necesidades, dada la naturaleza de estas y los factores que determinan su priorización. Conclusión.Los artículos incluidos en esta revisión hablan de la frecuente interacción con la familia y su visión holística de la persona más allá de la enfermedad, lo que determina que la enfermera sea la profesional más idónea para conocer y satisfacer las necesidades familiares del paciente crítico.
Palabras clave:unidades de cuidados intensivos; evaluación de necesidades; familia.
RESUMO
Objetivo.Identificar as necessidades mais importantes para os familiares do paciente crítico adulto descritas na literatura conforme às dimensões estabelecidas no "Critical Care Family Needs Inventory" (CCFNI) de Molter & Leske. Metodologia.Revisou-se a literatura na qual se utilizou o instrumento CCFNI. As bases de dados empregadas foram: Pubmed, CINAHL, Proquest Nursing & Allied Health Source, Proquest Psychology Journals, LILACS, Science Direct, Ovid SP, PsyicINFO, e Scielo. Dentro dos limites da busca se tiveram: pacientes adultos, artigos em idioma inglês e espanhol, com resumo e texto completo disponível e que tivessem sido publicados desde o ano 2003 a junho de 2013, foram incluídos 15 artigos. Resultados.A esperança da família nos resultados desejados e a comunicação sincera com o pessoal de saúde resultaram ser as necessidades mais relevantes enquanto as menos importantes se relacionaram com a comodidade e o contar com estruturas ou sistemas apoio. A maior parte dos estudos foram realizados na Ásia e na América do Norte observando-se diferenças na ordem de importância atribuído a cada necessidade. Determinadas características sócio-demográficas e culturais influem no modo em que os familiares hierarquizam suas necessidades e dada a natureza das necessidades mais importantes para a família e os fatores que determinam sua priorização. Conclusão.Os artigos inclusos nesta revisão falam da frequente interação com a família e sua visão holística da pessoa além da doença, determinam que a enfermeira seja a profissional mais idónea para conhecer e satisfazer as necessidades familiares do paciente crítico.
Palavras chave:unidades de terapia intensiva; determinação de necesidades; familia.
INTRODUCTION
Admitting an individual to an intensive care unit (ICU) generates an impact on the patient, as well as on the patient's family group. Literature describes that within this period of serious illness, the family of the critical patient experiences a unique set of needs related mainly to their perception of assurance, closeness, information, comfort, and support.1 These needs can be experienced silently, going unnoticed by the healthcare staff and which if not satisfied generate stress and anxiety in the family member.2 On the contrary, knowing and satisfying them strengthens the family's ability to interact and support the patient, increases satisfaction regarding the perceived care, and promotes trust and assurance in the nurse-patient relationship.3
The first professionals within the healthcare staff in showing interest for the needs of family members of critical patient were the nurses. In 1979, American nurse, Nancy Molter,4 elaborated a list of said needs based on surveys to nursing students and a bibliographic review that was later restructured by Jane Leske in 1991, becoming the instrument denominated "Critical Care Family Needs Inventory" (CCFNI). This instrument has 45 Likert-type questions, which are distributed into five dimensions: information (necessity for real information about the family member), proximity (necessity for contact and remaining near the family member), assurance (necessity for hope in the desired results), comfort (personal and comfort needs), and support (includes resources, support systems or structures).5
Besides the CCFNI, other instruments exist to assess both the needs of the families of critical patients and their satisfaction sharing certain characteristics like being self-administered, being applied to a single family member, and having adequate reliability and validity levels.6 Most of these instruments were created based on the CCFNI, pioneer in the assessment of family needs, which is currently the instrument most used throughout the world.
The aim of this review was to identify the most important needs for the family members of adult critical patients as described in the literature pursuant to the dimensions established by the CCFNI. With this, it is expected that nursing knowledge will be updated regarding the hospitalization experience endured by these families.
METHODOLOGY
A search was conducted in the Pubmed, CINAHL, Proquest Nursing & Allied Health Source, Proquest Psychology Journals, LILACS, Science Direct, Ovid SP, PsyicINFO, and SciELO databases during May and June 2013. The search strategy included the key words: "critical care family needs inventory", "CCFNI", "needs assessment", "intensive care", "family" and "critical care" with the corresponding translations into Spanish according to DeCS for LILACS and SciELO databases. The search limits included: adult patients, articles in English and Spanish, with abstract and complete text available, published as of 2003.
