











 text in
text in  English (pdf)
English (pdf)
 Article in xml format
Article in xml format Article references
Article references
 Send this article by e-mail
Send this article by e-mail Cited by SciELO
Cited by SciELO  Cited by Google
Cited by Google  Similars in
SciELO
Similars in
SciELO  Similars in Google
Similars in Google 
 Permalink
PermalinkIntroduction
Management of Chronic Diseases (CD) lacks attention and analysis worldwide. Many professionals develop models to minimize the impact of these diseases on people's health, as they are multifactorial conditions that impose requirements on patients, their families and the health system. The care of most of the CD include comparable and effective management strategies, so that similarities start to overlap differences.1 Patients with CD need support in their community to maintain good health. They lack skills for self-management, and thus, health teams must provide planned and integrated care and treatment to meet their needs and assist them in early detection of signs and symptoms to avoid evolving the disease to an acute exacerbate state.1 For this to be possible, professionals must acquire specific skills, and health services should work in interconnected, structured and organized through attention models or care models. These consist of careful logical systems that communicate, articulate and bind in a unique way the relationship between the population and its subpopulations divided by risk, interventions and health outbreaks interference.2,3
The Chronic Care Model (CCM) and the Innovative Care for Chronic Conditions (ICCC) stand out among models for CD. The first was introduced by a North American Institute in mid-1990 in order to transform care through a combination of elements such as health staff, self-management and decision support, and use of information and recording technologies.4 The ICCC derived from the above was developed by the World Health Organization and is based on the belief that outcomes for chronic conditions are achieved when patients and family members are motivated and informed and health professionals work together.5 These and other models have been created due to the need for changing the management of CD. They have the purpose of determining what actions and practices are adequate, respecting the peculiarities of their care. Thus, it is understood that there are some care concepts that have become part of the health discourse with the increased prevalence of CD worldwide, such as self-care management and case management (case management and operation are used interchangeably). Given the impact of CD and the need for life-long treatment and monitoring, these diseases require a new approach, such as the models of care. Thus, the present study aims to identify care models and their impact in the care of patients with CD published in literature from 2000 to 2014.
Methods
This is an integrative review, which allows summarizing studies approaching the selected theme, contributing to the understanding of problems and providing information for evidence-based practice. To guide this integrative literature review, a formal and rigid work structure based on a previously developed and validated research protocol was included.6 The following steps were defined: identification of the theme and definition of the guiding question; establishment of inclusion and exclusion criteria of articles; approximation of material based in common characteristics; analysis and discussion of results, identification of differences and conflicts, and presentation of results. The main question of this study was: What care models are used to assist patients with chronic diseases and what are the impacts of their application? The databases searched were the directory of the Virtual Health Library (VHL), the Latin American and Caribbean Health Sciences (LILACS), Medical Literature Analysis and Retrieval System Online (MEDLINE), Spanish Bibliographical Index on Health Sciences (IBECS), and Nursing Database (BDENF).
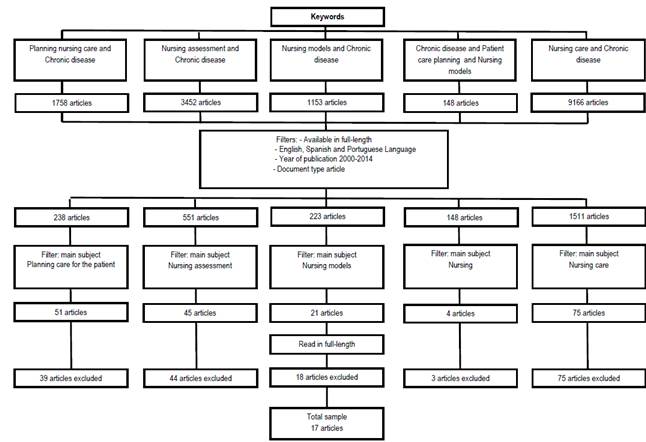
The search took place from May through June 2014, using the following controlled and non-controlled and associated descriptors: "models of care AND chronic disease", "nursing care AND chronic disease", "nursing assessment AND chronic disease", "patient care planning AND chronic disease" and "chronic disease AND patient care planning AND nursing models". This resulted in gathering a total of 15677 articles. Inclusion criteria were: articles available in full-length for free, in Portuguese, English and Spanish, published from 2000 to 2014. This resulted in 2,671 articles, for which the main subject filters were applied, reducing the number to 196 articles. These were submitted to exhaustive reading in full-length, independently, to ensure rigor while selecting those articles contemplating the guiding question. Exclusion criteria were: articles with population or sample composed of children or patients with chronic wounds and articles repeated in different databases. After applying these criteria, 17 articles remained (Figure 1).
