











 text in
text in  English (pdf)
English (pdf)
 Article in xml format
Article in xml format Article references
Article references
 Send this article by e-mail
Send this article by e-mail Cited by SciELO
Cited by SciELO  Cited by Google
Cited by Google  Similars in
SciELO
Similars in
SciELO  Similars in Google
Similars in Google 
 Permalink
PermalinkIntroduction
Throughout history, humans have developed and evolutions their way of living from different dimensions that characterize the past holistic beings, among these is the overwhelming and incredible capacity to create and innovate their lifestyle, by inventing new artifacts, improving these, and through technological progress that improve their comfort and offer well-being. Nevertheless, this human conduct has been at the forefront of effectively responding to those needs and problems that affect humanity, as well as diseases, from the development and improvement of medications, treatments, artifacts, and clinical services. This technological progress in health has created highly technical and developed environments to provide effective optimal intervention from the health staff, especially from nursing, on the use and handling of technology to care for life and human health.
By the mid-1970s, hospital institutions began to develop and create higher quality care models, with the aid of better equipment and from the technological progress to offer better services to patients and their families. Then, questions emerged on the sense and meaning assigned to technology in the professional care nursing provides to its patients. This led to reflecting on whether technology is becoming a barrier that distances and displaces personal and human contact between nursing professionals and their patients, or if the distancing and division is not technology itself; rather, the sense humans have of detracting from the reason said technology was created, in the first place, as a tool and aid to express their care with a high degree of quality and humanization and, in the second place, to recognize patients as humans just as the nursing professionals, who expect dignified treatment.1 Quite often, technology has been considered contrary to caring, that is, technology as a factor that isolates personal and human contact between nursing professionals and their patients, considered dichotomous. Due to user manifestations on healthcare services on dehumanization, in recent years, it has become relevant to discuss on humanization, defined as the “conduct and actions in thoughtful, emotional, and existential manner that differentiates it from other species, being an action inherent to human behavior”,2 and dehumanization as every physical or verbal action that generates harm or abuse from one person over another.
Some predecessors to the study of human care in nursing include Jean Watson with the theory of human care3 and Anne Boykin and Savina Schoenhofer with the theory of nursing con la Theory of Nursing as Caring in a kind, human and warm manner. (4 Regarding the construct of Technology and Care, it has been defined by authors like Marilyn Anne Ray,5 who published the theory of Technological Care, and Margarete Sandelowski with the theory of Dependence on Technology.6 These proposals were the foundation for the midrange theory Technological Competency as Caring in Nursing (TCCN) by Rozzano Locsin,7 as well as Heidegger’s philosophical thoughts that defined technology:8 “technology is seen as a means to an end and as a human activity” and Peck’s:9 “technology for nursing is the instrument to know about fully in the patient’s well-being”. These statements highlight that technology is an activity created by man and designed as a tool for the modern development of humans; additionally, the study of technology in relation to nursing care defines technology as an expression of nursing. Locsin proposes that the technological competency of Nursing is a skill and expertise to offer care, within a context that permits knowing patients integrally and achieving their recovery and healing under the premise of a harmonious coexistence between technology and care.7)
The TCCN is a relatively new theory, as well as the Technological Competency as Caring in Nursing Instrument (TCCNI).10) Its development began in 1999 when Dr. Locsin created the instrument from the theory of Technological Caring by Dr. Ray: Technological Caring Instrument (TCI),11 applied to hospitalization nurses (in critical and noncritical areas), which permitted designing and elaborating her first version of the instruments in its TCCNI theory with 30 items in 2010. This version was subjected to content validity with 13 experts related to and familiarized with the theory and practice, among which there were five theorists with over 20 years dedicated to nursing in education, practice, and research, and eight expert nurses women average of 15 years of practice experience in different specializations in the United States. The TCCNI was adapted to one electronic formats in an analog visual scale through linear graphics, where the left extreme of the line corresponds to totally disagree and the far right to totally agree. This research was adapted to Likert-type response options (totally disagree, disagree, agree, and totally agree) with prior authorization from the author. The results yielded a version of 25 items that was the basis of our study.10 According to email communication with the author on 22 August 2012, this version is applicable to nursing professionals to evaluate their competency and to users as an indicator of nursing care. The dimensions in which the instrument was originally postulated were based by the author on the TCCNI theoretical assumptions, which prior to the study were: D1-Knowing people/patients = items 4, 5, 7, 8, 9, 15, and 19; D2-Technological competency = items 13, 22, 23, 24, and 25; D3-Nursing as a discipline and profession = items 2, 6, 12, 17, and 21; D4- Nursing care = items 10, 11, and 14; and D5- People as participants in their care = items 1, 3, 18, 20 y 16) . The objective of this study was to evaluate the validity and reliability of the Spanish version of the Technological Competency as Caring in Nursing Instrument (TCCNI).