Exclusion criteria included: articles involving pediatric or neonate patients, qualitative studies, and applications of instruments different from the CCFNI to assess family needs. A total of 290 citations (Figure 1) were initially identified of which 114 were eliminated because they were duplicated and two articles were added via manual search. Thereafter, the remaining citations were analyzed based on their title and abstract, discarding a total of 141 citations and leaving 37 articles to be reviewed through complete text.
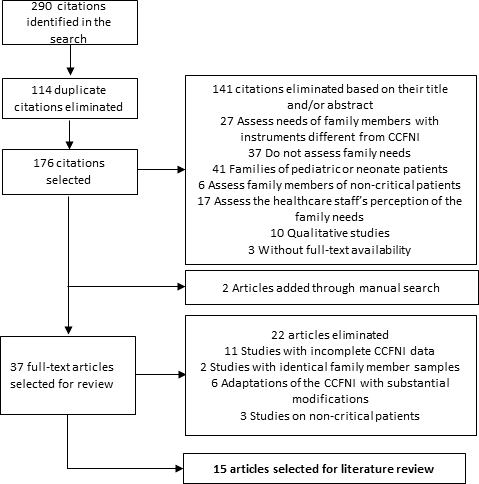
Figure 1.Flow chart of article selection
From the 37 full-text articles analyzed, a total of 22 studies were discarded, 11 of which reported incomplete data or data presented in a way that did not permit ranking the needs of the CCFNI, six studies corresponded to adaptations of the instrument with substantial modifications of the original list of 45 needs described by Molter and Leske (E.g.,: versions contemplating 11, 14, 20, or 31 items), three studies used the CCFNI in non-critical patients, and two used the same population of family members in another article included in this review; leaving 15 articles selected for the final analysis.
For the purpose of elaborating the hierarchical list of the family needs, we proceeded to assign a score to the most important family necessity from each study; said score diminished according to its relative position until reaching the least important necessity. These scores were weighted according to the number of participants in each study and then the sum was made of the score obtained by each of the needs weighted, obtaining the global list of family needs. To elaborate the list of needs according to geographic zone, the same procedure was used including the countries corresponding to each continent analyzed. Among the results included in this review, there are: identification of the most and least important needs for family members of critical patients, comparison according to geographic zones, and determinant factors of their ranking.
RESULTS
The investigations found reported a significant number of family members of critical patients around the world, which rank their needs differently. The total number of family members included in the 15 studies selected rose to 1392 (Table 1), distributed into 35 ICU (33 mixed ICU, 1 neurology ICU, and 1 coronary ICU) corresponding to 26 hospitals (public, private, and teaching). The number of family members included in the studies varies from 20 family members in China7 to 230 in Greece1, with an average of 92.8±63.9 family members per study. The continent including the highest number of family members in its research is Asia with 767 (55.1%) while Oceania8 reports only one study with 22 (1.8%). A study carried out in Brazil reports two samples comparing the needs among families belonging to a public hospital and a private hospital9.
Most of the studies were conducted in the United States17-20 (26.7%) and China7,11,14,16 (26.7%). No studies were found published in Spanish speaking countries, which fulfilled the inclusion criteria.
Table 1.Description of studies included
Most important family needs
A total of 86.7% of the articles included in this study reported at least 10 ranked needs,1,7-11,13-18 while the remaining articles mentioned only five needs.12,19 The needs perceived as most important by the family members of critical patients are related to the dimension of "assurance", with the most important being those of "having responses delivered sincerely" and "knowing the prognosis" (Table 2).
Table 2.List of the 10 most important family needs
Within the dimension of "information", the necessity "to know specific facts related to the patient's status" turned out to be the most important, occupying the sixth place. Of the ten most important needs, the dimension of "assurance" occupies the first five places and that of "information" four of the remaining five. No necessity from the dimension of "comfort" or "support" managed to placement within the ten most important needs.
When comparing the results of the studies according to the geographic zones with the highest number of family members involved, high heterogeneity can be noted in how the needs are ranked (Table 3).
