











 text in
text in  English (pdf)
English (pdf)
 Article in xml format
Article in xml format Article references
Article references
 Send this article by e-mail
Send this article by e-mail Cited by SciELO
Cited by SciELO  Cited by Google
Cited by Google  Similars in
SciELO
Similars in
SciELO  Similars in Google
Similars in Google 
 Permalink
PermalinkIntroduction
Emotional alterations are evident in people enduring breast cancer, among which mood swings stand out. This is considered an extended period of emotionality that transcends feelings, emotions, and aptitudes in general.1 These are characterized for being temporal, given that they fluctuate according to circumstances; in case of not being intervened on time, they may trigger serious and lasting alterations, which go from elation to severe depression1. Mood disorders occupy the first ranks in mental health globally.2 There are health conditions, like breast cancer, in which women frequently show mood variations, given that they face a world until then unknown and denied, in which they experience a series of emotional alterations.3
The American Psychological Association reports that women with breast cancer may undergo emotional changes with respect to symptoms and treatment. According to estimates, this condition can affect between 20% and 60% of the women with this disease.4) Duck-Hee et al.,5) describe the presence of emotional alterations in 20% to 40% of the women with breast cancer; in addition, they report that North American women with breast cancer have on average moderate levels of these alterations. Likewise, in Taiwanese women with this type of cancer a prevalence of mood disorders was found in up to 19.6% of these women.6 This is coherent with results reported in Australian women who evidenced significant effects of the mood in the long term (λ = 0.829; p = 0.024), with high scores immediately after surgery, but improving at the end of treatment,7 showing that women face emotional crises they manage to control over time. However, another study highlights that the greatest impact occurs during the first year after the diagnosis of breast cancer, a circumstance that can trigger emotional alterations, including bipolar disorder, depression, anxiety, psycho-social difficulties, and emotional stress,8 represented by ambivalence, uncertainty, alteration of self-esteem and body image, fear of recurrence and progressive weakness, or even death.6
Young women with breast cancer and of French origin reported in their emotional dimension the presence of negative affectivity and sensation of cohesion with the partner.9 Among the emotional alterations resulting from this study we can highlight mental health variation, low levels of emotional wellbeing, big difficulties in daily life, symptoms of depression, specific thoughts on the disease, greater threat to their lives, and dissatisfaction with the physical appearance and sexuality.10) Although the literature focuses mainly on women with breast cancer, some studies indicate that between 20% and 30% of men whose spouses endure this disease have emotional alterations characterized by mood swings and depression against the diagnosis and treatment of the women.11
Lagana et al.,11 state that treatment of breast cancer alters life events and generates significant emotional impact on patients and their partners. The emotional repercussions of breast cancer and its treatments, like mastectomy, are transferred and generate mood swings in the spouse,11 that is, suffering, feelings of incapacity to provide support and empathy, adoption of the role of “protective guardian”, isolation in their own feelings -which generates a communication block with the partner-, disability in functions, and difficulty in helping their wives cope with the disease and treatment.12) Distancing and escape-avoidance of the spouses relates to a high level of stress and to symptoms of depression. In addition, Wagner et al.,12 attribute greater emotional stress and problems of the role because of the interruption of their intimate relations, indicating that the partner’s disease affects their lives. According to the information mentioned, the objective of this study was to determine the mood state of women subjected to treatments due to breast cancer and their relationship with the mood state of their spouses, so that this article may contribute to the development of knowledge in the area.
Methods
This was a correlational type, cross-sectional study with quantitative approach and non-probabilistic sampling. To collect the data, an instrument was applied inquiring on the sociodemographic and health variables developed by the authors of this study and by the POMS instrument, version A, by García, Meliá and Balaguer.13 The POMS-A is a self-reported abbreviated scale of 15 items with Likert-type responses (0 = nothing, 1 = somewhat, 2 = moderately, 3 = quite a bit, and 4 = very much). It has five dimensions: depression, vigor, cholera, tension and fatigue. It has significant psychometric tests,13 like Cronbach’s alpha = 0.77 and validity of construct with a report of the total items, which explains approximately 87% of the total variance of the complete 58-item scale. The POMS-A total minimum score is 42 points and total maximum score is 100 points, showing that higher scores indicate higher levels of mood alteration. Due to the study’s rigor, face validity and content validity tests were conducted, demonstrating a content validity index (CVI) of 0.84. Besides, the factor analysis -method of the principal component - evidenced 0.80 in the Kaiser-Meyer-Olkin (KMO) test an acceptable fit of the data to the factor analysis model, while the rotated factor matrix showed load factors > 0.50.