Methods
An observational, quantitative, test validation, psychometrics-type study was conducted between 2012 and 2014 with a population mainly from Bogotá; however, data collection was extended to cities, like Medellín and Cali.
Linguistic validity. For this validity, the study selected two official American English language translators from the Colombian Ministry of Foreign Relations and Justice. In addition, two nursing professionals were selected who spoke American English and had knowledge of the TCCN theory and who had professional experience in technological and labor environments in the United States and Canada, which permitted contextualizing the technical language and that of the profession. Further, expert assessment was made of the quality of the English to Spanish translation with a linguist familiarized with medical terminology. Lastly, a third official translator re-translated the instrument. This last version was carried out after approval by the expert evaluators in the face and content validity and, finally, with approval from the instrument’s author.
Face validity. Two groups were established: the first, to see the behavior of the instrument and evaluate the need to make adjustments in semantics and ease of reading. This group comprised 17 nursing professionals who coordinated different hospital care services and who had been contacted via email. The second group was a panel of experts, selected with the profile of specialists and knowledgeable of technological services, nurses with at least five years of teaching experience and work experience in clinical service over 10 years. Contact was made through email, which contained the invitation to participate in the study, the justification, the objective, and study instrument to evaluate. The invitation was sent to 20 experts of which only 10 accepted to participate. The experts scored each item (0 = does not comply and 1 = complies) from three criteria: Comprehension, Clarity, and Precision. Furthermore, they made their respective observations and recommendations. With the results from this phase, Lawshe’s modified content validity index12 was determined to define inter-observer agreement among judges with Fleiss’ kappa index.13
Content validity. This phase had the participation of the 10 experts who conducted the instrument’s face validity. An evaluation was requested of each item under the criteria of Pertinence and Relevance, and each of the scored, as mentioned by Denise Polit 14) with 0 = Not pertinent/relevant, 1 = Poorly pertinent/relevant, and 2 = Pertinent or relevant. Analysis of the data obtained was verified with Lawshe’s modified content validity index; to determine inter-observer agreement among judges, the study used Fleiss’ kappa index.13
Construct validity. This phase permitted measuring the instrument in the object population of nursing professionals from hospitalization areas. Sample determination was based on the classical instrument validity theory according to Henson and Roberts 15 and Beavers,16 who propose 10 subjects per variable. According to this, the option was a calculated sample of 250 participants (n = 25 items times 10 participants) and 255 nurses participated. The information obtained was tested for factor analysis of principal components extraction and the Varimax rotation method with Káiser-Meyer-Olkin and Barlett’s sphericity test.
Evaluation of reliability. The internal consistency of the instrument was evaluated with Cronbach’s alpha coefficient.
Techniques and information collection. The invitation to participate in the study was sent via email, after selecting the nursing professionals who complied with the following inclusion criteria: working in services (surgery, recovery, hemodynamics, renal units, adult intensive care, emergency, cardiac rehabilitation, and hospitalization) or studying in any graduate program (emphasis in cardiovascular, critical care, cardiac rehabilitation, nephrology, emergency, perfusion or cardiorespiratory surgery); or with knowledge, experience, and studies in managing technological machines (training, courses, specializations), and with at least one year working in services. Exclusion criteria involved nursing professionals who worked in administrative areas, public health, epidemiology, and teaching. The study sought nursing professionals from Bogotá and from other cities in Colombia to broaden the context of the instrument and not limit it to the country’s capital.