Table 3.Order of the 10 most important family needs, according to geographic zones
W/S: Family necessity not scored in the global sum of studies; not possible to assign it a comparable position
The most important necessity for the families from the Asian studies, "having responses delivered sincerely", is in a similar position in North American families while for the latter the most important necessity is "being sure the best care possible is granted to the patient", which is in the eleventh place in Asian families. For South American families, "sensing the healthcare staff is concerned about the patient" turned out to be the most relevant necessity and which in other geographic zones occupied third (Asia) and eighth (North America) place, respectively. In spite of the difference in the importance attributed to each necessity, the most important continue corresponding to the dimensions of "assurance" and "information" independent of the geographic zone examined.
Least important family needs
Regarding the needs the family members perceive as least important, only eight studies reported them,7,8,11,13,14,16,18,19 adding a total of 612 family members (43.9%). Table 4 describes the least important needs, which were related to the spiritual support of the family members ("being notified of religious services available" and "being visited by a pastor"). Basic needs and those of comfort like "having good food in the hospital", "having comfortable furniture in the waiting room" or "having a telephone near the waiting room" resulted more important than religious support. The majority of these needs belong to the dimensions of "support" and "comfort", without finding any belonging to the dimension of "assurance" or "proximity".
Table 4.Order of the 10 least important needs
DISCUSSION
This study contributes to updating knowledge on the needs of family members of critical patients as described by the CCFNI. The most important needs for the families agree with existing reports to date21 and are related to the beliefs, hopes, and perceptions the family experiences during admission into ICU of a family member with vital risk.
Family uncertainty during the initial hours and the need of the healthcare staff to focus exclusively on the patient's vital needs could negatively affect contact during the first days. It is within this context where it is complicated to establish an affective link between the healthcare staff and the family, capable of generating honest communication that contextualizes the family on the patient's situation in the short and mid-term and which permits the personnel in charge of inspiring the necessary trust and assurance necessary to satisfy the needs of the family in crisis.
In relation to the least important needs, those belonging to the dimensions of "support" and "comfort" are also considered by literature as the least relevant.10,14 The lower importance related to needs of spiritual assistance could be attributed to the fact that the CCFNI is generally applied from 24 to 72 hours after admitting the patient, while the religious services required by the family members in ICU are mostly required during stages close to the patient's death. Belonging to a religion could also be considered as determinant in this order; however, only one of every five of the studies included mentions adherence to some type of religion or belief by the participating family members, which reaches 94% in some North American families18,19 and 40% in the Chinese families,14 with religious needs placed in the three studies in the last five places of importance. Likewise, a study in China11 reported differences in the prioritization of the needs of family members of patients who were about to be transferred to lower complexity units in comparison to their admission, which indicates that family needs evolve during hospitalization and that they must also be assessed days prior to admission.
Also, families act as guarantors of the rights of critical patients, assuming responsibility for decisions related to their care and treatment. Of the 45 needs assessed by the CCFNI, at least 40% could be directly related to Legislation 20.584 of the Patient's Rights and Duties, recently promulgated in Chile.22 This law, in paragraphs 3 and 4 expressly refers to the right to access to sufficient, timely, truthful, and comprehensible information; to the right to facilitate the companionship of family members; and to the right to spiritual assistance. Assessment of family needs, with instruments like the CCFNI, will help to establish the degree of importance the family members of critical patients attribute to certain rights guaranteed by the law, permitting providers and the healthcare staff to optimize resources destined to assuring, respecting, and promoting these rights.
The difference in the relative order of the needs among countries or continents could be explained in part by the number of studies and family members each zone contributes to this review. Nevertheless, some reports exist suggesting that the cultural background of the families studied would impact on how they prioritize their needs whether through their beliefs, values, or religion1,10,11,14,16,19 or through their country's geographic location, East or West.7,16 The studies evaluated also describe certain variables that would influence upon how the families organize and satisfy their needs, among which there are: educational and socioeconomic levels,1,11,13 being a female family member,11 public or private hospital,9 religion, and prior experience in ICU.14 Nonetheless, the needs included in the dimension of "Assurance" would not have their prioritization affected, given that they are independent of the families' demographic and cultural profile.
Bearing in mind the impact of the previously mentioned sociodemographic variables, future research in the field of family needs should be complemented with qualitative methodologies, which would help to clarify the meaning of concepts like "feeling that there is hope", "sensing that the healthcare staff is concerned about the patient" or "having responses delivered sincerely" that can be influenced by diverse factors and which necessarily require more profound understanding of what the family understands by hope, concern, or sincerity.