The study involved 103 women who fulfilled the following inclusion criteria: a) having just finished treatment for breast cancer (surgery/chemotherapy/radiotherapy) - up to a maximum of five years, with healing prognosis or relapse; b) being between 25 and 64 years of age; c) not having psychiatric alterations confirmed through medical diagnosis prior to the breast cancer; d) acceptance of their spouses to participate. For this study, the spouse is the person with whom the woman who has undergone treatment for breast cancer maintains a close and mutually satisfying relation, characterized by permitting to experience and express feelings, communicate interests, opinions, needs, and share physical intimacy.14 The study permitted including homosexual and heterosexual couples; however, the sample was comprised of heterosexual couples. Exclusion criteria involved being sex workers, given that this condition can interfere in the sexual health reported by the women. These criteria were verified through the socio-demographic and health instrument filled out by each participant.
The sample was collected over a 16-month period during 2010 and 2011, in different foundations for support to women with breast cancer located in the cities of Ibagué, Cali, Medellín, Bogotá D.C., and Cartagena (Colombia). The collection took place in different cities to achieve higher characterization of the mood state in the Colombian population and to cover a higher number of women who complied with the criterion of having a spouse. The Ethics Committee of the Faculty of Nursing at Universidad Nacional de Colombia approved the study. Commitment contracts were signed with each of the foundations; complying with requirements, like socialization of the results and some educational sessions. Via telephone calls from each foundation the couples were asked to participate, each of which signed the informed consent. The information was collected in places that offered privacy, located in the institution’s offices or in the homes of the participants, with prior agreement on an appointment. This depended on time available and on the preferences of the participants.
After applying the instrument, a database was elaborated and the analysis was performed in the SPSS statistical software (version 19). Descriptive statistics and inferential statistics were applied regarding frequency, percentages, means, and standard deviation (SD). The Kolmogorov-Smirnov test showed normal distribution in the total of the mood variable. The parametric t test was applied for two independent samples with respect to means, with p = 0.354, higher than the significance level (0.05), concluding that it is not possible to reject the null hypothesis, that is, it was determined that significant differences do not exist between the average mood of the women and that of their spouses. The subscales presented abnormal distribution. The Mann-Whitney U test was applied to the subscales, reporting p < 0.05 in the Tension (p = 0.35) and Cholera (p = 0.025) subscales, showing that it is possible to reject the null hypothesis. That is, according to the data reported in the test, differences were found between tension and cholera within the couple, while the Depression, Vigor, and Fatigue subscales do not show differences in the dyad.
Results
In this study, 39% of the couples participating were selected in Medellín, Colombia. Among the sociodemographic characteristics of the couples (Table 1), prevalence was noted in married marital status (69%), socioeconomic levels three and four (47.5%), and average time of sharing in the relationship was 20.5 ± 11.3 years (41.8% with more than 21 years).
Table 1 Sociodemographic characteristics of the 103 women with breast cancer and of their spouses
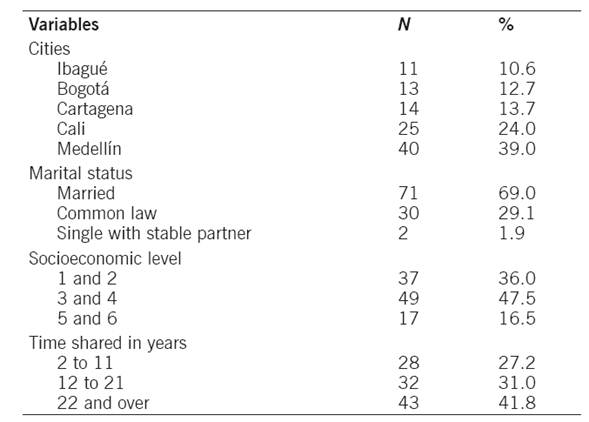
The mean age in the group of women was 48 ± 8.5 years (minimum of 28, maximum of 64) and of their spouses, it was 51 ± 11.3 years (minimum of 20, maximum of 79).
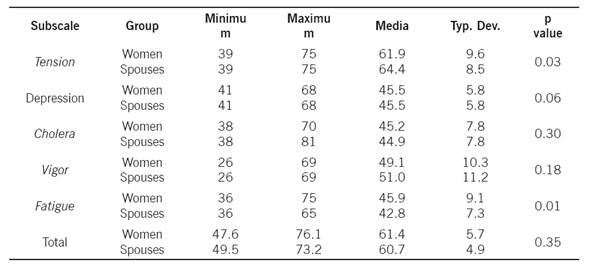
Regarding the time of the women’s treatment termination, it ranged between 1 and 60 months, close to 48% had less than one year, 28% from one to three years, and the remaining 24% had four and more years. A total of 73.8% of the participants received three or more treatments combined to manage breast cancer, like surgery, chemotherapy, radiotherapy, and hormone therapy. None of the women or their spouses presented mental health alterations prior to the diagnosis of breast cancer. The mood level of women reported a mean of 61.4 ± 5.7, versus 60.7 ± 4.9 in the spouses, a difference that was not statistically significant.
