











 text in
text in  English (pdf)
English (pdf)
 Article in xml format
Article in xml format Article references
Article references
 Send this article by e-mail
Send this article by e-mail Cited by SciELO
Cited by SciELO  Cited by Google
Cited by Google  Similars in
SciELO
Similars in
SciELO  Similars in Google
Similars in Google 
 Permalink
PermalinkIntroduction
Chronic Non-Transmittable Diseases (CNTD) are characterized by a set of diseases, such as cardiovascular disease, obesity, diabetes, cancer, chronic respiratory diseases and neuropsychiatric disorders. With the increase in the ageing population and life expectancy in Brazil, these diseases are prevalent in the mortality statistics, with 63% of the deaths in the world and 72% in Brazil. 1 The CNTD are directly related to social determinants, such as modifiable risk factors like gender, genetics, and age; and the modifiable risk factors such as smoking, alcohol, physical inactivity, and unhealthy foods. These can lead to intermediate risk factors such as hypertension, hyperlipidemia, overweight, obesity, and glucose intolerance, with outcomes in coronary diseases, cerebrovascular disease, peripheral vascular disease, chronic kidney disease, diabetes, chronic obstructive pulmonary disease, emphysema, cancers, and psychological problems.1-3) With the chronic diseases and their consequences, reducing life expectancy and increasing spending to the public health sector in rehabilitation, so there is an interest in monitoring the epidemics with control and prevention mechanisms in Brazil and in the world. 2 The detection form is the individual nutritional assessment based on medical records, nutrition, medications, physical, biochemical, and anthropometric data in order to identify or confirm the existence of risk for a nutritional disease process, such as obesity and dyslipidemia. Thus, the early identification of risks and guidelines involving dietary, anthropometric and biochemical data by the health team can promote health, rehabilitation and encourage healthy habits.4
In Brazil, there was established the Strategic Action Plan for Facing the CNTD in Brazil (2011-2022), aiming to promote the development of effective public policies for preventing and controlling the CNTD,2 being accomplished primarily in the Primary Health Care (PHC), consolidated through the government program for Family Health Strategy (FHS), which act on health promotion, disease prevention, diagnosis, treatment of the most prevalent health problems and personal recovery of the entire population. The clients in this system are mostly children and middle-aged and elderly women, while men are generally elderly with already-installed chronic diseases.3 The main professional involved in these activities, is the nurse and nursing team, which is responsible for assisting, preventing and promoting self-care, assuming the responsibility for continuity of cares along all life time. When comparing men and women, in Brazil, some studies have been showing parameters that show risk for developing cardiovascular disease in both genders. In women, there is a larger index of abdominal obesity, physical inactivity and diabetes, while in men the consumption of tobacco, alcohol, inadequate diet and overweight, hypertension and dyslipidemias prevail, thus there is no difference in both genders.1,3 Demonstrating the need for promotion and prevention to control the development of cardiovascular diseases mainly in modifiable risk factors, primarily with stimulation of physical activity for women and social habits changes for men. In this context, the main objective of this study was to evaluate the current state of health in the population of young women, adults, and elderly in a Basic Health Unit in Londrina, Paraná, Brazil, raising the risk factors that predispose to the development of cardiovascular disease.
Methods
Research. This study is characterized as observational and descriptive, with quantitative analysis. The study's subjects were 60 women over 18-year old, with appointment in a Basic Health Unit (BHU) for medical consultation, medical monitoring and nursing care, in Londrina, Paraná, Brazil. For ends of analysis and comparison, the subjects in the research had been distributed in three groups of 20 women each, being the age groups: 18 to 39 years, 40 to 59 years and equal or above of 60-year old. The subjects had been selected by simple random sampling on categorical variable and the number of subjects was determined through statistical calculation, using the following parameters: population (p) of the municipality of Londrina, normal standardized variable (Z) associated with the confidence level (90%), real event probability (p) and sampling error (e) (10%). The formula used for the calculated sample (n) was n=N.Z2. p.(1-p)/Z2. p.(1-p) + e2. (N-1).