The aspects identified in the articles selected were: title, authors, publication year, journal, keywords, objective(s), methodology, results and the type of care model. Data were pooled from qualitative analysis, which identified the similarities; Thus, there were three categories: "Health costs"; "Model-based care experience" and "Patient autonomy".
Results
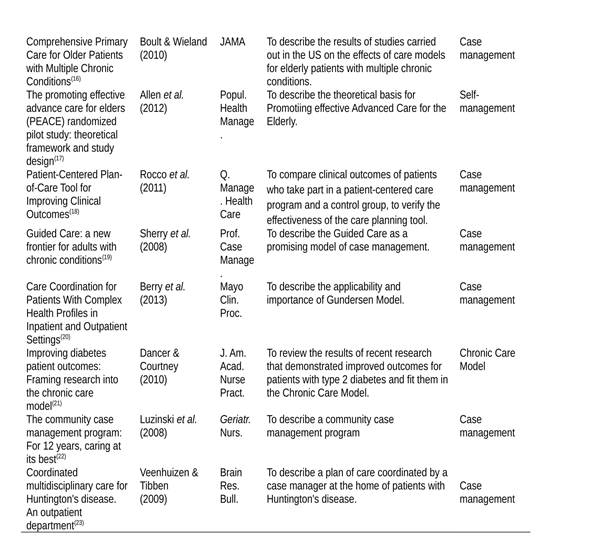
The sample included 17 articles, all published in international journals in English and in the MEDLINE database. Among journals, seven are Nursing journals, seven are Medical journals, one involves both areas, and two are interdisciplinary. Most articles (12) had "Planning Assistance AND Chronic Disease" as descriptor. No article was included with the keywords "Nursing care AND chronic disease". As for the year of publication, seven were published in 2008 and four in 2012. The CD addressed in the articles represent numerous areas such as genetic, psychiatric, musculoskeletal, metabolic, cardiovascular disorders, among others. Regarding care models exposed in the studies, nine were of the case management model type, six were of the self-management model type, and two were CCM. The evaluation of results led to clustering converging issues, from which three categories derived. These are entitled "Costs for the Health System"; "Model-based care experience" and "autonomy of the patient". In the first and third category, articles covering the case management model predominated, and in the second model, self-management predominated (Table 1).
