











 text in
text in  English (pdf)
English (pdf)
 Article in xml format
Article in xml format Article references
Article references
 Send this article by e-mail
Send this article by e-mail Cited by SciELO
Cited by SciELO  Cited by Google
Cited by Google  Similars in
SciELO
Similars in
SciELO  Similars in Google
Similars in Google 
 Permalink
PermalinkIntroduction
Subjective memory complaints in the elderly may have several natural causes. They may be due to the aging process itself, deriving from depressive mood and low education or from cognitive disorders. This term is used to designate a report of memory problems, which may or may not be perceived by others, although currently there is no consensus on the definition of this symptom.1 This leads to reflection on the elderly’s health promotion means and the preservation of their mental health, focusing on specific nursing interventions for each of the older age groups, that is, with subjective memory complaint only, or with subjective memory complaints and one of the following conditions: low education or humor complaint (mourner, loneliness). Previous studies bring information that cognitive dysfunction negatively influences in activities of daily living - ADLs.2,3) The interpretation of the results show that cognitive function and functional capacity can be correlated.2 Thus, as an individual loses cognitive ability, they can also lose their functional capacity, responsible for assessing the subjective complaint. The concept of functional capacity is related to the ability to perform activities that allow taking care of themselves and live independently.
Although subjective memory complaints are associated with psychological factors such as anxiety, depression and high personal requirement, they represent strong impact on the assessment of functional capacity. Subjective memory complaints among non-demented elderly are not only secondary to depression, but reflect the cognition status and express, in part, a realistic detection of cognitive deficit.4 In addition, there are suggestions that subjective memory complaints, particularly in older individuals and among those with early low cognitive status, can also express significant damage in the future.5 A major cause of subjective memory complaint is the depressive state, the most frequent cause of emotional distress and worsening of quality of life in the elderly, associated with deficits in functional capacity.6) Other factors that may contribute to this situation are the cognitive complaints from aging and low education in the elderly, which may lead to functional decline and can even cause dependency.7)
Formal education can also affect cognitive performance in tests such as the Mini Mental State Examination (MMSE). In addition, people with low education could be wrongly identified as at risk for dementia. Studies indicate that participants with more years of formal education had better MMSE scores than those with low education.8 In general, the level of education seems to be positively correlated with better performance of the elderly.9 Thus, the nursing interventions encompass group activities, called cognitive stimulation workshops, or memory workshops, which aim to encourage the elderly to carry out activities for the memory, for the performance of cognitive functions and Activities of Daily Living (ADLs).10,11) Given the above, it was defined as objective: to evaluate the functional capacity of elderly people in workshops for cognitive stimulation over a year, divided into three intervention subgroups (elderly with exclusive memory complaint, or associated with low education, or with depression) and a control group.
Methods
This is a study with a quantitative approach to evaluate the effect of intervention in the form of workshops before and after the functional capacity screening test in a longitudinal perspective, throughout one year, from July 2013 to July 2014. The research location a public university used by the extension project: Cognitive Memory, adherence to treatment and Technological Innovation: actions to promote health in old age, in Niteroi (RJ), Brazil. The research subjects make up a sample of 67 elderly people, of both sexes, aged from 60 to 88, registered in the social project of university extension for the elderly called Advanced Space UFF. Altogether, there are 200 registered participants of extension activities including theater, yoga, language course, water aerobics, fall prevention and citizenship workshops. It is noteworthy that the elderly spontaneously chose cognitive stimulation workshops, make an application, and then are sent to carry out the functional capacity evaluation tests, and compliance with selection criteria for inclusion in the workshops.
It was adopted as inclusion criteria for each subgroup: older adults with subjective memory complaints, more than eight years of schooling, and MMSE greater than or equal to 26 points, 20 seniors were referred to this group called healthy seniors; in the low education level subgroup, there were 11 subjects with subjective memory complaints, five, illiterate and 6 with up to 5 years of schooling; as for seniors with humor complaint, the group of depression, the criteria adopted were scores on the Geriatric Depression Scale (GDS) of 4 or more points and was composed of 25 elderly people. The control group consisted of 11 subjects with more than 8 years of schooling, more than 26 points in MMSE, and less than three points in GDS; this group did not receive cognitive therapy intervention, only conventional treatment that deals with other activities proposed in the Advanced Space. It was adopted as exclusion criteria elderly participants with a diagnosis of dementia, with limited mobility to the location and those with more than three unjustified absences in workshops.
