











 text in
text in  English (pdf)
English (pdf)
 Article in xml format
Article in xml format Article references
Article references
 Send this article by e-mail
Send this article by e-mail Cited by SciELO
Cited by SciELO  Cited by Google
Cited by Google  Similars in
SciELO
Similars in
SciELO  Similars in Google
Similars in Google 
 Permalink
PermalinkIntroduction
Health promotion consists in providing people the necessary means to improve their health and exert greater control over it. To reach an adequate state of physical, mental, and social wellbeing, an individual or group must be able to identify and carry out its aspirations, satisfy its needs, and change the environment or adapt to it.1) Within the labor context, Health Promotion in the Work Place (HPWP) includes a variety of policies and activities in the work area designed to increase control and improve the health of employers and employees at all levels.2 Likewise, HPWP implies achieving quality of life in work scenarios, considering the consequences that the conditions appertaining to the labor activity generate upon workers within their different spheres: family, social, political, economic.3 Similarly, this constitutes a strategy to study the health of workers in their work environments within a comprehensive approach to have a greater impact on the quality of life of the individuals.4
Work and work environments, as well as habits and life routines, bear an effect upon the health, security, and wellbeing of workers. Healthy workers tend to improve their work environment through relationships with their colleges and their supervisors or subordinates, which leads to improving the quality of work.5 This relationship between health and labor quality is quite important to foster a culture of prevention within organizations and favor the adoption of a health-promoting lifestyle. Work conditions and the form of labor organization that seeks greater productivity, efficiency, and competitiveness based on producing high-quality goods and services have caused workers to be subjected to excessive effort to satisfy market demands and exigencies, leading man to live for work, which has - in many cases - made employees neglect their physical and mental health. This, in turn, has promoted in workers a more sedentary life with scant opportunities for relaxation and recreation, which is reflected in inadequate work performance.6
Added to the aforementioned, there is the worrisome situation of chronic non-communicable diseases related to unhealthy lifestyles in workers. Statistics in this regard indicate that annually 17.3-million people die due to cardiovascular diseases; 7.6-million due to cancer; 4.2-million due to respiratory diseases; and 1.3-million due to diabetes mellitus.7-9) Said ailments not only affect the quality of life of workers and their families, but also reduce their productivity and increase health costs, thus, compromising the country’s development. Studies with workers with respect to overweight and obesity conditions reported a prevalence of 34% in university students10 and 55% in administrative, manual, technical, and directive workers.11 Another study reported 85% sedentary habits and 41% cigarette consumption among construction workers.9 Regarding consumption of foods with an excess of calories, a prevalence is reported at 40% among workers from the health sector.8
Health in the workplace is a social commitment, with employers being the main agents responsible for providing the warranty to conduct and execute diverse labor functions in the best conditions to guarantee not only good work, but also for the work to be done not to affect at a given moment the physical and mental health of workers.6) Within the academic context, the healthy university proposal has as a base a concept of integral health, which is a product of the internal and external harmonious relations individuals manage to maintain with themselves, with the rest, and with the environment.12) A health promoting or healthy university is defined as that which incorporates health promotion onto its educational and labor project to propitiate human development and improve the quality of life of those who study or work there.13 Therein, a healthy university is that which conducts sustained actions aimed at promoting the integral health of the university community, acting upon the social and physical environment, as well as on the formation of healthy lifestyles.12 Its implementation is founded on the public health policies of every country, under the entry of health promotion, hence, its study can encompass the themes of responsibility of health, physical activity, nutrition, spiritual development, interpersonal relations, and stress management as dimensions of the health-promoting lifestyle.
In the specific case of the university workers, it is known that they constantly relate to other people; often, distressing and conflictive situations are derived from these relations, which are strong generators of stress and can obstruct work performance,14 therein, it is important to include the study of psychosocial variables, which is the case of labor assertiveness defined as a conduct of self-affirmation within the work context.15) According to Arredondo,16 assertive professionals permit obtaining benefits in the personal area by increasing their self-esteem, personal security, self-image, and self-concept, as in the work area by diminishing the number of stressful situations and increasing efficacy, quality, and competence in the services offered. Hence, assertiveness must be a characteristic or personality trait that employees must have or develop to remain at their work posts and above all adapt to diverse changes and provide an optimal response to what the environment offers day to day.
