











 texto em
texto em  Inglês (pdf)
Inglês (pdf)
 Artigo em XML
Artigo em XML Referências do artigo
Referências do artigo
 Enviar este artigo por email
Enviar este artigo por email Citado por SciELO
Citado por SciELO  Citado por Google
Citado por Google  Similares em
SciELO
Similares em
SciELO  Similares em Google
Similares em Google 
 Permalink
PermalinkIntroduction
The parturition process is a complex phenomenon due to different factors that interact amongst themselves,(1) which can increase the risk of complications and death, and which additionally affect the mother’s wellbeing. Likewise, women during the parturition process report feeling mainly fear,(1-3) which alters their performance and comfort, especially in primiparous.(1) These negative emotions,(1) constant pain, affectation in the capacity to make decisions,(4) communication difficulties with the health professionals,(1) and care guided with biological approach translate into negative perception toward the care givers and the parturition.(4)
For women to have a positive experience,(4) participation is recommended from nurses trained and experts in obstetrics during parturition care,(5) given that this favors the naturalness of the event and diminishes rates of caesareans and complications. Through humane care, they can reduce potential problems that arise;(6) however in practice, nursing care is provided routinely,(7,8) with knowledge of the task involved, but without disciplinary theoretical orientation, and although they are suitable professionals to achieve broad benefits and satisfaction of the woman during the parturition process, little time is assigned for this purpose, dedicating over 70% of the time to objectives different from specific care(8) due to different barriers(9) identified by the nurses and by the women.
Even so, nurses have been seen as leaders(10,11) to favor empowerment and control during the parturition process;(10) women value individualized information, explanations, advice, and nursing care(2) and identify the professionals as humanized, respectful, and sensitive to the women’s expressions of pain and joy;(2) however, these perceptions are sporadic.
In light of this panorama, it is necessary to provide care based on the theory of the discipline that permits appreciating benefits and wellbeing during the parturition process. Swanson’s theory of nursing as informed caring for the well-being of others(12) is the support of the intervention proposed in this study, which guides nurses through the five care processes proposed: Maintaining belief in the woman’s capacities to confront the situation, approaching with affection, offering hope and favoring autonomy;(1) Knowing the meaning of the event, without judgments and understanding specific manifestations; Being with - listening to concerns, being available, offering emotional support, and understanding feelings; Doing for - offering physical measures of comfort and information, controlling fear and pain;(2) Enabling - protecting the woman from any type of harm and favoring self-care, guiding in the process. A theoretical analysis was performed and, supported by existing evidence, the specific activities were constructed for nurses to apply care processes during the parturition process.
Seeking to compare the assessment of nursing care offered during the parturition process in the intervention group based on Swanson’s theory of caring versus that of the control group, which received conventional care, the intervention proposed was applied and nurses were evaluated, in both groups, with the Professional care rating scale by the same author.(13)
Methods
This was a preventive-type controlled clinical trial. A minimum sample size was calculated of 20 women for each of the study groups, bearing in mind an alpha value of 0.05, a beta value of 0.8, and a minimum difference between groups of 8 points for the scale total. The participants were women over 14 years of age who were hospitalized to care for the parturition process in the maternity service at the Regional Hospital in San Gil, Santander (Colombia) during the period from September to November 2016, and who signed the informed consent.
Assignment of the women to the study groups was done according to the day they were hospitalized during labor. The control group was comprised by the mothers who received conventional care from the maternity service staff plus the skin-to-skin contact during the immediate postpartum, while the intervention group was provided care based on the care processes proposed by Swanson in the Theory of informed caring for the well-being of others.(13) For this intervention, a last-year Nursing student was trained through 6 h of theory, 5 h of supervised practical hours, and 40 h of independent practice on the specific activities of the intervention proposed to be applied during labor and expulsion.
During the immediate postpartum, another last-year Nursing student who ignored to what group the mothers had been assigned, applied the Professional care rating scale based on Swanson’s theory of caring(13) to the participants from the intervention and control groups. The rating scale has 15 items with four Likert-type response options: 1 = never, 2 = sometimes yes, sometimes no, 3 = most of the time, and 4 = always. The general classification of professional care is considered according to the total score, thus: <23 = Deficient; 23 to 37 = Regular; 38 to 51 = Good; and 52 to 60 = Excellent (14). The scale applied received semantic validation for Colombia with excellent reliability (Cronbach’s alpha: 0.90).(14) To store the information, the study used an electronic device with the scale aggregated, connected to an immediate response to the principal researcher’s e-mail and a meticulous record of the women’s answers was kept.
This research was approved by the Ethics Committee of the Faculty of Nursing at Universidad Nacional de Colombia and by the Ethics Committee at the Regional Hospital in San Gil. Respect for the dignity of the women prevailed, along with the protection of their rights, and their wellbeing. The study kept in mind the ethical principles contemplated in Legislation 911 of 2004: Beneficence, Non-maleficence, Justice, Autonomy, Fidelity, and Reciprocity. The study was classified as minimum risk and participant information confidentiality was protected.