Cognitive screening tests were applied for the data collection, before the start of the workshops and after six weeks and one year. The facilitator nurse responsible for intervention did not participate in pre and post evaluations, minimizing possible bias in research. In the group with humor complaints, the coordination of activities was performed together with the psychologists.
Regarding the assessment tests used, the MMSE evaluates the individual regarding the temporal orientation, spatial orientation, attention and calculation, immediate memory, recall, language, writing, and constructive skills.12,13 In Brazil, the validated MMSE score ranges from zero to 30 points, and has the level of education as an aid in its classification results. The cutoff points according to education level are: 13 points for illiterates, 18 points for average schooling (up to 8 years of formal education) and 26 points for high school subjects (over 8 years).12,14) The clock test helps in assessing the ability to think abstractly and to plan, initiate, continue and determine the time to complete a complex behavior. It is usually carried out in association with MMSE, which is widely used for screening of diseases that lead to cognitive and/or memory impairment. The elderly is asked to draw a clock with all hands and numbers, marking the time of 11:10. The total score sums four points, of which one point is for the circle, one point for the numbers, one point for the correct position inside the watch, and one point for setting the hours correctly.12,13
Another test used was the Word Recall Test (WRT). It assists in the evaluation of language, semantic memory and executive functions. It is requested that the elderly speaks the greatest possible number of names of animals in a minute. After this time, it is expected a result between 12 to 18 animals. The repetitions are also evaluated, by underlining the repeated animals. Values lower than expected scores and the number of repetitions assist in evaluating a possible cognitive impairment.12
The rating scale Instrumental Activities of Daily Living (IADL) - Lawton examines the degree of dependence to perform the following activities: use of telephone, getting out of the house, shopping, food preparation, participation in house chores, management of medications and management of financial life. The evaluation items are divided into: fully independent, partially dependent, totally dependent and/or unable to perform a certain daily activity.15) Thus, the results are analyzed as follows: values of 21 points are classified as completely independent. The cases below this value have some degree of dependence and 7 points for a totally dependent person.
The GDS evaluates cases of mood disorders, and it is a useful test for screening these disorders. It asks questions relating to the individual's perspective on their life and has 15 items that request yes or no answers; the cutoff point is 6 and items forward to further evaluation with results of more than nine points.16
The development of memory workshops as a nursing intervention follows the recommendation proposed by the Taxonomy Nursing Interventions Classification - NIC, Domain 3 - Behavioral, and Class P - Cognitive Therapy: "Interventions to enhance or promote desirable behavior, or to change undesirable behavior”.17) For intervention techniques in the form of workshops, the available literature was used as a basis. Thus, the exercises were adapted to the level of understanding of participants in each intervention group, so that they become meaningful to the participants.18,19
The descriptive analysis of the variables was presented in the form of tables and consisted of calculating the mean, median, standard deviation, minimum, maximum and amplitude. To compare the values between the intervention groups, authors used the Kruskal-Wallis test, a nonparametric test quite effective in comparison of n unpaired groups, which seeks to know whether these groups have the same mean.20) The result against the null hypothesis indicates difference in the mean of at least one of the groups. For cases in which the null hypothesis of the Kruskal-Wallis test was rejected, researchers used the exact Wilcoxon test, a nonparametric test that compares two unpaired groups.20 In this test, the result against the null hypothesis indicates that there is difference in the median of the two groups. The level of significance was set at 0.05. The results were obtained from the software R.
It is noteworthy that the research was approved under the opinion 250,132/13, meeting the requirements of Resolution 466/2012 of the National Health Council for research involving human beings. All steps of the research, as well as its goals and willingness on participation were informed and after agreement, the elderly signed the Informed Consent Form.
