











 texto em
texto em  Inglês (pdf)
Inglês (pdf)
 Artigo em XML
Artigo em XML Referências do artigo
Referências do artigo
 Enviar este artigo por email
Enviar este artigo por email Citado por SciELO
Citado por SciELO  Citado por Google
Citado por Google  Similares em
SciELO
Similares em
SciELO  Similares em Google
Similares em Google 
 Permalink
PermalinkIntroduction
Systemic arterial hypertension (SAH) and diabetes mellitus (DM) are chronic noncommunicable diseases (CNCDs), that is, diseases that are persistent and require permanent care.1) Global data indicate that, in 2015, 415 million people between 20 and 79 years of age were living with DM and it is estimated that in 2040 there will be 642 million people with this disease, increasing by 65% in Central and South America.2 Epidemiological studies indicate that diabetes and hypertension are commonly associated conditions.3,4 The prevalence of hypertension is approximately twice as high among diabetics compared to non-diabetics. This alarming information is mainly due to sedentary lifestyle, obesity and the aging of the world population.4
Considering the increasing incidence of new cases of CNCDs, the need for preventive and control actions have become crucial, since they represent an important public health problem.5 In Brazil, the monitoring of individuals with a diagnosis of SAH and DM should be carried out primarily by Primary Health Care (PHC).3,5 PHC is considered the gateway to the health system, by establishing its own level of care, with the structuring of service in the programmatic dialectics, in the longitudinal care, comprehensiveness and in the coordination of health actions and services.3,5) Although it has been established for more than a decade in Brazil, the standard of care for people with SAH and DM by PHC, that is, the Hiperdia program, which consists of the continuous monitoring of these individuals along with the basic health units (BHU) of the Brazilian Health System (SUS), with the provision of medicines and the promotion of healthy living habits, there is still a low percentage of follow-up of these people by the professional teams of the BHUs.6,7 Therefore, it is essential that professionals maintain the provision of a comprehensive, effective and quality care.1,3,4 In this way, in addition to curative care, professionals must be able to perform early detection of risk factors for CNCDs, as well as organize strategies for their prevention.3
Thus, nursing can act in an expressive, evidence-based manner, identifying human responses and establishing strategies that provide for the recovery of health and/or the improvement of individual or collective well-being. For this, nursing needs to use tools, such as the Nursing Process (NP), which, when executed using standard languages7 and encompassing nursing diagnoses of NANDA International (NANDA-I),8 systematizes the care provided to the person, family or community focusing on the coprehensive care and interaction between professional-client-family.7,8) Nursing diagnoses (ND) are clinical judgments derived from interpretations of information/data raised during the nursing appointment.8 They compose the synthesis of clinical reasoning and are primordial in the orientation of nursing care planning, implementation of interventions and evaluation of care provided.7 The situations/potentialities of nursing diagnoses are: problem-focused, health promotion and risk promotion.8 The elaboration of ND brings multiple benefits, such as an objective assessment of care; it helps in determining priorities in nursing care, promotes a continuous development of the profession, contributes to improving the quality of care and facilitates the selection of the most important nursing interventions that lead to better results.10,11
In a systematic review of the evidence of the use of standardized nursing language, the authors emphasized the importance of conducting studies to link the use of taxonomies with the health outcomes of clients.9 Studies addressing ND for hypertensive and diabetic individuals were found, however, with small number of participants and convenience sampling,12 case study,13,14 others studies addressing ND/nursing interventions for hypertensive people only15-17 or describing the ND/nursing process for diabetics18,19 and addressing the management of the two chronic diseases without describing the ND.20,21 Therefore, although there has been a wide discussion about the nursing process and the management of hypertension and DM, there has also been a shortage of articles describing the profile of ND of hypertensive individuals and also diabetic users of PHC with sample size from the population of interest and with data obtained through anamnesis and physical examination of all the participants by the researchers themselves. Within this perspective, this study is of great relevance to improve the care of nurses working in PHC, as well as to corroborate or confront the existing NDs in the literature. Therefore, the objective of this study was to identify the profile of nursing diagnoses of hypertensive and diabetic people using Primary Health Care.