Ethical considerations. The study considered Resolution 8430 of 1993 and Legislation 911 of 2004, chapter IV, articles 29, 30, and 34 of the Republic of Colombia. This research was approved by the Ethics Committee of the Faculty of Nursing at Universidad Nacional de Colombia. All the phases had informed signed consent from the participants, after receiving explanations on the nature of the study.
Results
Linguistic validity. It was found that in items 2 and 7 of the original instrument in English there was no clarity in the sense of the words “What” and “Who”. Through the accompaniment of the instrument’s author it was clarified that the words asked, “what is” and “who is” the person. Item 3 conducted an exhaustive consensus with the experts regarding the discussion on the Word curing or healing, contextualizing it in everyday professional language in nursing; and the term saving the patient, whose sense in item 3 is: increases their self-sense, to finally write this item as: “the purpose of nursing is healing - saving lives and increasing self-sense”. The rest of the items presented favorable acceptance by the translators, experts, and the linguist.
Face validity. Bearing in mind that Lawshe’s modified content validity index must be above 0.5823, this criterion was fulfilled in most of the items with clarity of 0.86, precision of 0.83, and comprehension of 0.89. The agreement of Fleiss’ kappa index showed substantial agreement in clarity and precision (0.75 and 0.72, respectively) and almost perfect agreement in comprehension (0.81). Inter-observer agreement evaluated with Fleiss’ kappa index coefficient had a global average of 0.8, with this result being highly satisfactory.
Content validity. Lawshe’s modified content validity index of the criterion of Pertinence was 0.9, being a high degree of agreement among experts and in the criterion of relevance of 0.9, considered a highly important result. Expert evaluation of the concordance performed through Fleiss’ kappa index obtained 0.82 in the criterion of relevance and 0.82 in the criterion of pertinence, which indicates high acceptability in coherence and concordance, being almost perfect in the evaluation of the Spanish version TCCNI. Additionally, the work considered the recommendations and qualitative observations of experts of the items to draft the final version of the instrument.
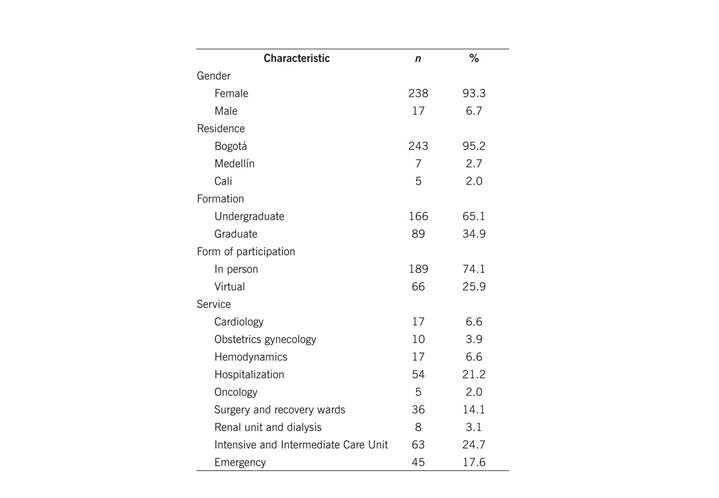
Construct validity. This phase reports the data from the 255 participating nursing professionals of which 189 participated in person and grouped according to the institution and area of service. These participants were briefed about the research and voluntarily accepted to participate in it. Regarding the virtual participation, the instrument was created online with the google questionnaire form comprising: invitation, research presentation, informed consent, and instrument. The online invitation was sent via email, having previously selected those who complied with the criteria established for this research. Of the 115 email invitations, only 66 participated by answering the questionnaire; of the total participants, in the professional profile 93.3% were females; 65.1% of the participants had only undergraduate education, and most were assigned to high-technology services, like cardiology, obstetrics gynecology, hemodynamics, hospitalization, oncology, surgery and recovery wards, renal unit and dialysis, intensive and intermediate care unit, and emergency (Table 1).
Factor analysis. The factor analysis with the extraction method was used, along with principal components and Varimax rotation. Prior to the factor analysis, adequacy indicators were obtained of the items to the factor analysis. The Káiser-Meyer-Olkin sample adequacy measurement was 0.85, proving good sample adequacy paired with Barlett’s sphericity test of approximate chi square of 1840.58. Anti-image matricity in extraction by the principal components method and Varimax rotation method permitted generating six factors that had a total accumulated variance of 54.16%. Table 2 shows the explained variance of each item per component.