Universidad Autónoma de Guerrero (UAGro), in its collective labor contract for 2015-2016,17 establishes that the Joint Mixed Commission on Health, Hygiene, Safety, and the Environment in the workplace, responsible for permanently overseeing work conditions in all the dependencies at UAGro to determine the working conditions of risk for the health of workers, will identify and justify, through a study, which are the work centers that represent risks to them, will dictate the implementation of prevention and/or correction measures and, when warranted, provision of adequate protection equipment to carry out their assigned academic activities. Likewise, in the Institutional Development Plan (PDI) 2013-2017,18 UAGro promotes the culture of health in university students through sports.
On its part, the Nursing Academic Unit N° 1 and 2 (UAEnf. 1 and 2), through the Joint Mixed Sub-commission on Health, Hygiene, Safety, and the Environment in the workplace conducts health promotion of workers; in addition, the Sub-direction of Integration of Substantive Functions promotes the culture for health through sports, music, dance, and social coexistence among students, professors, and administrative personnel. Likewise, other sections have been involved for intra- and extra-mural participation in these events. In spite of these initiatives, university workers at UAEnf. 1 and 2 endure chronic-degenerative diseases triggered by sedentary habits, smoking, alcoholism, obesity, and violence, among others, which lessen the quality of health of the workers.
This project is part of one of the strategies on prevention and health promotion contemplated within the vision and strategic direction of the 2013-2017 Institutional Development Plan,19 at UAEnf. 1 and 2. This shows evidence of the health-promoting lifestyle of workers and, consequently, the bases to develop specific programs to improve the work environment, propitiating the comprehensive development of its workers to favor productivity and quality in the workplace, as well as the health of the university students and staff. This permits broadening understanding around the perception of workers’ health conditions, of risks, and evidence of disease processes and allows having a diagnosis on lifestyles of its workers to underpin the design of interventions that favor the health of its members, besides strengthening its vision as a sustainable university. The aim of this study was to analyze the health-promoting lifestyle and assertiveness variables and their relation to the health condition in university workers.
Methods
A cross-sectional study was conducted, which described the health-promoting lifestyle, assertiveness, and health condition variables of university workers. Likewise, the relations among these variables were studied. The universe was made up of workers from the Nursing Academic Units No. 1 and 2 from Universidad Autónoma de Guerrero (México); data was collected from August to December 2015; all (100%) of the active workers participated in the study (n=112).
To gather the sociodemographic information, a form was designed containing sociodemographic information (age, gender, marital status, and level of education), work information (shift, area, and post), personal background, anthropometric data (body mass index (BMI) and waist circumference), blood pressure (BP), and capillary glycemia. The health-promoting lifestyle variable was measured by using the Spanish version of the health-promoting lifestyle questionnaire (PEPS II),19 comprised of 52 items with Likert-type response scale: 1 = never, 2 = some times, 3 = frequently, 4 = routinely. The scale is made up of six subscales: responsibility for health (9 items = 33, 3, 51, 15, 21, 39, 27, 9, 45), physical activity (8 items = 4, 10, 16, 22, 28, 34, 40, 46), nutrition (9 items = 2, 8, 14, 20, 26, 32, 38, 44, 50), spiritual development (9 items = 6, 12, 18, 24, 30, 36, 42, 48, 52) interpersonal relations (9 items = 1, 7, 13, 19, 25, 31, 37, 43, 49), and stress management (8 items = 5, 11, 17, 23, 29, 35, 41, 47); the range of scores to obtain is from 52 to 208 points, this score was converted to index (values between 0 and 100 points), indicating that a higher index reflects better lifestyle. The authors of the instrument reported reliability of 0.94 in the total scale and for the dimensions from 0.79 to 0.94.
