











 text in
text in  English (pdf)
English (pdf)
 Article in xml format
Article in xml format Article references
Article references
 Send this article by e-mail
Send this article by e-mail Cited by SciELO
Cited by SciELO  Cited by Google
Cited by Google  Similars in
SciELO
Similars in
SciELO  Similars in Google
Similars in Google 
 Permalink
PermalinkIntroduction
The Manchester Triage System (MTS) was created in England in 1994 and has been adopted in most emergency services (ES) as a guiding tool for risk classification. In Brazil, patient triage systems emerged in 2002 and the MTS is the most frequently used among them. The use of the MTS has been a requirement of the state government of Minas Gerais since 2007, as part of the regionalization master plan of the state to which all municipalities must adhere.1
In Portugal, the MTS was implemented in 2000, initially in two hospitals in Coimbra. At present, the system is used in 60 urgency services and it is in the process of implementation in others units, although it is considered indispensable for the organization and administration of such services in the country.1) Emergency and urgency rooms have been mistakenly seen as the first choice of care by users, even in situations where the most apropriate service is not that provided in first-aid posts.2,3. This generates overcrowding, disorganization of care and dissatisfaction among the population. For this reason, new ways of organizing the flow of users in the health service are necessary.4 In an attempt to remedy these problems, the Ministry of Health in each of these countries has taken actions seeking to organize emergency and urgency services, in order to meet different levels of specificity and resolution in the assistance provided to emergent or urgent grievances. One of these actions is the reception with risk classification.4,5
Risk classification is a dynamic process where patients are evaluated as soon as they arrive at the service. This ensures that high-risk users receive immediate care and reduces the waiting time for medical care, depending on the degree of priority assigned to each user, decongesting emergency rooms, determining the primary care area and referring users to specialties, according to the guiding protocol.1 The assignment of degrees of risk to patients consists in a complex decision-making process. Nurses have been the most indicated professionals to perform this task. Protocols have been used to guide the prioritization of care.6,7
The MTS includes levels of priority, color to be assigned, and an estimative of waiting time for medical care. Based on the identification of the user's main complaint by the nurse, a specific flowchart guided by discriminators presented in the form of questions is selected. There are 55 different flow charts and a risk scale that, depending on signs and symptoms, classifies the situation of the patients into: emergent (red), very urgent (orange), urgent (yellow), not urgent (green) care to be provided between 0 and 240 minutes.1 A study carried out in Brazil compared the MTS with an institutional classification system showing that the former is more inclusive and increases the priority level of the classified patients.8
In a study carried out in Portugal, the MTS was useful to distinguish patients who needed emergency care from the others.9 Brazil and Portugal have similar health services; in both, the health system is controlled by the State, is ruled laws of the Federal Constitution and is under the responsibility of the Ministry of Health. Principles of universality, comprehensiveness, gratuity and validity throughout the national territory are also guaranteed in both countries. In Portugal, fees are charged, which are not intended to finance the system, but rather to limit unnecessary access to certain services. Moreover, the MTS in the emergency services has been adopted as a guiding protocol in the two countries. Thus, the system data such as complaints, colors, stratifications, severity, time of service, and so on, can allow valuable analyses. The patients' behavior towards the classification of risk has been studied by authors from several countries.9-11 The predictive validity of the classification is understood as the affirmation of the patients' correct classification, based on their clinical evolution and length of stay in urgency and emergency services.12 Considering that the implementation of the MTS in Brazil was assisted by the Portuguese Risk Classification Group and that the MTS has not been translated, adaptated and validated for its use in Brazil, a study evaluating the prediction of the protocol in these two countries is necessary. The present study aimed to evaluate the outcome of patients classified through the MTS in two large hospitals, one in Brazil and the other in Portugal.
Methods
This is a historical cohort study carried out in two hospitals in different countries: the emergency service (ES) of the Hospital Centre and University of Coimbra (CHUC), Portugal, and in the ES of the Odilon Behrens Municipal Hospital (HOB) of Belo Horizonte, Minas Gerais, Brazil. They share common characteristics: both are large hospitals, and references for urgent care in municipalities and regions. The CHUC is a national reference in clinical and surgical areas of various medical specialties, besides offering field of internships for undergraduate, graduate and research programs. The HOB is also a teaching hospital and a state reference in trauma, and clinical and surgical care of various medical specialties. Both have medical and multiprofessional residency programs in various specialties. The study population consisted of all the patients who entered the ES in both hospitals, who passed through the triage room between January 1st and December 31st, 2012, and were triaged by nurses using the MTS.