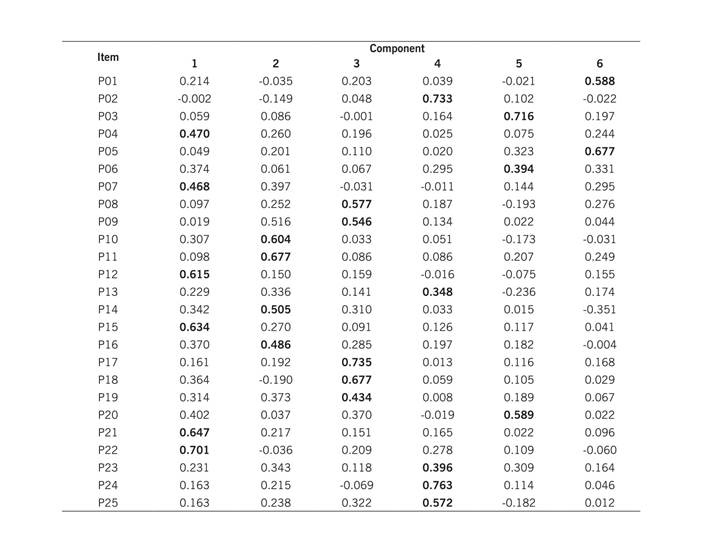
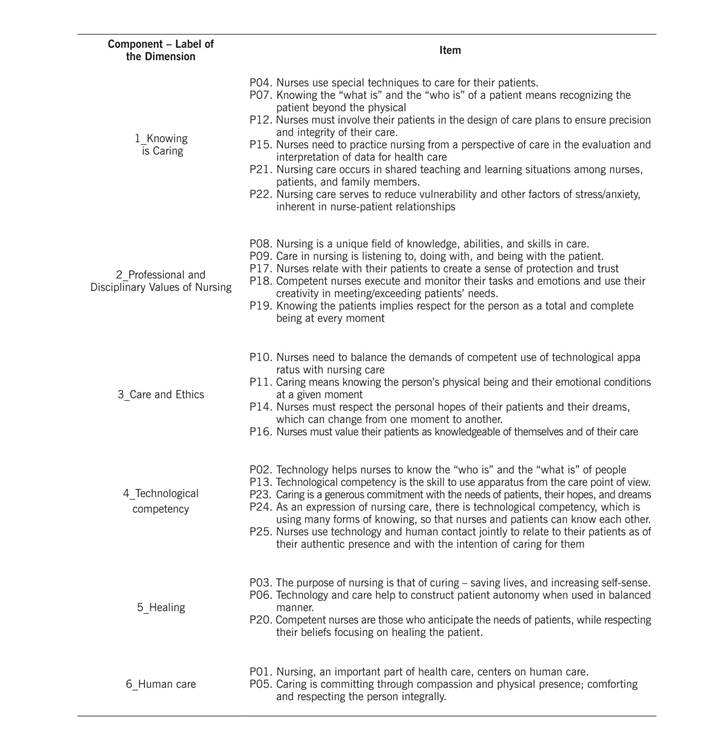
Through the variance report with the Varimax Rotation Standardization method with Kaiser, it was possible to identify six components of the instrument, one more than in the instrument, selecting those items from the instrument that provide the greatest variance by component. Because these are generated in the instrument, each component or dimension is labeled, based on the assumptions and concepts of the TCCN theory (Table 3).
Reliability. The internal consistency of the TCCNI in Spanish was 0.88.
Discussion
The instruments, as empirical indicators of the nursing concepts and theories, are required to advance in knowledge. It is a challenge for these to be truly based on theory for which the TCCNI fulfills this criterion by being based on a series of its own theories and widely known philosophical postulates.
The methodological requirement in the language transcription from the TCCNI was an aspect worth highlighting in this study, given that recommendation by the Mapi Research Institute17) and Jaimes et al.,18 were followed. This work also received permanent accompaniment and feedback to the process from the TCCNI author, which is not always viable in instrument validation processes.