In relation to the measurement of the assertiveness variable, the study used the Assertiveness Questionnaire (AQ) by Lazarus and Folkman,20) which contains 20 statements. The instrument was designed for self-administration, evaluating through self-report the social behavior of individuals (two dimensions: assertiveness and non-assertiveness), exploring their responses in varied situations of social interaction, according to a dichotomous response (yes/no). Its correction is carried out by adding the responses given in each column (Assertive response: Yes in items 1,4,5,6,9,12,13,14,15,16,17,18,19,20, and No in items 2,3,7,8,10,11/ Non-assertive response: NO in items 1,4,5,6,9,12,13,14,15,16,17,18,19,20, and Yes in items 2,3,7,8,10,11), obtaining two scores, one for each column, which indicates that a higher score in the column of assertive responses means higher assertiveness. The authors of the questionnaire reported reliability of 0.6.
Data analysis was performed by using the statistical program for social sciences - SPSS, version 17. Frequencies, proportions, and percentages were obtained for the categorical variables and for the numerical variables measures of central tendency and variability were calculated. Additionally, the Kolmogorov-Smirnov goodness-of-fit test was carried out with correction by Lilliefors to contrast the normality hypothesis in the distribution of the continuous variables, which is why parametric tests were applied. This research adhered to the ethical principles in the Regulations of the General Health Legislation on Health Research.21 Participation was voluntarily and signed informed consent was obtained from the participants; the study was approve by the authorities of the Nursing Academic Units No. 1 and 2 from Universidad Autónoma de Guerrero.
Results
The reliability test of the instruments used in this study was established through the Cronbach’s alpha and Kuder Richardson coefficient values. In this study, the PEPS II and AQ instruments showed an internal consistency of 0.9 and 0.6, respectively. In terms of the sociodemographic characteristics of the participants, women prevailed (61.6%); married marital status (58.9%); participant age ranged between 24 and 72 years with a mean of 45.4±12.2 years. Of all the participants, 68.8% belonged to the Nursing Academic Unit No. 2; as far as level of education, 63.4% had graduate degree; 24% undergraduate degree; 8.1% high school; and 4.5% basic education; in addition, 49.1% worked the day shift, 69.6% worked as teaching staff, 18.8% as administrative staff, and 11.6% in general services.
With respect to the health condition of the participants, 74.1% of them had no health problem; however, 17% had a medical diagnosis of high blood pressure, 4.5% had type II diabetes mellitus, and 4.5% suffered both diseases. Regarding BMI, overweight condition was noted in 46.4% and obesity in 22.2% (Grade I = 20.5%, Grades II and III = 1.7%). Table 1 shows the results of the general index of health-promoting lifestyle and by its dimensions, as well as the assertiveness index, where the dimensions with the highest indices were spiritual development and interpersonal relations. The general index of health-promoting lifestyle corresponds to a medium level and that of assertiveness to a high level.
Table 1 Central tendency measurements of the indices per dimensions of the health-promoting lifestyle and assertiveness

Table 2 shows the percentages of assertive and non-assertive responses for each of the items from the Assertiveness Questionnaire, where the participants have an assertive tendency by obtaining higher scores in the assertive responses column, except in questions 1, 2, 7, and 8 that have a lower percentage of assertive responses.