Data collection. Data collection took place between February to November 2014, at the BHU itself, by means of a structured questionnaire with the help of mHealth Data Collector (mHDC)4 software via a mobile device, where data was gathered, stored, and transported to the researcher's email in the tabular form. The questionnaire included the following items: a) personal data form; b) anthropometric data; c) biologic data; d) daily habits, and; e) previous illnesses. For anthropometric data collection, such as Body Mass Index (BMI), Waist Hip Ratio (WHR) and Body Fat Percentage, anthropometric scale, Toledo® brand, anthropometric tape, and Cescorf® brand adipometer, were used. As far as WHR measuring tape was placed at the midpoint between the costal edge bottom and the iliac crest and the skin folds were vertical triceps, diagonal subscapular, diagonal suprailiac, and horizontal abdomen.5 In order to check the blood pressure, a sphygmomanometer, and stethoscope were used, Premium® brand. The classification of the parameters for BMI was 18.5 to 24.99 (normal), 25 to 29.99 (overweight), 30 to 34.99 (level I obesity), 35 to 39.99 (level II obesity) and >40 (level III obesity). For WHR the following were classified as low (<0.74), moderate (0.74 to 0.81), high (0.82 to 0.88) and very high (>0.88). For the Body Fat Percentage, the following were rated as average (15 to 22%), above the average (23 to 29%) and obese (≥ 30%).5 Blood pressure was checked after the subjects has been resting for 10 minutes. The following were classified as systolic blood pressure normal (<120 mmHg), borderline (130-139 mmHg) and normal (>140 mmHg). For diastolic blood pressure the metrics were considered normal (<80 mmHg), borderline (80-90 mmHg), and abnormal (>90 mmHg).6
For data collection regarding the biological analyses, the subjects fasted for 12 hours and one used a Portable Monitor for determining blood sugar and for cholesterol level, Accutrend Plus Roche® model. Asepsis for the subject's left index finger was done, later on, a puncture with sterile lancet, Roche®, a drop of blood was collected on a blood sugar strip, then, another drop on a test strip for cholesterol, always using the same device that has been calibrated for the respective samples, the results took a few seconds to be ready and have been stored in the mHDC. Blood sugar values were classified as normal (<100 mg/dL), impaired glucose tolerance (100-126 mg/dl) and diabetes mellitus (≥ 126 mg/dl).4 For total cholesterol, values were classified as normal (<200 mg/dl), borderline (200-239 mg/dl) and high (>240 mg/dl).4 Later on, the results were showed by absolute and relative frequency, distributed in tables, with percentage.
Statistical Method. The differences between the women groups on different ages were analyzed using Variance Analysis (One-way ANOVA). The results compared among the different ages were: smoking, alcohol, physical activity, family history for coronary heart disease, cholesterol, blood sugar, WHR, Body Fat Percentage, BMI, systolic and diastolic blood pressure. The statistical significance level for the tests was p<0.05.
Ethical Aspects. The project was approved by the Research Ethics Committee of Universidade Estadual de Londrina under written opinion report number 494.314, CAAE: 24140413.0.0000.5231, and the participation of the subjects in the study was voluntary, consisted of prior acceptance by the subject and women were oriented about the purpose of the survey and after resolving possible doubts, signed the Consent Form. Anonymity was guaranteed, preserving the privacy of the received information.