Results
During the study period, 107 women in labor were admitted to the Hospital’s maternity service, 43 of them fulfilled the inclusion criteria; 20 were assigned to the intervention group and 23 to the control group.
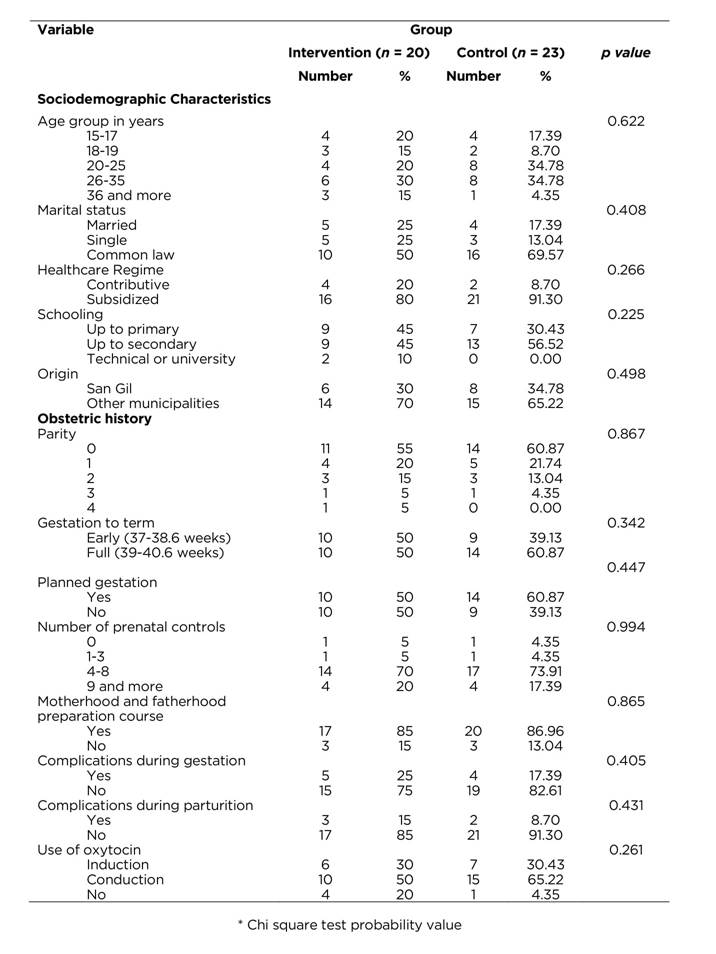
Sociodemographic characteristics
The mean age in the intervention group was 25.15±7.91 years versus 24.35±5.77 years in the control group (p = 0.893). Table 1 shows that the groups are similar regarding the sociodemographic variables and obstetric history. Most of the women in both groups are between 20 and 35 years of age, are registered in the subsidized regime and report their level of studies to complete secondary. Other common characteristics in these women is that they come from municipalities near San Gil to have their first parturition, with gestations at full term, having as antecedents compliance of prenatal controls and attendance to the motherhood and fatherhood preparation course. Principally, the women in both study groups had no complications during gestation or labor. The parturition lasted 14.85±12.11 h in the intervention group versus 17.65±10.45 h in the control group (p=0.420), with this difference not being statistically significant.
Results in the Professional care rating scale
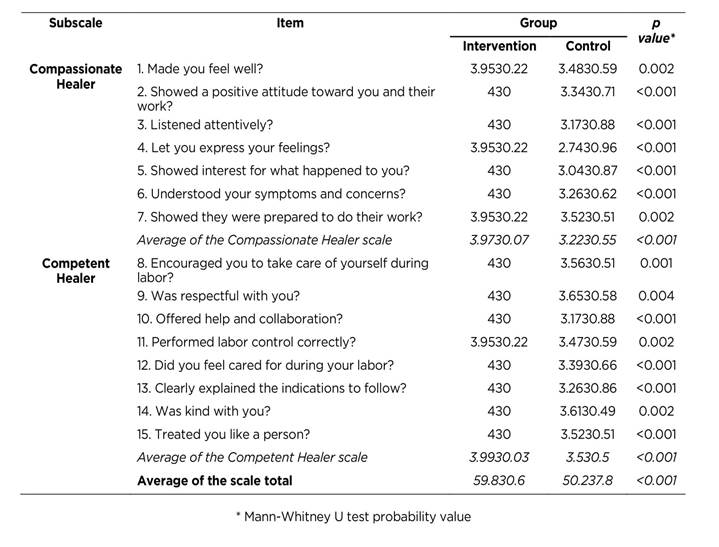
Assessment of professional care in the intervention group was Excellent (average 59.8±0.6, minimum = 58, maximum = 60), while the control group was Good (average 50.2±7.8, minimum = 39, maximum = 60). Table 2 reviews the average values obtained in each of the items, which per subscale and scale total were higher in the intervention group compared to those of the control group, and all these differences were statistically significant. Specifically, in the intervention group the scores of the 15 items were between 4 and very close to 4 (3.95-3.97), indicating that the questions were mostly answered with the option “always”.