Results
Table 1 provides information on the distribution of data, such as mean, median, standard deviation, minimum, maximum and range of the amplitude to which the data is distributed, to all three evaluations carried out in intervention subgroups.
Table 1 Distribution of statistical averages of three evaluations conducted in the intervention subgroups and control group. Brazil, 2014.
| MEEM | |||||||
|---|---|---|---|---|---|---|---|
| Subgroups | Mean | Median | Standard deviation | Minimum | Maximum | Amplitude | p-value |
| Healthy seniors | 28.05 | 28.5 | 1.67 | 25 | 30 | 5 | 0.002 |
| Low education level | 23.64 | 24 | 2.80 | 20 | 28 | 8 | |
| Depression | 26.52 | 26 | 3.02 | 20 | 30 | 10 | |
| Control | 25.54 | 25 | 3.14 | 20 | 30 | 10 | |
| GDS | |||||||
| Healthy seniors | 1.25 | 1 | 1.02 | 0 | 4 | 4 | < 0.001 |
| Low education level | 1.91 | 1 | 2.47 | 0 | 9 | 9 | |
| Depression | 4.36 | 4 | 2.48 | 0 | 11 | 11 | |
| Control | 1.45 | 1 | 1.51 | 0 | 4 | 4 | |
| Lawton | |||||||
| Healthy seniors | 20.35 | 21 | 1.14 | 18 | 21 | 3 | 0.19 |
| Low education level | 19.73 | 20 | 1.10 | 18 | 21 | 3 | |
| Depression | 20.44 | 21 | 0.77 | 19 | 21 | 2 | |
| Control | 20.18 | 21 | 1.25 | 17 | 21 | 4 | |
| WRT | |||||||
| Healthy seniors | 17.85 | 18 | 4.20 | 11 | 29 | 18 | 0.020 |
| Low education level | 13.09 | 14 | 3.02 | 7 | 17 | 10 | |
| Depression | 17.36 | 17 | 5.43 | 9 | 32 | 23 | |
| Control | 14.64 | 15 | 4.61 | 6 | 21 | 15 | |
| Clock | |||||||
| Healthy seniors | 2.90 | 3.5 | 1.29 | 1 | 4 | 3 | 0.097 |
| Low education level | 1.82 | 2 | 1.33 | 0 | 4 | 4 | |
| Depression | 3.04 | 3 | 1.06 | 1 | 4 | 3 | |
| Control | 2.64 | 3 | 1.36 | 1 | 4 | 3 | |
For the study evaluations, the null hypothesis was rejected (p-value <0.05) in three of them, MMSE, GDS and WRT. Thus, there is evidence to say that there is difference between the intervention groups, in one of these assessments. For Lawton and Clock the null hypothesis was not rejected (p-value> 0.05) and therefore there is no evidence to say that the intervention groups are different, in these assessments.
It was observed that in the group of healthy seniors, the mean MMSE score was 28.05; in the depression group, 26.52; 25.54 in the control group; and 23.64 in the low education group. These data lead to the conclusion that low education is a factor influencing the cognitive response of the elderly, and although they do not present positive screening for cognitive impairment, this group is the most likely to this condition. The GDS showed that the depression group had the highest mean, 4.36, when compared to the low education group, with 1.91, the control group, with 1.45 and the healthy seniors, with 1.25. Regarding the IADL scale, Lawton, the means found in the study were 20.44 for the depression group; 20.35 for healthy seniors; 20.18 for the control group and 19.73 for individuals with low education level.
Although there was no significant impairment in performing IADL's in any group, it is noteworthy that the lowest mean found in the low education group may be related to learning limitations in handling and instrumental operation in activities that make it possible to maintain their independence in community.
Relating to WRT, the mean was 17.85 for the healthy seniors group; 17.36 in the depression group; 14.64 in the control group and 13.09 in the low education group. Because this test depends on a word framework, it was expected poor performance of the group with low education.