Results
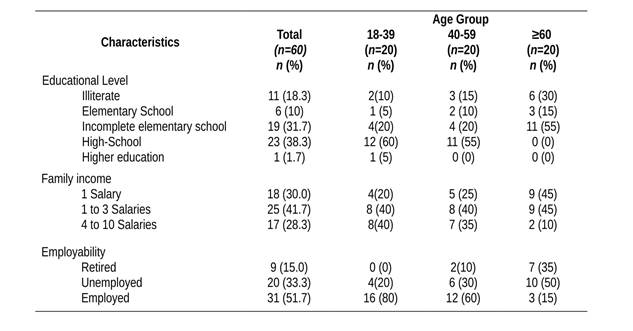
Socioeconomic characteristics. The subjects in this study were divided according to age group, being 20 women aged between 18 and 39 years, 20 between 40 and 59 years and 20 over 60-year old, a total of 60 subjects. Table 1 shows the data for the socioeconomic conditions, such as the educational level, familiar income and conditions in work. Regarding the schooling of the studied population, it was found that for women aged 18 to 39 years and 40 to 59 years, 12 (60%), and 11 (55%) have high-school grade, respectively, and of the 20 women over 60-year old, 11 (55%) have only elementary school. This shows that the lower is the age, the higher the educational level, which may be related to the higher incentive for education and development of the country. On family income, it was verified to be higher in women aged between 18 and 39 years, while in the elderly it is minor, with one to three minimum salaries classification. Regarding employability, most women have employment bond, 16 (80%) between 18 to 39 years, 12 (60%) between 40 to 59 years and women over 60-year old were 10 (50%).
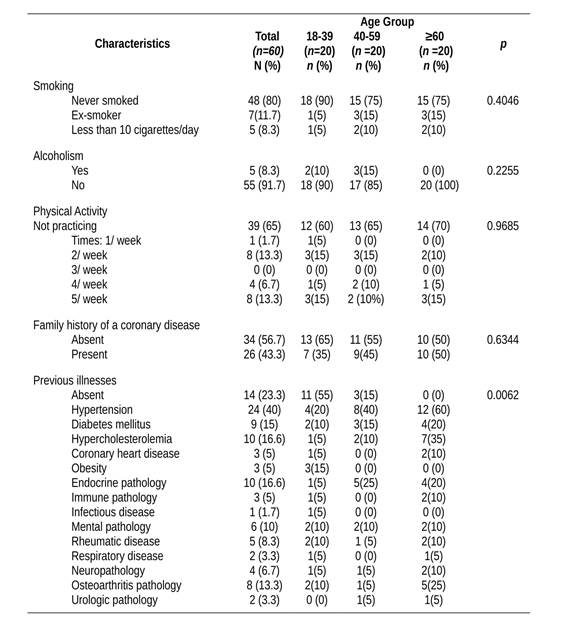
Health indicators and daily habits.Table 2 shows data for health indicators and daily habits, including smoking, alcoholism, physical activity, family history of coronary heart disease and previous illnesses. For smoking, 18 (90%) of the women are aged between 18 to 39 years, 15 (75%) 40 to 59 years and 15 (75%) above 60-year old, have never smoked. With respect to the indicators of alcohol consumption among women from 18 to 39 years, 40 to 59 to 39 years and 60 years or more, 18 (90%), 17 (85%), 20 (100%) reported not consuming alcohol, respectively. In relation to data on physical activity, there was low adhesion of women to physical exercising in all age groups; and 39 (65%) said they do not have this habit. About the family history of coronary heart disease, women were asked if they have already had cases of cardiovascular disease in first-degree relatives (father, mother and/or brother) in their family, as a result, in the age group going from 18 to 39 years and 40 to 59 years, 13 (65%) and 11 (55%) denied owning, respectively. In the age group of women over 60-year old, it was found that 10 (50%) reported coronary heart disease in the family. Also in Table 2, on the indicators of previous diseases, only 14 (23.3%) women denied the existence. The remainder, 46 (76.6%), all had some sort of pre-existing pathology. There is an increase in the pathologies as age increases.