Methods
This is an exploratory and descriptive study, carried out in eight BHUs located in the state of Minas Gerais, Brazil. These BHUs were intentionally chosen because they received nurses linked to a residency program on Primary Health Care/Family Health Care. This is a postgraduate specialization with a weekly workload of 60 hours intended for in-service teaching of health-related professions, in this case, nurses. One of the structuring axes of residencies should be the comprehensiveness of care with the adoption of evidence-based practice; therefore, the use of the NP is essential.22) People with type 2 diabetes mellitus and hypertension, enrolled in the Hiperdia program, were chosen as the selection criteria in the participating health units. Inclusion criteria were clients over 18 years of age with preserved cognitive ability, which was verified through the application of the Mini Mental State Exam, an important tool for screening cognitive impairment to be used in research and clinical evaluation, validated for the Brazilian population.23 Exclusion criteria included individuals with other medical diagnoses and hospitalizations during the study period.
Data were collected at the participant's home or at their reference health unit by two researchers, from September 2015 to July 2016. The study population comprised 175 adults with hypertension and diabetes. The sample calculation was defined by means of the z statistic test, with a normal distribution, estimating a proportion referring to the population of interest for a significance level of 5% and statistical test power of 80%. Data were obtained by primary source directly with the clients, through interview and physical examination.
For the clinical evaluation of the participants and interview, a form prepared by the authors was used, based on two previous studies. The first, on the validation of a questionnaire with diabetic adults in Brazil and the other, on an instrument for nursing appointment of hypertensive patients in family health.24,25 This form contained data regarding the date of birth, sex, marital status, SUS card number, profession, religion, occupation, housing, information on the disease and treatment, medications in use, family history, lifestyle, psychosocial data, vital signs and physical examination with relevant information about organs and systems. The collected data were examined based on the process of diagnostic reasoning proposed by Gordon, which involves the following steps: information collection, interpretation of information, grouping of information and denomination of nursing diagnoses, in this case, using the NANDA-I Taxonomy.8)
The indications and inferences obtained, based on the scientific basis of nursing diagnoses, were performed by two authors independently. One of the researchers was the one who collected and filled out the instruments with the clients, and the other researcher, a specialist in nursing diagnosis, member of NANDA-I, performed the diagnostic reasoning process based on the filled instruments. Afterwards, the nursing diagnoses were compared and, when there was disagreement, the two researchers debated until reaching an agreement. The data obtained were organized in a database built in the software Excel version 2016 and statistical analysis was done through the Statistical Package for the Social Sciences (SPSS), version 21.0 for Windows® and Program Epi Info, version 7, according to absolute and relative measures of numerical frequency, measures of central tendency and dispersion.
This research was approved by the Research Ethics Committee of a Federal University of Minas Gerais, Brazil (CAAE: 46439415.7.0000.5545 and Opinion no. 1,218,267/2015). Data were collected after the participant signed the Informed Consent Form.
Results
Of the 175 hypertensive and diabetic subjects, 66.9% were female. The age ranged from 39 to 89 years, with a mean of 62.1 years and a standard deviation of 10.6. The majority were married (62.3%), had some religious practice (93.1%), incomplete elementary school (57.7%), were retired or pensioner (%), had white skin color (52%), and 94.8% did not live alone. All interviewees lived in urban areas with access to running water and basic sanitation (Table 1).
Table 1 General characteristics of 175 hypertensive and diabetic subjects. Minas Gerais Brazil, 2016
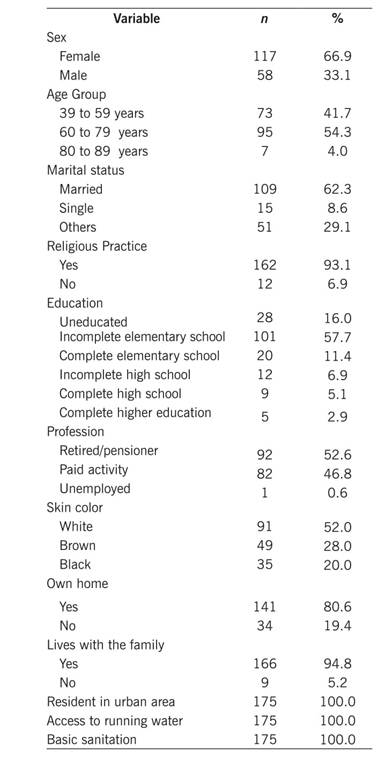
The average length of time patients lived with the disease was 17.8 years for hypertension and 10.8 years for diabetes. Regarding users' knowledge on their health problem, 72% were poorly oriented while only 20.6% showed some knowledge about their current condition. Regarding the risk classification of these users in the Hiperdia program, 71.4% were considered individuals at high risk for the development of cardiovascular diseases and complications associated with hypertension and diabetes, 16.6% were at moderate risk and 12% at low risk.