Assessing the needs of Jordanian families, Al-Hassan10 suggests a holistic approach of the dimensions and family needs by taking as an example the necessity for comfort, which not only encompasses the physical but also the environmental, sociocultural, and psycho-spiritual. From this perspective, in a study conducted in South Korea using mixed methodology,23 the needs included in the dimension of "assurance" were also considered the most important by the CCFNI, as well as by the qualitative data. Upon delving into the description of these needs, the family members refer to the lack of words of hope from the physicians and reproach their excessively defensive posture.
Similarly, access to information, which is also in second place, turns out difficult given the absence of the physicians and the lack of clarity from the nurses. However, this vagueness could be attributed to the type of information solicited by the family members and the nurses' impossibility to provide, given legal reasons, certain type of information related to the patient. Additionally, a recent review of literature related to family participation in caring for the critical patient24 confirms that the need for information and hope are the most important from the qualitative perspective, which is compatible with the results described in this review.
The lack of studies published in Spanish speaking countries in South America partially limits knowledge of the most important needs in this population in particular; to date, one study has been conducted in Brazil applying the CCFNI in its version adapted from the original.9 Although the CCFNI shows important differences in the prioritization of needs according to geographic zone and the cultural background of the family member, the most important dimensions are independent of these factors; not so the needs in particular.
All these elements must be considered when planing interventions seeking to know and/or satisfy family needs that should be based on an objective evaluation of these needs, using validated and reliable instruments like the CCFNI, besides incorporating - but to a lesser measure - the experiences reported by families in other countries and the perceptions of some members of the healthcare staff, given that evidence has described that these last do not always know or are capable of satisfying these needs,18 which can be translated into ineffective efforts and eventual damage to the family.7 A diverse group of individuals interact in ICUs with nurses being the professionals with the most adequate tools to satisfy these needs7,12,14,15,17,25 given their frequent interaction with the family members and their clear and familiar language. The holistic view of patients and of their family environment, added to the approach centered on the person rather than on the illness, place nurses in a privileged position to fulfill this objective; however, healthcare institutions need to generate the necessary organizational conditions for nurses to assume this role, which is deteriorated due to the current shortage of nursing professionals and their high work load.26
This study concludes that the principal needs of families of critical patients are related to assurance, understood as hope for the desired results for the family member hospitalized; followed by the necessity for information, which implies communicating with foundation and detail aspects related to the patient's care and treatment. Diverse factors exist that can affect how families categorize their needs, which are mainly related to the sociodemographic and cultural characteristics of the family member. Keeping the aforementioned in mind and the shortage of studies conducted with Spanish speaking South American families, the results from this review are partially applicable to our continent. The "Critical Care Family Needs Inventory" continues being a valid instrument that permits knowing the family needs; however, its results must be complemented with qualitative methodologies, given the nature of the concepts involving said needs. Within the healthcare staff, nurses are the most appropriate professionals to lead initiatives seeking to know and satisfy the needs of families of critical patients.