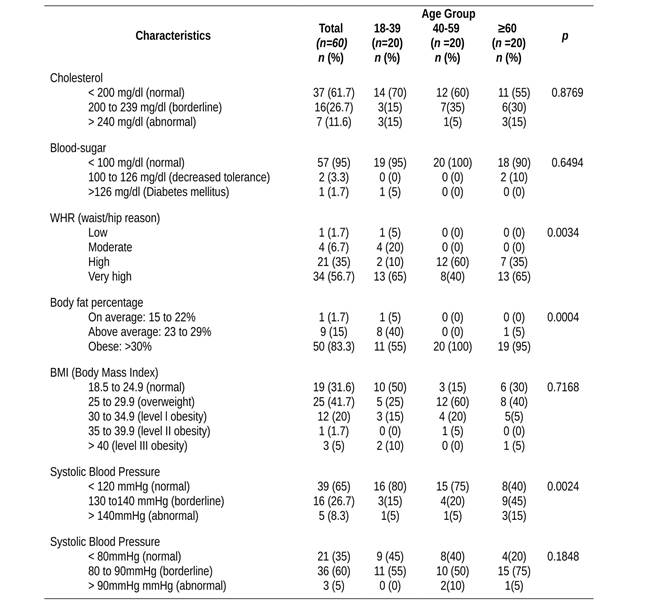
Anthropometric and biological parameters. In Table 3, there are data on cholesterol, blood sugar, WHR, BMI, body fat percentage, and systolic and diastolic blood pressure. In relation to the cholesterol indicators, in all age groups more than half of the women had satisfactory results, but this proportion has decreased as age increased. The results were changed to 6 (30%), 8 (40%) and 9 (45%) between the ages going from 18 to 39 years, 40 to 59 years, and with more than 60-year old, respectively. Being these results concerning for middle-aged women, which resemble to the old ladies. As for the blood sugar, 57 (95%) of women were within normal limits, just 9 interviewees referred a diagnosis for diabetes mellitus, these results suggest that there is a blood sugar control by using pharmacological therapies. Data from BMI, WHR, and body fat percentage (Table 3) were collected in order to measure overweight and obesity. In relation to BMI, normal values were obtained for just 10 (50%) of women aged between 18 to 39 years. Results altered to overweight and obesity, 10 (50%) were from 18 to 39 years, 17 (85%) from 40 to 59 years and 14 (70%) over 60-year old. These results are above the national average and the highest index in women aged from 40 to 59 years.
Regarding the WHR, the results are alarming, only 1 (1.7%) women in the group range from 18 to 39 years had low risk, the remainder, 59 (98.2%) had some type of risk. As a result of abdominal fat accumulation, 15 (75%) from 18 to 39 years and 20 (100%) were classified at high risk of developing chronic diseases in the other bands. These results are interesting, because, as age increases, there is a tendency for an increase in abdominal fat in women, but in our data, the young ladies show results that are very approaching women over 40-year old, bringing a concern with the overall risk of the population for developing chronic diseases. Referring to body fat the percentage, the obesity prevalence has been identified in all age groups, 11 (55%) from 18 to 39 years, 20 (100%) from 40 to 59 years and 19 (95%) above 60-year old are obese complementing the altered values of BMI and WHR. Data on the systolic blood pressure showed only 1 case (5%) abnormal and 3 (15%) borderline in the age group from 18 to 39 years; 1 (5%) and 4 (20%) abnormal and borderline for the range from 40 to 59 years. In the age group above 60-year old, 12 (60%) showed borderline values. The diastolic blood pressure showed borderline value similar for both age groups, respectively, 11 (55%), 10 (50%), 15 (75%), which is worrying, showing that even in young and middle-aged women, there is an approximate index of diastolic pressure with the elderly women that are more likely to shows changes due to factors that involve increasing age.
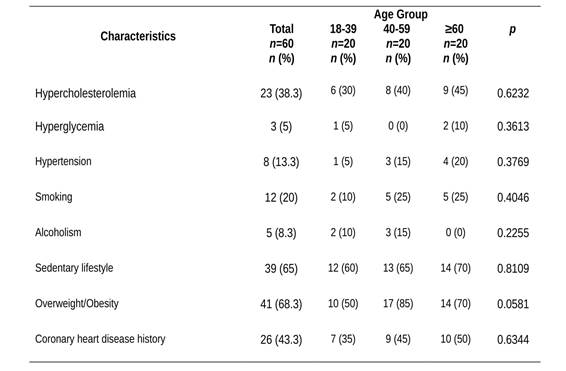
In our study, many women have previous diseases associated with risk factors, such as overweight/obesity (68.3%), physical inactivity (65%), and hypercholesterolemia (38.3%), present in all age groups, especially above 40-year old. In addition, approximately half said they had a history of coronary heart disease in the family (Table 4).