From the diagnostic reasoning process, 26 different diagnoses were identified, with a mean of 16 ND per client, 39 defining characteristics, 46 related factors and 62 risk factors (Table 2).
Table 2 Distribution of nursing diagnoses, defining characteristics, related factors and risk factors formulated for the 175 hypertensive and diabetic participants. Minas Gerais Brazil, 2016

*Confidence Interval
Most of the nursing diagnoses found were of the domain activity/rest (38.5%), followed by nutrition (15.4%), safety/protection (15.4%), health promotion (11.5%), elimination and discharge (7.7%), coping/stress tolerance (7.7%) and comfort (3.8%). 13 (50%) ND were problem-focused, 12 (46.1%) were risk nursing diagnoses and one (3.9%) diagnosis was of health promotion. Nursing diagnoses were observed in all clients: risk for ineffective gastrointestinal perfusion, risk for ineffective renal perfusion, risk for reduced cardiac tissue perfusion, risk for ineffective peripheral tissue perfusion, risk for impaired cardiovascular function. Other high frequency diagnoses above the 75th percentile were: ineffective health control (98.9%), risk for unstable blood glucose level (92.6%), risk for constipation (82.3%), ineffective peripheral tissue perfusion (78.3%), risk for activity intolerance (78.3%). Nursing diagnoses were organized according to 75th, 50th, 25th and below 25th percentiles (Table 3). In the data found, the nursing diagnoses that presented above the 50th percentile were analyzed.
Table
3 Distribution of the nursing diagnoses formulated for the 175 hypertensive and diabetic participants, according to the domains of human response and according to the percentile. Minas Gerais Brazil, 2016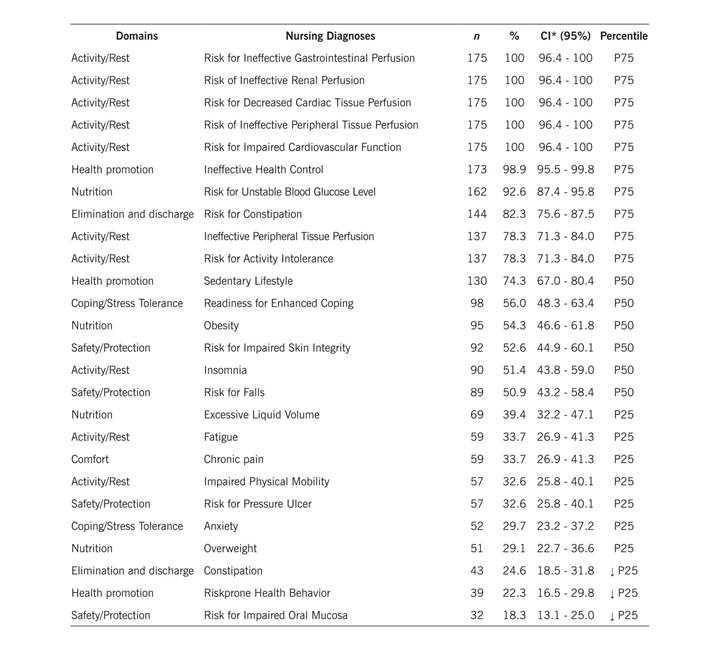
Table 4 below shows the distribution of the defining characteristics and the most significant related factors in the ND proposed for the hypertensive and diabetic clients of this study. It shows that, in relation to the ND with a high frequency, above the 75th percentile, that is, ''Ineffective Health Control'', the defining characteristics: Failure to include treatment regimen in daily living (98.9%) and Ineffective choices in daily living for meeting health goals (98.9%) and; the related factor: Perceived barrier (90.3%) were the most observed in the participants. In the NE ''Ineffective Peripheral Tissue Perfusion'', the defining characteristic: Altered skin characteristics (78.3%) and the related factors: SAH and DM (100.0%) were the most examined in participants.