The clock test showed no clinical signs of cognitive impairment in any group. The mean found for this test was 3.04 for the depression group; 2.9 for healthy seniors; 2.64 for the control group and 1.82 for the low educational level group. The low mean for this latter group may be related to the constructive difficulty and dexterity of the executive fine motor skill for the design architecture, showing no impairment of cognitive functioning.
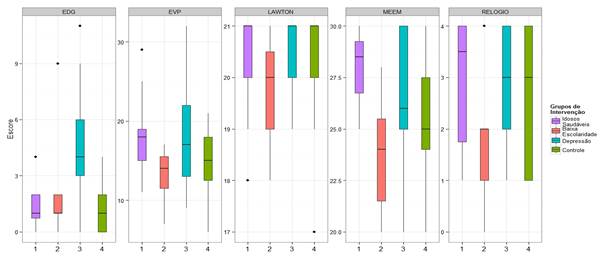
For MMSE, GDS and WRT, the exact Wilcoxon test was performed for two samples, in order to know which of the intervention groups behaved differently, comparing whether there was improvement in functional capacity assessment tests after the used intervention. Thus, Table 2 and Figure 1 show the p-value found for each pair of tested groups.
Table 2 Comparative distribution for two samples pre and post intervention. Brazil, 2014
| MEEM | ||||
|---|---|---|---|---|
| Subgrupos | Healthy seniors | Low education level | Depression | Control |
| Healthy seniors | - | < 0.001 | 0.1089 | 0.0204 |
| Low education level | - | 0.0149 | 0.1724 | |
| Depression | - | 0.4256 | ||
| Control | - | |||
| GDS | ||||
| Healthy seniors | - | 0,6401 | < 0,001 | 0.945 |
| Low education level | - | < 0,001 | 0.735 | |
| Depression | - | < 0.001 | ||
| Control | - | |||
| WRT | ||||
| Healthy seniors | - | 0.0012 | 0.6052 | 0.1071 |
| Low education level | - | 0.0229 | 0.2611 | |
| Depression | - | 0.2564 | ||
| Control | - | |||
Regarding the MMSE, there was evidence to say that the group of healthy seniors showed different median from low education and control groups, i.e., the healthy group achieved better results in the MMSE than the other groups. And the low education group showed different median from the depression group. In WRT evaluation, the healthy seniors group showed median different from the low education group, and the low education group had median different from the depression group. It is noteworthy that the emphasis on these groups, healthy and low education, was the subjective memory complaint, but adapted to each level of cognitive and educational performance. As for the GDS, it is possible to say that the depression group is the only one that shows median different from the others; this may because it had specific and targeted interventions to the humor complaint, which did not occur in the others.
Discussion
The cognitive stimulation groups were aimed at the promotion of cognitive performance and creating new possibilities of being, of feeling belonging to the world. To ensure the proper functioning of memory, some interrelated aspects must be considered, such as consciousness, attention, motivation, processing speed and perception.21 In addition to activities that are attractive to individual and collective interests, contributing to the strengthening of group interaction, to the act of belonging to the group.
The use of tests and functional capacity screening scales are essential for tracking and validation of clinic "suspicion", as in the case of symptomatology suggestive of cognitive impairment in the elderly. At the same time, it is important to standardize such instruments, ensuring the proper use in the evaluation, the possibility of comparisons between studies, and the record of cognitive, behavioral/psychological profiles and of performance in activities of daily life of the elderly.22) In a study conducted in Belo Horizonte, with the elderly residents of a long-stay institution for the elderly, the authors considered that the performance on the MMSE was low, since 93.3% had values below the cutoff point for schooling.23
Statistically, there was vulnerability in the depression group for memory and humor complaints, which reports to the need for close monitoring of depressive symptomatology and nursing interventions aimed at contributing to the promotion of mental health. For this observation, researchers defend the idea of strengthening team work, since these elderly need to receive special treatment and in groups that have the same feature, which enhances the language, but that address issues of humor, as they tend to somatize many emotions. It should be noted that heterogeneous groups of older adults with subjective memory complaints can contain these three subgroups combined, which at first may seem like only one thing, all complain of memory only, including the group complaining of humor that cannot report or express subjective problems when seeking the cognitive stimulation workshops; it is only detected in a detailed interview with individual conduction of tests and scale. Individuals with characteristics of humor complaints are often people living alone, with insulation complaint, or recently bereaved. Because they cannot express their feelings, they tend to somatize a more significant memory loss than it would be. During the group activities, they tend to manipulate speech, the group, in an attitude of calling the group's attention to their memory difficulties; this may be one of the drawbacks in the practice of heterogeneous groups.