Table 2 Percentage of assertive and non-assertive responses for each reactive of the Assertiveness Questionnaire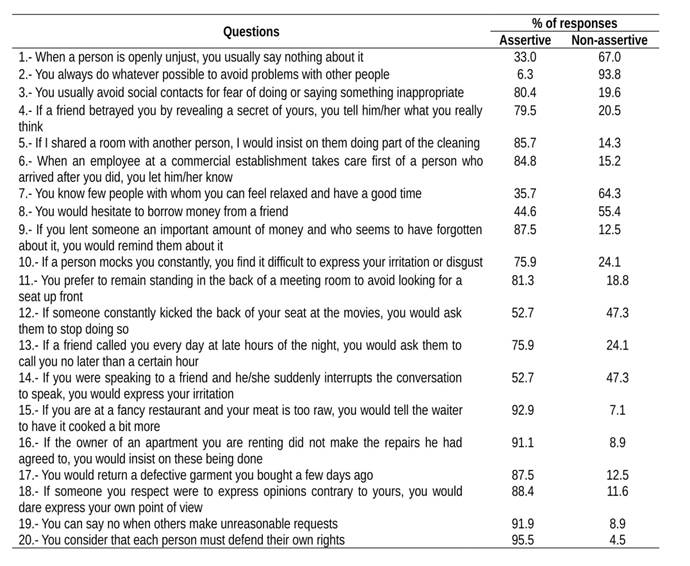
Upon evaluating the correlation among the dimensions of the general index of the health-promoting lifestyle, assertiveness, and some health condition variables, a positive and statistically significant relation was found among assertiveness and: the total score of the health-promoting lifestyle questionnaire (r = 0.22, p <0.05) and the dimensions of spiritual development (r = 0.35, p <0.01) and of interpersonal relations (r = 0.29, p <0.01). From the health condition parameters, glucose was inversely related to the total score of health-promoting lifestyle (r = -0.20, p <0.05) and the dimensions of physical activity (r = -0.24, p <0.01) and stress management (r = -0.24, p <0.01). As per the difference of health-promoting lifestyle by gender, this was statistically significant (t = 2.99, p <0.05), women had a higher (41.17) mean than men (36.03) and in self-esteem it was not statistically significant (t = 0.51, p >0.05), the mean in men (59.76) as in women (58.62) were similar. The relationship between the age variable and the health-promoting lifestyle (r = 0.07, p >0.05) and self-esteem (r = -0.15, p >0.05) were not statistically significant.
Discussion
The results obtained from the reliability test of the Assertiveness Questionnaire are considered accepted, given that Tavakol and Dennick22 describe that reliability coefficients >0.70 are satisfactory in most cases; nevertheless, some circumstances will require a higher score or will consider a lower score acceptable. Additionally, it is worth mentioning that given the cultural diversity of the Mexican population in its urban and rural zones, it is deemed convenient for this instrument to be applied and used for other research to test its reliability in other contexts.
In reference to the variables measured in the health condition, seven of every ten participants do not have health problems. The proportion of overweight condition found in this population (four of every ten) was higher than the national mean (three of every ten), and that of obesity (two of every ten) was lower than the national mean (four of every ten). With respect to the values found for hypertension (17%) and obesity (4.5%), these are lower than the national values (hypertension 64.1%; diabetes 9.2%).23
Regarding the results from the general index of health-promoting lifestyle, (mean = 39.2) corresponds to a medium level; this data was similar to that reported in another study in healthy adults who obtained a good score24) and that of assertiveness (mean = 74.5) at a high level, this was different from the results reported in workers who evidence assertiveness deficit.25) Results of the correlation among assertiveness and the health-promoting lifestyle and the dimensions of spiritual development and interpersonal relations were positive and statistically significant, indicating that higher assertiveness goes in hand with greater health-promoting lifestyle, spiritual development, and interpersonal relations. This is because when workers have higher levels of assertiveness, they make better decisions with respect to conducts that favor their health-promoting lifestyle.26 In addition, glucose - as a parameter of the health condition - was inversely related to the health-promoting lifestyle and to the dimensions of physical activity and stress management, that is, with higher levels of glucose there is worsened health-promoting lifestyle, physical activity, and stress management. In this regard, related studies report that exercising improves peripheral resistance to insulin.27
To conclude, the study permitted demonstrating the relationship between the health-promoting lifestyle and assertiveness in the university workers studied, which justifies the design of educational interventions from nursing aimed at improving these aspects. In light of the study’s results, the need is evident to carry out prevention and health promotion actions, directed at this population group from the multidisciplinary approach. Within this context, the nursing professional’s role becomes relevant as health promoter, a position that grants them the necessary elements to contribute to improving the health and quality of life of this population by implementing actions aimed at providing workers the skills to maintain a health-promoting lifestyle and develop personal self-affirmation (assertiveness) conducts that allow them to improve the self-care practices of their health.