Table 4 Distribution of the 39 defining characteristics and 46 related factors of the nursing diagnoses proposed for hypertensive and diabetic clients. Minas Gerais Brazil, 2016
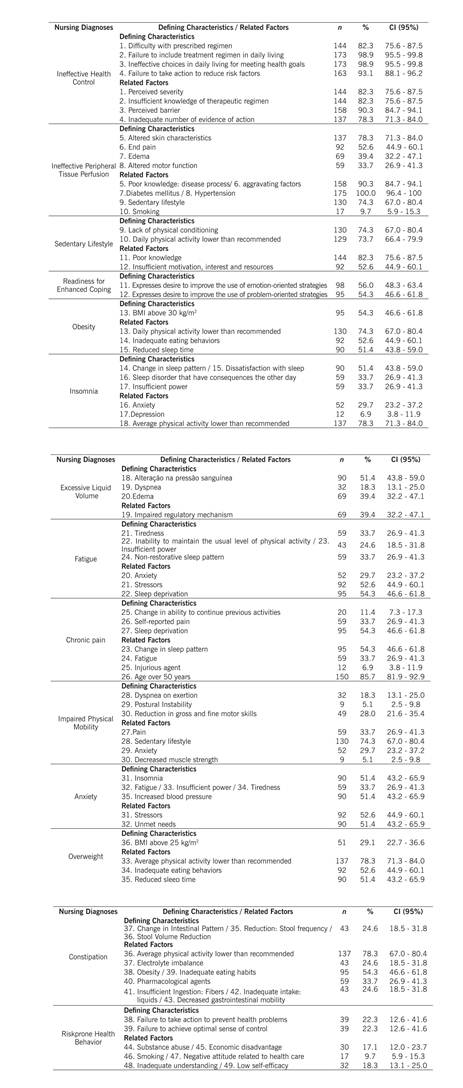
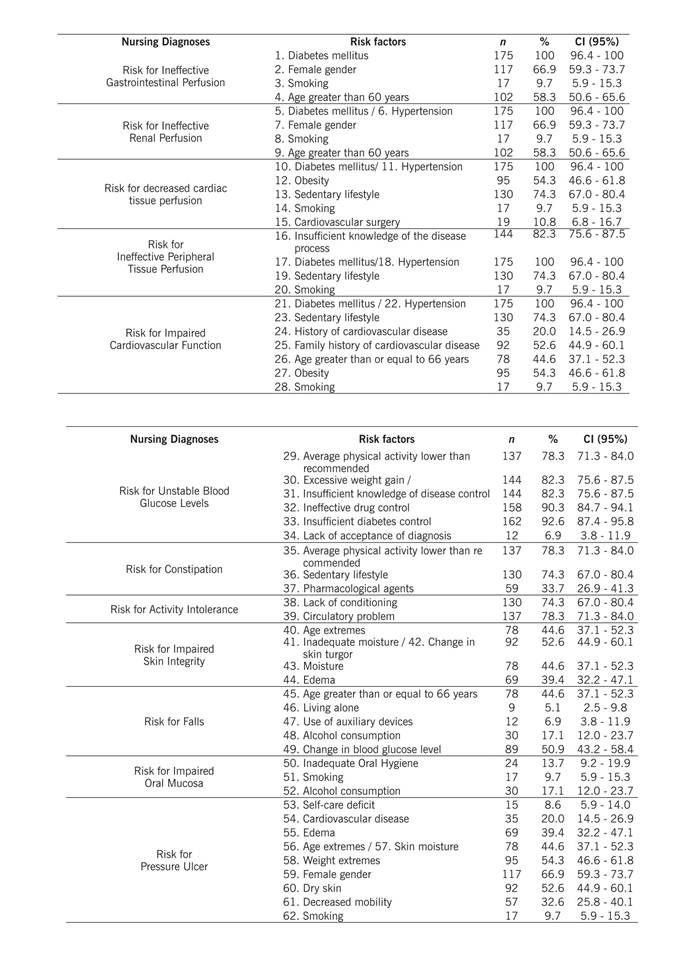
Table 5 below shows the risk diagnoses of hypertensive and diabetic clients according to the vulnerabilities. The risk factor of high frequency, i.e., above the 75th percentile, that is, ''risk for ineffective gastrointestinal perfusion'', the risk factor DM (100.0%) was the most observed in people of this group research; regarding the ND "Risk for ineffective renal perfusion", "Risk for decreased cardiac tissue perfusion", "Risk for ineffective peripheral tissue perfusion", "Risk for impaired cardiovascular function", risk factors for hypertension (100.0%) and DM (100.0%). With regard to the ND "Risk for unstable blood glucose levels", the most commonly found risk factors were: Insufficient control of diabetes (92.6%) and Ineffective drug control (90.3%) and; in relation to the ND "Risk for constipation", the risk factor Average physical activity lower than recommended (78.3%) was the most prevalent. Regarding the ND "Risk for activity intolerance", the risk factor circulatory problem (78.3%) stood out in hypertensive and diabetic subjects in this study.