Among the words that had to be revised in the linguistic validity were Healing or Curing, rescued by Jean Watson3 as an important result of nursing, supported principally by the spiritual component of care and which recognizes that perspective that moves away from the biomedical paradigm that had impregnated nursing in its beginnings. Likewise, it was found that the fact of “increasing self-sense” is now necessary in nursing, given that we no longer have a person traditionally recognized as a patient, rather, the act of caring is a process of interaction and nutrition between two people, coherent with that proposed by Boykin and Shoenhofer.4 These theoretical perspectives rescue concepts that really belong to nursing that are often invisible in care, which confirms the need to rescue the theoretical disciplinary background.
The results found in face validity through the FVI are adequate according to that proposed by Tristan in the modification of Lawshe12) of being above 0.582. In obtaining the degree through Fleiss’ kappa index, the results confirm the correlation among the experts, which were finally 10, surpassing Polit’s recommendation of three experts14 and that by Tristan of a minimum of five experts.12) The sociodemographic characteristics of the nursing professionals in this study are similar to populations in intensive care units in Brazil19 and Colombia,20 which indicates that these professionals require some important experience; rarely, are these people younger than 30 years of age. In addition, quite often they require formal specialized formation or technical courses.
The TCCNI is among the few found in literature that does not focus attention on the description of technology, but which harmoniously gathers the characteristics of human care and technology from skills and expertise. This may not be attractive for those seeking to measure technological behaviors and not care in technology. Due to this, it may be felt that it is viable to apply the instrument in any context that does not necessarily have high technology, but minimum technology, like a thermometer, blood pressure meter, glucometer, among others, but necessary in basic nursing care.
This instrument had no published evidence of its own dimensions. The author provided, via email, the five dimensions from the theoretical assumptions. However, based on the area with the Varimax standardization rotation method with Káiser, others were identified that may better reflect the concept of technological competency in Colombia. The dimensions were: 1_Knowing is Caring (originally called Knowing the people/patients): found in items: (4, 7, and 15) that correspond, according to Locsin, to the dimension of “knowing the people”, followed by items 12 and 21 that belong to the dimension of “Nursing as Discipline and Profession”, and item 22 belonging to the dimension of “technological competency”. 2_Professional and Disciplinary Values of Nursing (originally called Knowing the people/patients): is constituted by items: (8, 9, and 19) corresponding to the dimension of “knowing the people”, item 17 of the dimension “Nursing as Discipline and Profession” and item 18 belonging to the dimension of “people as participants of their care”. 3_Care and Ethics (originally called Cares in Nursing): had the peculiarity of maintaining the three only items of the dimension “Cares of Nursing” items: 10, 11, and 14. Item 16 was added, belonging to the dimension of “people as participants of their care”. 4_Technological competence (originally called Technological competency): is constituted by four items of which three belong to the dimension of “Technological competency”. The additional, item 2, belongs to the dimension of “Nursing as Discipline and Profession”. 5_Healing (originally called People as participants in their care): this dimension has items 3 and 20 from the dimension “People as participants in their care”, and item 6 that belongs to the dimension of “Nursing as Discipline and Profession”. 6_ Human care (originally called People as participants in their care): a dimension constituted by only two statements, item 1 belonging to the dimension of “People as participants in their care”, and item 5 belonging to the dimension of “Knowing people”. The dimension of Nursing as discipline and profession was not visible statistically as a grouping of items, but such were part of other dimensions.
Studies that have reviewed care in environments with technology reconfirmed the need to have elements of human visitation,21 technical skills and direct care,22 interpersonal23 and inter-professional21 interaction, and the search for visible results in health principally in the biomedical area.24 The TCCNI does not center its results on any concrete indicator of physical health; rather, it contemplates health as healing, which is the search for the equilibrium of the human being in constant interaction with the caregiver. The reliability results of the TCCNI are within the expected interval proposed by Carvajal, corresponding to 0.8 and 0.9, classified as excellent.25
Among the limitations of the study, we have that the TCCNI may have measurement bias, given that the instrument used is a relatively new research tool in the world and these are the initial studies within the nursing context and specifically in the Latin American context.
To conclude this study, it may be said that the TCCNI has adequate psychometric properties in terms of reliability and validity, which will allow this instrument to be used to measure the technological competency of nurses with similar characteristics to those of the study group.