Discussion
One of the models used for care is the case management. This is a strategy that health services and social services use to support patients in their care, and that can result in the organization of a care plan in the form of a document with definition of agreed goals.7 This model is also understood as a process of cooperation between a health professional, the patient with complex conditions and the social support network, to plan, monitor and evaluate care alternatives, in order to provide a qualified care, that may increase the functional ability and preserve the individual and family autonomy.5
The English Department of Health seeks a care planning based on case management. In this model, the person with a chronic condition comes into contact with the nurse or other health professional, discusses his care plan, implement it in written or electronic form (via email) and schedules a new meeting to review goals. This planning allows shared decisions, supports the patient to manage his condition and promotes care based on scientific literature.7 In North American countries, there are case management programs adopted by health insurance companies, such as Guided Care, Geriatric Resources for Assessment and Care of Elders (GRACE), Program of All-Inclusive Care for the Elderly (PACE), among others. All these are models used in primary care and make the development of a comprehensive care plan possible, incorporating protocols based on evidence, the implementation of a long term care plan, proactive monitoring of the patient's clinical status, adherence to the care plan, and coordination of primary care in hospitals and emergency services.16
Another case management used in the United States by the health insurance companies is the Gundersen. This calls for improved communication between health professionals and patients in order to make them partners in the decisions taken on their care and in the pursue of better health conditions.10 It was observed in a Brazilian study that the planning of care used as a tool served as a guide to record goals and to facilitate the case management. It was found that when guidelines are agreed between patients and professionals, and recorded, this helps to give continuity to the care in the homes.24 Self-management is considered another model of care that is associated with teaching skills for problem solving. Its purposes are to incite changes in behavior, to teach the patient to recognize signs and symptoms of exacerbation of the disease and act before these.25 An example of this model is the 4G, in which the health professional distributes information and guide self-management, in identifying the problem and of habits and lifestyle changes necessary. This takes place in three stages: meeting, generation and conduction. At first, the patient analyzes his situation through the five W, What? When? Where? Who? Why? and questions the impact of this in his life. Then, the professional helps the patient to understand the problem and to set medium-term goals, acting as a guide in the evaluation and review of such goals.11
Another self-management program is the Carelink. This was designed to assist the elderly in self-management of chronic conditions, with home visits, nursing interventions, health education and continuous monitoring. Nursing students, in partnership with communities, conduct training activities to promote and maintain health.22 In addition to case management and self-management, the CCM, developed by Wagner et al.26 assists in chronic situations of high prevalence and in the failure of systems to take care of them. The objective is to turn the daily care for patients with CD into something preventive and proactive by combining planned actions with community support, integrated decision and records, to promote teamwork and patient autonomy.4,15
To identify the impact of these models, the first category "Costs to the health system" refers to the use of the health care models by professionals in order to reduce financial costs of CD. Studies carried out with health insurance companies in North-America that adopt some case management and self-management programs showed that such companies reduced by 23% their cost by avoiding conducting unnecessary hospital care, which are performed in homes. When programs are not used, this results in 75% more costs for the health system.16,19,20 The second category "Care experience based on a model" refers to the accounts on the experience of being assisted based on case management and self-management. One study found that when patients are assisted based on case management, they felt surprised and were not familiar with the term "care planning".7 Other studies reported that case management can improve the quality of communication between the health team and patients and help to satisfy those involved in the experience of care, whether doctors, patients or families.8,16,19 The use of the GRACE and PACE models and Gundersen program, patients reported receiving more information about their conditions, they had fewer needs that were not cared for, and the last aspect led to change the outbreak of the disease for the patient.16,20
A trial with bipolar affective disorder patients tested the case management and noted that patients whose care was performed with this model showed improved physical and mental health quality when compared to the usual care group. In the case of applying the Carelink model, it was found that the patient started to manage his illness safely and effectively and had no readmissions in the period.9,22 The last category "Autonomy of the patient" concerns the role of the patient in making choices before the guidelines provided by the health team. Therefore, the will of one will prevail over the other, as exemplified in the case study that employed a home care plan for two patients who had Huntington's disease. One of them reported satisfaction with the care and returned to his work and leisure activities while the other refused to follow the guidance provided and his choice was respected.23
Conclusions.
The use of case management model predominated and as benefits were found the close relation between patients and professionals, patients' autonomy, reduced expenses to individuals and health systems. We emphasize the importance of using these models in Brazil, since there was no national study included in this work. Thus, we suggest that health professionals share their experiences in the application and/or creation of other care models adapted to the Brazilian reality with a view to incentive the active participation of nurses in the use of these new technologies that can be applied in the care of chronically ill patients.