Discussion
Socioeconomic characteristics. Several demographic, social, political, and economic transformations have modified the Brazilian society in the recent decades, causing serious impacts on the lifestyle and health of the population and creating new demands on the public health system. In addition, the role of women in society has also changed over the years, however, there is still much to be discussed, because with the women in the labor market, with increasingly accelerated routine and stress of everyday life, one realizes the carelessness with food and physical activity related issues, in addition to the increased use of substances, such as alcohol and tobacco.1,7) In this study, it was found that with increasing age of women, the level of education decreases and even in youth, education falls short of the desired. Education is seen as essential for promoting citizenship, with visible impact on the population's general life conditions, becoming more and more essential for social inclusion. With the need for qualification for work occupations, there has to be greater access to quality education, therefore, more egalitarian and with opportunity to rise to the most valued positions.8) As for the employability in the last ten years in Brazil, there has been an increase of formal work for men and women over 16-year old. With regard to women, in 2011, 54.8% had a formal job. The informality is a characteristic of the elderly population with 60 years or more (71.7%) and young people from 16 to 24 years (46.5%).8 These rates are still unsatisfactory to be considered ideal for families to enjoy favorable conditions to maintain and increase the standard of living, essential for the family's welfare.
Analyzing the national per capita household income, there is a value of US$ 232.43. Among the units of the Federation, the State of Paraná is in the sixth place, with a per capita household income of US$ 263.81 and 41.66% of women live with one to three minimum salaries, which hampers access to education, good nutrition, since that they often do not reside in their self-owned house and have expenses for transport to work.8) A study conducted in the metropolitan region of Londrina, Cambé, Paraná, Brazil, examined the association between indicators of social capital and behavior related to health and stressed out that the economic status affects health outcomes, having the social capital score inverse relationship with the number of health risk behaviors, reinforcing the importance of social capital in health promotion policies. In other words, less social capital indexes were associated with insufficient physical activity rate, irregular fruit, and vegetable consumption and increased smoking, while the highest social capital showed low average for risky behavior.7 In our study, we included the level of education, occupation, and income for an association with the results related to the health of this population and we saw that the level of education and income are not favorable and may be one of the factors for results with risky behavior.
Health indicators and daily habits. According to some authors, health indicators, especially the cause of morbidity, serve to draw the epidemiological profile of a particular region and the analysis of this indicator translates into an important tool in health research and can contribute to the understanding of the involved processes, as well as planning public health actions. In this sense, other studies suggest that behaviors and lifestyles are important social determinants for chronic conditions.2,7,10) Among the indicators, smoking and alcohol consumption had little prominence in all age groups. A study conducted in the city of Fortaleza, Ceará. Brazil, 2691 people registered in the health system for hypertension or diabetes, 73.6% were women and 79.7% were non-smokers,11 similar to our findings that were 80% of non-smokers. Other studies also showed low rates for tobacco consumption, being the largest tobacco and alcohol consumption seen mainly in men as age decreases and usually associated.3,7,12
As for physical inactivity, our results show that 65% of the interviewees said they did not have the habit to practice physical activity. Similar data have been observed in another study in Cambé, Paraná, Brazil, that among the examined risk factors, the prevalence was higher in relation to physical inactivity and obesity.13) Other researches in the same municipality showed that physical inactivity was more prevalent (71.3%) followed by low or moderate consumption of fruits and vegetables (63.1%), smoking (19.7%) and abusive consumption of alcohol (18.2%),7,14 being that women showed negative behavior (52.3%), being prevalent in lower economic classes, with lower educational level and age between 40 and 49 years,15 similar to our findings. Research conducted in the northeastern of Brazil, show that 56.9 percent of women did not practice physical activity, and 32% practiced up to twice a week,16 being the results similar to our study's results. Another study with women in Latin America shows that only 6.6% practiced physical exercises five days a week, 25% two or more days a week, from the 31.6% who practiced physical activity.16