Upon analyzing the score of the mood subscales, it was noted that statistically significant differences were only found in the Tension and Fatigue subscales. In the first, the average score was higher in the spouses; in the latter, the higher score was found in women (Table 2). In addition, the existence of a mean positive correlation of 0.5 (p <0.001) was determined between the women’s mood with respect to that of their sexual partners, which indicated that better mood in the women also meant better mood in their spouses.
Discussion
This study found a mean score of 61.4 in women and 60.7 in men, which, without this being a significant difference, revealed a high alteration of mood in couples. The findings in the women agree with the study reported by Gao et al.,15 who state that emotional alterations can persist until after the treatment in 50% of these individuals. Lagana et al., 11 in turn, indicate that the spouses of these women presented emotional impairment.
Emotional commitment is high in the group of Colombian couples from this research, which is characterized for having a broad age range (women: 24-64 years; spouses: 20-79 years), an aspect that can differ from studies that highlight youth (under 40 years of age) as a risk factor for emotional alterations.10 Also, although this study did not consider indicating the relationship between marital status and mood, it should be clarified that being married was most prevalent in the sample (69%) versus common law (29%), a fact that, according Giraldo,14 in the Colombian culture subscale does not seem to have significant differences in the development of the couple’s life among those married and those living in common law.
In this study, mood level alterations experienced by the dyads, especially in the Depression, Cholera, and Vigor subscales account for very close mean values, which is why it is possible that values from the previous subscales have this behavior, given that spouses are an integral part of the women’s emotional performance. Likewise, they constitute one of the principal sources of emotional support, given that by living together they share the effects of the treatments, which is confirmed by Salonen et al.,16 who found up to 77% support from their partners in Finnish women with breast cancer.
For the women in this study, the condition of having a partner is a fundamental aspect for their mood. Literature reports that women who communicate with their partners are less labile to emotional alterations, like anxiety, depression and stress.10 Nevertheless, it is interesting herein that, although the women have partners, they have a high average (61.4) of negative mood, possibly related to specific situations upon ending the treatments, like psycho-social difficulties, emotional stress, ambivalence, uncertainty, anxiety of survivors in the transition from active treatment, alteration of self-esteem and body image, depression, fear of recurrence, progressive weakness, or death.6,10)
Another factor contemplated in this study was the occurrence of significant differences among the means of the Tension and Fatigue subscales for the women and their spouses, respectively. This aspect demonstrates that although the couple presents changes in levels of tension and fatigue, their behavior can vary in each of them: tension is higher in the spouses, while fatigue is higher in the women. It would be necessary to delve into these couples if over time this condition can be overcome, as expressed by Webber et al.7) With respect to the higher fatigue average in women than in their spouses, this result is coherent with that documented in literature, which highlights fatigue in women as consequence of the effects of the treatment that - in turn - impact upon the emotional dimension.11
From the correlation, the mood of women and of their spouses has a significantly positive relationship, which shows how a person’s mood level affects the couple.11 This finding guides nursing care interventions aimed at the dyads to improve, or maintain mood at positive levels, so that women obtain greater support from their spouses, as proposed by the American Psychological Association.4 Thus, our results are determinant because they permit broadening knowledge in so far as they statistically validate the mood levels of couples, agreeing with that stated by Huston and Burgess -retaken by Giraldo,15 who conclude that due to the couple’s condition, we may lead “on the one hand, to the process of interaction to take place with greater frequency within a range of circumstances, and in this case they are linked to the situation faced by women with breast cancer. On the other hand, investment on the relationship grows, increasing its importance in the partner’s life and the feeling that their personal interest is tied to the wellbeing of the relationship or, on the contrary, ʻthe partner can be affected’.16)
To conclude, it is highlighted that women and their spouses present mood alterations. The Tension and Fatigue subscales, although affecting the couple, their means differ significantly, while the Depression, Cholera and Vigor subscales show very close values. Additionally, it was statistically proven that as the negative mood increases in the woman, it likewise increases in her spouse. According to the methodology, this study approached couples from different regions of the country, permitting to obtain an important sample.
The results from this study should help to guide the development of an innovative practice, which promotes care and self-care in virtue of preventing and controlling mood alterations in couples confronting breast cancer. From the investigation, we seek the development of interventions and impact indicators that promote improving the mood state. It is important to conduct future longitudinal studies to inquire on the mood swings confronted by women and their spouses from the diagnosis phase to the post-treatment phase in individuals with different types of cancer. Similarly, it is necessary to validate interventions to promote the emotional wellbeing of women with breast cancer and which include participation from their spouses. As a study limitation, we found underreporting of information about women with cancer and of their spouses, as well as the lack of follow-up programs with updated databases, which prevented randomizing the sample.
Acknowledgments. The authors thank Universidad Nacional de Colombia and the Colombian Institute for the Development of Science and Technology (COLCIENCIAS) for their support in the development of this research. Gratitude is also expressed to the couples who shared their emotional experiences.