Discussion
A person's life habits, beliefs and values characterize the way the individual identifies themselves within the social world. Such attitudes are corroborated by socioeconomic and political factors that interfere with the environment, behavior and biology of these individuals, influencing the health-illness process and, consequently, their disposition, safety, independence and quality of life.(1) These environmental/cultural/social/historical determinants influence inexorably in the daily lives of people with chronic diseases, such as hypertensive and diabetic patients.(1,5) Therefore, they need care and follow-up provided by the health services in order to have a better quality of life.
The analysis of the data revealed that the majority of the interviewed population were female, married, had some religious practice, incomplete elementary education and average age of 62.1 years, did not live alone and had retirement or pension as the main source of income. This reflects the reality of low- and middle-income populations around the world as they are most affected by chronic diseases and their complications. The percentage of elderly people living with their children continues to be high, even with the increase in longevity, which corroborates the research carried out with elderly people assisted by the Family Health Strategy of a municipality in Minas Gerais, Brazil.(5) In relation to ethnicity, the white color predominated, as opposed to other studies that indicate a higher prevalence of chronic auto-referred diseases in black people when compared to white.(6) The baseline diseases studied, hypertension and diabetes mellitus, had a significant mean time of diagnosis, being 17.8 years for hypertension and 10.8 years for diabetes. This data shows that in the majority of clients interviewed, hypertension evolved with a prognosis for diabetes. From the epidemiological point of view, hypertension is considered three times more frequent in diabetics than in the general population. In type 2 diabetics, about 40% have already been hypertensive at the time of diagnosis.(1,5,6)
However, despite the respective periods with the diseases, a considerable number of participants presented deficient knowledge about the meaning of the diseases, their complications, prognosis and treatment, mainly related to the use of insulin. The lack of information becomes an obstacle to user empowerment and to adherence to treatment. Hypertensive and diabetic patients are known have chronic conditions that require continuous nursing care in order to prevent complications from diseases. Health care priorities are defined in an equitable manner, according to the degree of risk they present, and high risk, observed in 71.4% of the participants, corresponds to the population that demands greater attention. In view of the above, nurses should improve their practices, based on scientific evidence for decision making, which requires that nursing care is based on nursing diagnoses in order to prevent complications that affect quality of life of the hypertensive and diabetic individual in a general manner. This study identified a total of 26 different nursing diagnoses, 13 problem-focused diagnoses, 12 risk diagnoses and one diagnosis of health promotion, presenting an average of 16 diagnoses per client, 24 defining characteristics, 28 related factors and 38 risk factors.
The quantity and multiplicity of NDs detected in this study indicate that nursing professionals need to develop individualized interventions, always aiming at the humanization of health actions, the respect for the dignity and the comprehensiveness of the citizen, also assuming a dialogical interaction, respecting the needs and fears of expressing the aspirations lived by each person. This profile of nursing diagnoses was relevant since, in the planning of nursing care, the initial care to the problem-focused diagnoses should be prioritized. These diagnoses are the human responses to health conditions and preventive interventions must be implemented jointly for the risk diagnoses.(10,11) Five risk diagnoses were present in all hypertensive and diabetic subjects interviewed ("Risk for Ineffective Gastrointestinal Perfusion", "Risk for Ineffective Renal Perfusion", "Risk for Decreased Cardiac Tissue Perfusion", "Risk for Ineffective Peripheral Tissue Perfusion", "Risk for Impaired Cardiovascular Function"), and other five diagnoses ("Risk for Unstable Blood Glucose Levels", "Risk for Constipation", " Risk for Activity Intolerance", "Risk for Impaired Skin Integrity" and "Risk for Falls") score above the 50th percentile. Given this finding, nursing care planning should be performed in a way to make a control of risks, with the goal of prioritizing safety. Research performed at the PHC in Madrid, Spain, showed that clients with CNCDs had better indicators of control of their condition in health units where nurses used the nursing process compared to clients accompanied by nurses who do not use NP.(11)
With regard to nursing diagnoses, studies involving diagnoses profile in specific clinical circumstances and those related to validation and diagnostic accuracy have helped in the process of diagnostic inference, making clinical practice more safe and effective.(7) In this research, the defining characteristics ''Failure to include treatment regimen in daily living'' and ''Ineffective choices in daily living for meeting health goals'' of the nursing diagnosis ''Ineffective Health Control'' were the most observed among participants. Data from the literature show that long-term or chronic treatments generally have less adherence, since therapeutic regimens require discipline and a great commitment of the client who, at times, needs to modify their habits of life to fulfill their treatment.(1,5) For this reason, hypertensive and diabetic patients must have adequate answers to their doubts regarding the management of chronic diseases, such as care related to specific use of medications, the search for adequate diet, physical activity, among others. This will provide greater credibility around health professionals and therefore provide customers with real and individualized parameters for their self-care.(4,5)