Unhealthy lifestyles, such as inadequate food and lack of physical activity are the main factors that contribute to mortality from cardiovascular disease, stroke, respiratory disease and diabetes. In addition to contributing as the main causes for death by cancer in middle and low-income individuals: being tobacco responsible for 18% of deaths; low consumption of fruits and vegetables for 6% of deaths; and excessive consumption of alcohol for 5% of deaths.3) Still, as for auto-recovering health and demographic variables, there is higher prevalence of negative self-perception in women, individuals with less schooling or any chronic disease.17 In our study, many women have previous diseases associated with risk factors like cardiovascular, rheumatic, endocrine, osteoarthritis and mental diseases, found in all age groups, especially above 40-year old. In addition, approximately half said they had a history of coronary heart disease in the family, which is worrisome, because study shows that family history cardiovascular disease is associated with coronary heart disease and myocardial infarction.11 This reinforces that these women in our study need to be cared for and that the health team need to offer health controlling measures and work for risk reduction in this population, whereas the PHC nurses together with their team are making this work. As reported in study, nurses should be attentive with the population that has greater exposure to risk factors for the metabolic syndrome, working to strengthen the educational programs that promote healthy lifestyles.18
Anthropometric and biological parameters. In relation to cholesterol, 38.3% of the women showed borderline and abnormal values. Now, in a study conducted in the State of Maranhão, in northern Brazil, with 218 women, there was a prevalence of altered lipid profile (hypercholesterolemia in 68.8%) and weight excess.19 Blood sugar level showed normal in 95% of women, while borderline and abnormal blood sugar values in 5%, and 15% reported having Diabetes diagnosis, suggesting they are controlled by pharmacological treatment. Our findings are smaller than the national average which shows 8% of the population with Diabetes.1 Different values may be due to methodological differences that in national survey this was done via phone while our study used biochemical tests for blood sugar. Our sample was small not representing the southern region of the country, which have values greater than the national average, as shown in another study done in our region with men and women over 40-year old, showed 12.1% of individuals that reported having Diabetes, which differ from our findings.20
In anthropometric measurements in our study, the WHR was elevated in 91.6% of women. In a study conducted in Brazil, 83.7% of the 369 individuals had inappropriate WHR values and 85.4% were women and 89.7% were sedentary,21 a fact that agrees with our findings. A study in our region showed prevalence of abdominal obesity for 49.7% in men and women, and was higher in women (more than double that in men) and increases with age progression, mainly from 50-year old,20 being similar to our results that there was prevalence in all ages with higher emphasis from 40 to 59 years. Other research reports that there are greater risks for cardiovascular events with increased waist circumference,22 indicating that women from our study have risk for developing chronic diseases, because they have high values on the WHR, BMI and body fat percentage, followed by high obesity rate. Data on the systolic and diastolic pressure are worrisome, especially in borderline diastolic in 60% of all interviewees. There has been found in other studies a prevalence of 60%23) and 65%18) of the sample with high blood pressure, representing more than half of the individuals, being similar to our findings. Another study with the Brazilian population has shown that the south region of the country had a greater increase in blood pressure from 2006 to 2011 as compared to other states and the prevalence was higher in women.24
The ELSA-Brazil study researched Brazilian adults about the risk factors for developing chronic disease, found in 63.1% of the population overweight, 61.5% hypercholesterolemia, 35.8% hypertension, 20.3% glucose intolerance, 19.7% diabetes, 26.7% mental disorder, and 4.7% coronary heart disease history. In this study, when comparing women and men, there was highest rate for sedentary lifestyle (79.9%), obesity (24.8%), hypercholesterolemia (63.6%), low HDL (20.7%), mental disorders (33.7%), cancer (5%) and respiratory diseases (13%).25 Some of our findings are close to ELSA-Brazil, such as sedentary lifestyle (65%) and obesity (26.6%).