This study used data obtained from the ALERT software®, which is a management system for risk classification of patients employing the MTS as the guiding protocol. In Brazil, it was necessary to collect data from the HOSPUB system®, which is used for inpatient registration. This system makes it possible to calculate the length of stay, based on the clinical outcome of patients in the institution.
The five categories of classification were always compared with the color considered of lower priority in the service, the "blue" category. This was applied to the length of stay. For analysis of the risk of death, data were evaluated in relation to the "Green" color, because deaths did not occur in the "blue" category in either country.
Patients classified in the "white" color were excluded from statistical analysis because this is a category that refers to hospital returns or administrative appointments, which are not emergency cases. A total of 13 968 (9.0%) patients were classified as "white" in Brazil, and 4 244 (2.7%) in Portugal. The sample consisted, therefore, of 158 959 cases in Portugal and 155 121 in Brazil, in the year 2012.
Evolution to hospital discharge, transference, abandonment of treatment and death, as well as the length of stay of the users who sought the emergency service within the stipulated period were considered as "outcome". The following data were surveyed: age, sex, MTS classification (red, orange, yellow, green and blue) and flowchart.
Data were submitted to statistical analysis in the software Statistical Package for Social Sciences (SPSS), version 19.0. Descriptive statistics with frequency and inferential analysis were used for characterization of patients. In order to measure the strength of association between exposure and outcome, the Relative Risk (RR), the 95% confidence interval and the p value were calculated. Median was used for length of stay, which corresponds to the 50th percentile. Logistic regression was performed to control confounding variables.
The study was approved by the Research Ethics Committee (REC) of the Odilon Behrens Municipal Hospital and the University Hospital of Coimbra, under Opinion nº 834 973/2014 and nº 0110/2013, respectively.
Results
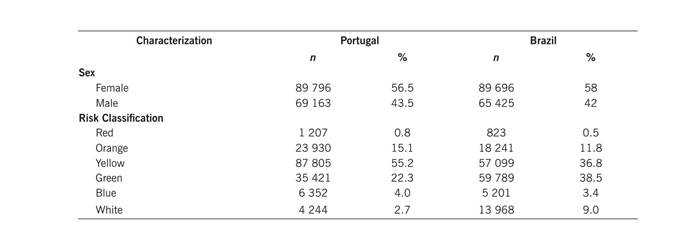
Among the patients analyzed in the Portuguese group (158,959), female subjects predominated (56.5%), with mean age of 54 years and standard deviation of 21.1 years, minimum of three days and maximum of 112 years. In the Brazilian group (155,121), female subjects (58%) were also predominant, with mean age of 32 years and standard deviation of 22 years, minimum of four days and maximum of 114 years. The characterization data is presented in Table 1.
Table 1 Sex distribution and risk classification of patients assisted in the emergency service. Portugal, 2012 (n = 158,959), Brazil, 2012 (n= 155,121).
The main complaints of patients attended at the institution in Portugal were: adult malaise (22 679 - 14.3%), problems in the extremities (18 810 - 11.8%), problems in the eyes (12 150 - 7.6%), obstetrics/gynecology (11 253 - 7.1%), dyspnea (9 234 - 5.8%), and abdominal pain (8 830 - 5.6%). In Brazil, problems in extremities (21 627 - 12.9%), obstetrics/gynecology (13 300 - 7.9%), abdominal pain (12 471 - 7.5%), dental problems (9 892 - 5.9%), headache (9 566 - 5.7%) and thoracic pain (6 447 - 3.9%) were the most frequent flowcharts.