The diagnosis "Ineffective Peripheral Tissue Perfusion", referring to the reduction of blood circulation to the periphery, which can compromise health(8) due to "altered skin characteristics", score above the 75th percentile. Poor knowledge about the disease process, sedentary lifestyle and self-reported smoking are relevant variables that influenced ineffective peripheral perfusion, corroborating with the literature.(1,7) The diagnostic title "Sedentary Lifestyle", evidenced in the majority of the participants, refers to a habit of life characterized by a low level of physical activity.(8) In a study on the review of the nursing diagnosis ''Sedentary lifestyle'' in hypertensive patients, the defining characteristics of ''Choice of a daily routine without physical exercises'' and ''Lack of physical conditioning'' were the main ones of this diagnosis, according to a conceptual analysis performed by the authors.(26) Many studies have shown that lifestyle modification in people with chronic conditions, besides contributing to the improvement of indicators of clinical control of diseases, significantly reduces drug consumption and, consequently, financial costs with drugs.(1,4,6)
The nursing diagnosis with potential for health promotion "Readiness for enhanced coping", which refers to the pattern of behavioral and cognitive efforts to address demands for well-being and that can be strengthened (8) was observed in 56.0% of the studied public. 60.57% of respondents are optimistic about their treatment and although 74.3% are sedentary, 82.8% believe that physical exercise is paramount for their health and for the control of chronic diseases diagnosed. This is contrary to the literature, since this diagnosis has not been verified in other studies with hypertensive and/or diabetic patients. In a considerable number of patients (54.2%), the diagnosis "Obesity" was identified, a condition in which the individual accumulates abnormal or excessive fat for their age and sex, which exceeds overweight.(8) Obesity has been considered a serious public health problem, reaching ever higher levels among the elderly in Brazil and in the world.(1,5) Faced with this reality, nurses should encourage changes to promote a healthier lifestyle, including helping users overcome obstacles related to dietary changes, regular physical exercise and use of community support devices.
The diagnosis "Insomnia", considered as a disturbance in the quantity and quality of sleep that impairs functioning,(8) was present in 51.4% of the participants. The defining characteristics associated to the definition of this diagnosis include "dissatisfaction with sleep", "anxiety" and "sedentary lifestyle". Impaired sleep increases blood pressure, increases appetite and may compromise insulin sensitivity, as well as being associated with the incidence of diabetes.(1,2) Insomnia is more frequent from middle age, as in the population of this study. This fact has been proven by other studies.(5,10)
In view of the above, when providing care for chronically ill users, nurses should adopt a flexible, individualized approach adjusted to the different stages of the disease, to the needs and interests of each individual, and appropriate to the cultural environment where care is provided. One of the most important aspects for the control of chronic diseases is the therapeutic adherence, since non-compliance or lack of adherence to treatment is considered the main cause of difficulty in the control of chronic diseases.(1,5) A research has showed that nurses who use the nursing process in PHC presented greater coverage in all health promotion services and risk and injury prevention, better indicators of control of the patient's health condition and consequently less expenditures on the consumption of medicines, when compared to nurses who planned and executed their interventions without the aid of the nursing process.(11)
These results allow concluding that establishing the profile of hypertensive and diabetic people assisted in PHC is necessary to propose care actions specific to this clientele, considering their limitations and possibilities in coping with the disease. Health education actions carried out in the basic health units environment and focused on the profile of this clientele are crucial and may favor changes in behaviors in the hypertensive and diabetic person. In the present study, 26 NDs were identified, according to NANDA-I, and 16 diagnoses above the 50th percentile were found and discussed in greater depth. The largest number of NDs was identified in the domain activity/rest. Risk diagnoses had an expressive frequency, corroborating the risk classification of these users in the Hiperdia program, in which the great majority of the participants in this study were considered to be at high risk for the development of cardiovascular diseases and complications associated with hypertension and diabetes.
The objective outlined for this study was reached; however, a limiting factor in this study was the fact that it was performed only with the research and diagnosis stages of the nursing process. Thus, further studies that contemplate all stages of the nursing process should be carries out aiming at developing accuracy, validation, results and intervention studies involving the main diagnoses found in this study in order to confirm the findings and cooperate with the choice of the defining characteristics and related factors that actually represent the conditions of the hypertensive and diabetic client.