Abnormal health conditions and daily habits of women characterize the risk for developing cardiovascular diseases, highlighting in this study obesity, overweight, followed by physical inactivity, previous history of cardiovascular disease, hypercholesterolemia and hypertension, but had greater emphasis on the obesity risk factor in women over 40-year old, also remaining relevant in young women. As the results of our study, there are similar data, highlighting obesity, hypertension, low HDL, unhealthy diet and sedentary lifestyle related as risk behaviors and social capital. 1,7,14,15,18-24) Despite all these data, studies have evidenced that CNTD mortality rate showed a tendency for reduction of about 20% since the 1990's, being observed larger reductions in cerebrovascular, chronic respiratory and ischemic disorders. The authors attribute this reduction to PHC's expansion, covering more than 60% of the population, improving access to healthcare and the significant reduction for prevalence of smoking in Brazil, from 34.8% (1989) to 8.7% (2014).1,3 But in our study region it is necessary to be attentive, a survey that assessed rates of hospitalization for cardiovascular disease sensitive to PHC and coverage of the FHS for residents in the State of Paraná, showed that in our region there was no significant reduction of hospitalizations, revealing little stability or falls in these rates,26 indicating that even with greater coverage by the FHS there are still no improvements in the indicators, being needed a better performance of the nursing team and other health professionals with setting targets based on the Strategic Action Plan for Confronting the CNTD.2 And further studies in order to identify likely factors and causes that have influenced the results, such as access and quality of service.26
Advantages and limitations. There are important aspects in our study that shows the reality for a small part of the urban population, which has important socio-demographic lifestyle associated to obesity and risk factors for developing coronary heart disease. The study encompassed both healthy individuals (looking for the PHC for prevention and primary healthcare routine) and also a population with diseases, showing the reality of this population from 18-year old, unlike some studies that analyzed the factors in hypertensive population only,11 population from 40-year old,7,14,15,20 elderly 18) and the population in general of a state and a country.1,2,16,24 In addition to those, blood pressure and blood sugar and cholesterol values were checked at the time of the research and not just the disease being mentioned by the individual as it is in the researches done by population survey.1,2,20,24) There are limitations in this study, and the data were broken down by ethnicity; the calculated sample has a 90% confidence level and 10% error in the calculation; the addressed population is from a region that has lower socioeconomic level; although we consider the population looking for a BHU as a healthy part (prevention) and part ill (in treatment), in Brazil we still have the culture in most for the individuals to seek healthcare when there is a complaint, then it may be that our data represent a population that is more sick than healthy.
Conclusion
Analyzing these results, there is prevalence of obesity, overweight, physical inactivity, followed by a previous history of cardiovascular disease, hypercholesterolemia and hypertension, especially in women over 40-year old, remaining relevant in young women. Thereby, it is necessary to implement stimulus measures in order to change positively the modifiable risk factors and improve health conditions among women in order to reduce the risk for cardiovascular disease. There is a need for prepared health professionals, as the nursing team acts directly in the PHC services in order to care, guide, and decide on the health demands, welcoming the woman and her family throughout the process, working in prevention, early stages of signs and symptoms, illness with integral care and continuity. Thereby, health promotion activities can empower women on the benefits of appropriate behaviors and lifestyles that may help reducing the risks for cardiovascular disease included in the Strategic Action Plan for Confronting the CNTD, such as working with healthy eating strategies avoiding obesogenic products, reducing salt consumption and encouraging physical activity groups.
Acknowledgments
We thank to all study participants, and Londrina City Hall that accepted the research.We are also immensely grateful to Henrique Yoshikazu Shishido for the technical supporting and developing the software (mHealth Data Collector) for this study. This research was partially funded by the Federal Institute of Paraná (Program to Encourage and Support the Research - PIAP/2013).