Regarding the length of hospital stay of patients in Portugal, 2 264 (9.2%) stayed hospitalized for less than 1 day; 4 501 (18.3%), from 1 to 3 days; 10 753 (43.7%), from 4 to 10 days; 4 329 (17.6%), from 11 to 20 days; 2 738 (11.1%), for more than 20 days, and the maximum length of stay was 276 days. Of the total number of patients studied, 130 536 were admitted to the ES and discharged within 24 hours, and were not hospitalized. In the case of patients in Brazil, 75 175 (48.4%) stayed in the hospital for less than 1 day; 8 799 (5.7%), from 1 to 3 days; 67 074 (43.2%), from 4 to 10 days; 1 744 (1.1%), from 11 to 20 days; 1 739 (1.2%), for more than 20 days, and the maximum length of stay was 518 days. This information was not obtained in the case of 590 patients (0.4%). In Brazil, the variable "less than 1 day" refers to the patients who entered into the ES, received assistance, and were discharged within 24 hours or were hospitalized for less than one day.
Statistically significant difference of length of hospital stay was found among all groups of patients in the two cases studied. The five categories of classification were always compared to the color considered of lower priority in the service, i.e. the "blue" category. Thus, the higher the priority of the patients, the longer they would remain in the hospital (Table 2).
Table 2 Analysis of length of hospital stay of patients in relation to risk classification groups based on the MTS. Portugal, 2012 (n= 158 959), Brazil, 2012 (n= 155 121)
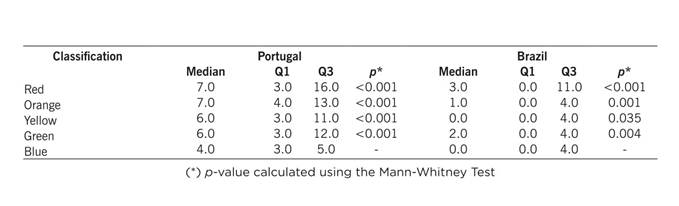
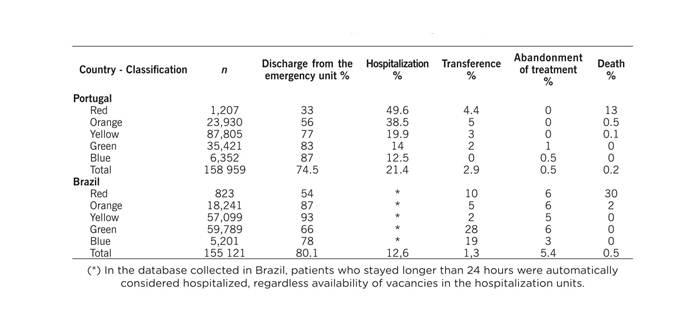
Table 3 presents the outcomes of patient care in the emergency units of the hospitals studied in Portugal and Brazil. Notably, in both cases, discharge numbers are high, and in Brazil, treatment abandonment is more frequent. The relationship between patients classified as red and the outcome of death is also outstanding in both hospitals.
Table 3 Distribution of frequency of care in relation to outcome and risk classification in hospitals in Portugal and Brazil
For the two groups studied, the risk of death in each risk classification color was determined through the calculation of Relative Risk (RR). It was observed that, for the two groups studied, the higher the patient's priority, the greater the risk of death compared to the "Green" classification group (Table 4).
Table 4 Risk of death among patient groups by color classification. Portugal, 2012 (n =158 959), Brazil, 2012 (n =155 121)
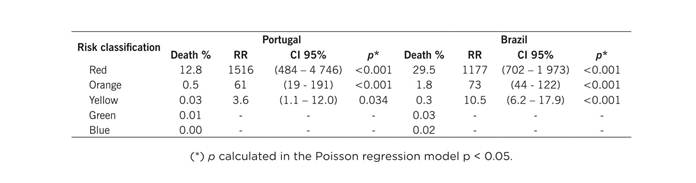
Patients classified in the red category in Portugal had 1516-fold higher risk of evolving to death compared to those classified in the green category. In Brazil, patients classified in the red category had 1177-fold higher risk of evolving to death when compared to those classified in the green color.