Table 2 Averages per item, subscale, and scale of the Professional Care Rating Scale according to study group
It was not found that the scale’s total score was affected by possible interactions between the study group with the variables of use of oxytocin (p = 0.85) or time of labor duration (p = 0.57).
Discussion
Most of the women in parturition process for both groups are within the age group 20 to 35 years, corresponding to the ages of highest rates of fertility for Colombia,(6) an important variable given that the two extreme groups, adolescents and women over 35 years of age are of obstetric risk. These data reiterate that found in Europe, Latin America, and Colombia where similar ages are reported.(1,15-17)
Women hospitalized for the birth of their children came from municipalities close to San Gil and many had basic primary and secondary studies, differing from data reported in other Colombian studies(15,18) in which between 50% and 60% of the women had higher levels of schooling; in this research, <5% had this level of schooling and it may be because most of the women come from small towns near San Gil, while the Colombian studies were held in Bogotá in sectors with prevalence of high socioeconomic level.(15,18) This reveals the need for intervention to women in parturition process in this province or in regions with similar characteristics. More than half the women were in the parturition of their first child; research in different continents report predominance of primiparous women,(1,15-20) which shows that, in general, women are in a group that requires greater care because they are upon the birth of their first child. Changes of different intensities occur during the parturition process, which behave as a complex phenomenon, especially for the primiparous women, who feel more fear than multiparous women (1); thus, the interrelationship with nurses improves the woman’s performance and wellbeing during the parturition process. It must be highlighted that the parturitions occurred in pregnancies with gestational ages to term, which require principally of care and of the nurse’s continuous presence(7,21) to contribute to the naturalness of the process.
Most of the women reported that their gestation was unplanned and this has been associated to the development of post-traumatic stress;(7) additionally, they comply with prenatal controls, but do not attend the motherhood and fatherhood preparation course - although they required it because most were primiparous. This corresponds to a wake-up call for care to be offered from the initial stages of gestation to the moment of parturition; the nurses’ presence and the support they provide during labor can diminish the onset of postpartum stress.(22)
Regarding the results of applying the Professional care rating scale, it was noted that the score was higher in the intervention group compared to the control group, showing the benefits of applying this care intervention during the mothers’ parturition process. These data are a reminder that women request and grant importance to the relational component of nursing care, which influences upon the care assessment, corresponding to that found in Latin American studies.(15,18)
Given that the participants from the intervention group scored the 15 items from the scale with values around 4, it is important to analyze some items in the control group that deserve attention: the reactive with the lowest score was # 4- Let you express your feelings? (2.74), which beckons nurses to keep in mind activities from the process “Being with”, broadening care toward feelings, remembering that women during parturition process have mixed feelings.1 Item 1- Made you feel well? Obtained an average score in the control group of 3.48. By using the linear interpolation of the averages of each item from the scale with its total score, it was found that this score corresponds to the lower limit for professional care considered Excellent, hence, the care process “Maintaining belief” requires being delved into by nurses who apply the intervention.
In the Competent Healer subscale for the control group, the lowest average scores were: 13- Clearly explained the indications to follow?; and 10- Offered help and collaboration?, which calls on nurses in general to improve in the education and direct care of women during parturition process; these scores obtained a classification of Excellent in the intervention group. It should be remembered that women who do not feel cared for by nurses report development of postpartum post-traumatic stress (7, which drives to continue delving into this care intervention and its benefits during the parturition process, expulsion and in the immediate, middle and late postpartum.
The scale’s total score for the women who received intervention was in the category of Excellent, while being classified as Good for the control group, which agrees with the data found in other research,(23) which also applied during prenatal control an intervention derived from Swanson’s theory of caring, with before and after measurements, and finding that women value nurses better after the intervention.
Finally, it was observed that in this study’s care intervention, the scores were equal in both subscales, that is, they keep in mind the care aspects of Compassionate Healer and Competent Healer, while for the control group the score of the Compassionate Healer subscale was lower. Studies related to the nursing care offered to women during parturition process demonstrate that its evaluation is conceived through two components: one technical - less strong, but not less important - and another relational, considered the most important,(8,15) hence, the interrelation between the nurses and women influences directly on the perception of the care assessment .(15)
The conclusion herein is that the intervention derived from Swanson’s theory of caring was associated to a better assessment of the professional nursing care by women during the parturition process. Research should be conducted to continue with the assessment of this study’s intervention, as well as explore the different variables related to the process that can modify the scores manifested by the women in the subscales during the evaluation of the professional care and the variables susceptible to modification by the care intervention. Likewise, future research should review the impact of nursing care with evaluations at different times, like during the middle and late postpartum, as well as in women who have been programmed for caesarean.