Depressive symptoms are very common in the elderly, most often evidenced through negative expressions towards themselves, others, the world and the old age. They reveal a diminished perception of their abilities, low self-esteem and adopt a reduced participation.24 On the other hand, the low educational group also revealed to be a group susceptible to depressive symptoms. According to Fonseca, the mental health assessment assumes, by itself, a complex set of variables that affect its results, and that other factors such as sensory deficit and low education may interfere with the assessment process.25) However, individuals with low education, if put in heterogeneous groups with individuals with subjective memory complaint and who have higher level of education, can feel inhibited to participate, behaving as disinterested or apathetic towards the activity, and finally, may be confused with people with low mood.
Similarly, the Lawton test is little sensible to detect influences of low educational level in the implementation of life activities or sensory deficits. One of the most present issues in the low education group, for example, was the difficulty in managing their financial lives and their need for help, therefore, considered in this case as semi-dependent. This refers to the fact of considering everyday activities in the preparation of the activities for the cognitive stimulation workshops, such as games of supermarket, bank or travel items. In addition, the Lawton index should be used with caution in elderly men, especially in some activities such as washing clothes, cooking and house chores, where the elderly’s disability may be related to the lack of activity due to personal/cultural factors, and must be relativized.26
Similarly, it was observed worse performance in WRT by the low education subgroup. As this test depends on a word framework, it was expected poor performance by the group with low education. Therefore, it is recommended to associate the Clock test the others, as it is simple to operate, it has no semantic diversity and is not of a scale with written items. It consists of objective commands to perform tasks, which do not depend on the subjective interpretation of the examiner or the examinee, and even individuals with low education or illiterate are able to accomplish it. (27 There is the need to invest in cognitive stimulation activities that do not rely solely on reading and language, but can be more visual and related to daily activities, to encourage the participation of a relevant elderly group that did not have the same opportunity of schooling, but who is able to continue to learn in normal human development cycle.
Based on the data, it is also observed that the less educated elderly showed greater decline in Clock test, WRT, Lawton and MMSE. In the case of Lawton, the rationale for the worst performance of these elderly is given by their higher degree of dependence compared to other groups. Despite the recall of words and the clock test are able to identify cognitive deficits, the MMSE is believed to be the best assessment tool for this group, since this test is very detailed and enables more reliable results of the cognitive status of the elderly with low education. Therefore, the low education group, by having lower cognitive reserve and increased risk for severe cognitive impairment, must be separated from the others so they can achieve better performance and follow-up. The group of healthy seniors had the best results in all tests. This fact along with the others presented shows once again how important the separation of groups is in the application of cognitive stimulation workshops, which is a proposition model, recommended to give follow-up on projects and gerontological practices.
The conclusion of this study is that the cognitive stimulation activities were effective in maintaining the functional capacity of participants and were especially configured as an effective strategy for socialization and health promotion. Participation in cognitive stimulation workshops allows monitoring group and predicting possible severe cases. The intervention also favors minimizing symptoms of memory loss and depression, often triggered by the feeling of loneliness, by encouraging group participation, as well as inciting the maintenance of independence. There is highlight to the social relevance of the cognitive stimulation project, which, once a year, attended individuals free of charge, offering skilled nursing care and multidimensional evaluation. It provided vocational training in gerontological nursing and gerontology, in a multidisciplinary approach, in contact with the team of professionals, emphasizing the multidimensionality of the human aging process. The limitation of the study relates to the non-randomness of the sample and/or randomization, but comparative studies of interventions that outline the groups certify reliability of the data presented, ensuring better homogeneity and chances of detecting the power of the intervention by reducing the high variability biases among and between groups.