Discussion
It was noticed that the majority of patients who sought care in the hospitals of Portugal and Brazil were female (58% and 56.5%, respectively). This result is similar to studies carried out in Brazil13 and in Portugal.14 In Brazil, the mean age of the population was lower (32 years) than in Portugal (53 years). A study conducted in Brazil found that the mean age was also 32 years.15 This indicates greater aging of the Portuguese population when compared to the Brazilian population. As for risk classification in the two hospitals, there were differences regarding the priority of patients. Patients classified in the categories with the highest clinical priority (red, orange and yellow) in Portugal had higher percentages when compared to Brazil: 71.1% and 49.1%, respectively. Portuguese reported 76.2% of the patients classified in the categories of higher clinical priority.9 In turn, a Brazilian study found 46.4% of the patients classified in the categories with the highest clinical priority.3
These data suggest that people who are in situations that are no urgencies continue to seek the ES as the main gateway to the health service in Brazil. This contributes to overcrowding the service, and hampering the resolubility in basic care services.15 The study showed that the Brazilian hospital had more patients classified in the white category (13,968 - 9.0%) than the Portuguese hospital (4,244 - 2.7%). This finding may be related to the fact that patients referred by doctors from other services to the hospital in Brazil, such as Basic Health Units and Emergency Care Units, are classified in the white category. It is worth mentioning that the flow of patients from other municipal services is quite intense, since several specialties and diagnostic tests are only available in the HOB. In Portugal, patients are classified and the category assigned guides their transference to hospitals close to the patients' residence, medical indication, realization of programmed techniques, among others. Thus, a difference was detected between the two countries with respect to the system of patient referral.
Among the six most frequent flowcharts analyzed in both countries, abdominal pain and gynecological/obstetric problems were present. It is important to know the complaints that lead people to seek the ES so that health care levels may be organized based on the degree of severity of complaints, in order to better meet the demand in each level.16 In Portugal, 130,536 people entered the ES and were discharged in less than 24 hours. In Brazil, this number dropped to 75,175 people. This may be related to the fact that health care in Portugal is public but still paid, which means that the population opts to go to ES because of technological resources and different professional categories gathered in the same environment. In Brazil, the health service is public and free, in the case of basic health units and the hospital area. People classified into little urgent or non-urgent categories should initially seek basic health units and have their needs met there. The purpose of basic units is to try to solve 85% of the health demands of Brazilians; needs that are not contemplated in this level are to be referred to services of greater technological complexity. It is suggested that further studies investigate this theme.3 Regarding the length of stay in hospitals, it was observed that numbers are higher in the Portuguese hospital. This data may be related to the increase in age (53 years) and the prevalence of chronic diseases in that country, which require longer hospitalization times to stabilize the disease.
The greater the clinical priority (red, orange and yellow), the longer was the stay in both hospitals. Statistical significance was found between the length of stay and MTS colors. The findings of this study corroborate a research carried out in Brazil in which more severe patients stayed hospitalized for longer periods when compared to those of lower clinical priority.11 Thus, the MTS can be considered a good predictor for length of hospital stay of patients of high clinical priority when compared to those of low clinical priority. Regarding the outcome of the patients, it was observed in both countries that the lower the urgency (blue, green and yellow colors), the higher the number of discharges , and the lower the number of deaths. This is in line with a study carried out in the Netherlands and another carried out in Portugal.9,10 However, whereas the behavior of patients in relation to severity in the classification corresponds to an equivalent distribution in hospital stay and outcome (discharge and death) in Portugal, the majority of patients was discharged in Brazil, indicating that less severe cases continue to seek ES in Brazil.
The univariate analysis showed that there is statistical difference between risk classification groups in relation to death. It is reasonable to expect, thus, that the greater the severity of the patient, the greater the risk of evolving to death, showing that MTS is a good predictor of death, as it has been pointed in other studies.11,13,15 The lack of a unified database for patients who entered the ES and were admitted to the hospitals studied represents a limitation of the study. It was necessary to resort to different databases to find the outcome of the patients. Ideally, the ALERT® should bring together all the information.
Conclusion
The MTS was introduced in Brazil more recently when compared to Portugal. It is still necessary to organize health services so that the emergency units responsible for providing care for seriously ill patients and also the reference and counter-reference systems may work better. Assistance to cases of lesser seriousness should be provided without involvement of levels of greater complexity, in services such basic health units. This restructuring will make it possible to reduce overcrowding and offer a more resilient service in both countries. The fact that the population of Portugal with higher levels of clinical severity seeks ES may be related to the fact that the health system is paid. We suggest that further studies be conducted with the aim to compare data from the emergency department of free and private hospitals (with and without health insurance plans).
In both countries, the MTS proved to be a good predictor of hospital stay and death outcome, confirming data from national and international surveys.