REFERENCES
1. Chatzaki M, Klimathianaki M, Anastasaki M, Chatzakis G, Apostolakou E, Georgopoulos D. Defining the needs of ICU patient families in a suburban/rural Greek population: a prospective cohort study. J Clin Nurs. 2012; 21(13-14):1831-9. [ Links ]
2. Davidson JE, Powers K, Hedayat KM, Tieszen M, Kon AA, Shepard E, et al. Clinical practice guidelines for support of the family in the patient-centered intensive care unit: American College of Critical Care Medicine Task Force 2004 - 2005. Crit Care Med. 2007; 35(2):605 - 22. [ Links ]
3. Buckley P, Andrews T. Intensive care nurses' knowledge of critical care family needs. Intensive Crit Care Nurs. 2011; 27(5):263-72. [ Links ]
4. Molter NC. Needs of relatives of critically ill patients: a descriptive study. Heart Lung. 1979; 8(2):332-9. [ Links ]
5. Leske JS. Internal psychometric properties of the Critical Care Family Needs Inventory. Heart Lung. 1991; 20(3):236-44. [ Links ]
6. Olano M, Vivar CG. Instrumentos para la valoración de las necesidades de los familiares de pacientes ingresados en cuidados intensivos: una revisión sistemática. An Sist Sanit Navar. 2012; 35(1):53-67. [ Links ]
7. Chien WT, Chiu YL, Lam LW, Ip WY. Effects of a needs-based education programme for family carers with a relative in an intensive care unit: a quasi-experimental study. Int J Nurs Stud. 2006; 43(1):39-50. [ Links ]
8. Kinrade T, Jackson AC, Tomnay J. The psychosocial needs of families during critical illness: comparison of nurses' and family members' perspectives. Aust J Adv Nurs. 2009; 27(1):82-8. [ Links ]
9. Freitas KS, Kimura M, Ferreira KASL. Necesidades de los familiares de paciente en unidades de terapia intensiva: análisis comparativo entre hospital público y privado. Rev Latino-am Enfermagem. 2007; 15(1):84-92. [ Links ]
10. Al-Hassan MA, Hweidi IM. The perceived needs of Jordanian families of hospitalized, critically ill patients. Int J Nurs Pract. 2004; 10(2):64-71. [ Links ]
11. Chien WT, Ip WY, Lee IY. Psychometric properties of a Chinese version of the critical care family needs inventory. Res Nurs Health. 2005; 28(6):474-87. [ Links ]
12. Hashim F, Hussin R. Family Needs of Patient Admitted to Intensive Care Unit in a Public Hospital, Procedia Soc. Behav. Sci. 2012; 36:103-11. [ Links ]
13. Khalaila R. Patients' family satisfaction with needs met at the medical intensive care unit. J Adv Nurs. 2013; 69(5):1172-82. [ Links ]
14. Lee LY, Lau YL. Immediate needs of adult family members of adult intensive care patients in Hong Kong. J Clin Nurs. 2003; 12(4):490-500. [ Links ]
15. Omari FH. Perceived and unmet needs of adult Jordanian family members of patients in ICUs. J Nurs Scholarsh. 2009; 41(1):28-34. [ Links ]
16. Wang W, Li X, Gao R. The needs of Chinese family members of acute myocardial infarction patients during the critical phase of admission to coronary care. World Crit Care Nurs. 2004; 3(4):96-102. [ Links ]
17. Davidson JE, Daly BJ, Agan D, Brady NR, Higgins PA. Facilitated sensemaking: a feasibility study for the provision of a family support program in the intensive care unit. Crit Care Nurs Q. 2010; 33(2):177-89. [ Links ]
18. Hinkle JL, Fitzpatrick E. Needs of American relatives of intensive care patients: perceptions of relatives, physicians and nurses. Intensive Crit Care Nurs. 2011; 27(4):218-25. [ Links ]
19. Obringer K, Hilgenberg C, Booker K. Needs of adult family members of intensive care unit patients. J Clin Nurs. 2012; 21(11-12):1651-8. [ Links ]
20. Prachar TL, Mahanes D, Arceneaux A, Moss BL, Jones S, Conaway M, et al., Recognizing the needs of family members of neuroscience patients in an intensive care setting. J Neurosci Nurs. 2010; 42(5):274-9. [ Links ]
21. Paul F, Rattray J. Short- and long-term impact of critical illness on relatives: literature review. J Adv Nurs. 2008; 62(3):276-92. [ Links ]
22. Ministerio de Justicia, Subsecretaria de Salud Pública. Ley 20584. Regula los derechos y deberes que tienen las personas en relación con acciones vinculadas a su atención en salud Santiago; (Abr 3, 2012). [ Links ]
23. Yang S. A mixed methods study on the needs of Korean families in the intensive care unit. Aust J Adv Nurs. 2008; 25(4):79-86. [ Links ]
24. Al-Mutair AS, Plummer V, O'Brien A, Clerehan R. Family needs and involvement in the intensive care unit: a literature review. J Clin Nurs. 2013; 22(13-14):1805-17. [ Links ]
25. Auerbach SM, Kiesler DJ, Wartella J, Rausch S, Ward KR, Ivatury R. Optimism, satisfaction with needs met, interpersonal perceptions of the healthcare team, and emotional distress in patients' family members during critical care hospitalization. Am J Crit Care. 2005; 14(3):202-10. [ Links ]
26. Penoyer DA. Nurse staffing and patient outcomes in critical care: a concise review. Crit Care Med. 2010; 38(7):1521-8. [ Links ]
