











 text in
text in  English (pdf)
English (pdf)
 Article in xml format
Article in xml format Article references
Article references
 Send this article by e-mail
Send this article by e-mail Cited by SciELO
Cited by SciELO  Cited by Google
Cited by Google  Similars in
SciELO
Similars in
SciELO  Similars in Google
Similars in Google 
 Permalink
PermalinkIntroduction
Quality of care is a theme of great interest and relevance for the nursing discipline. It is, in turn, a broad concept that involves elements related with infrastructure, process, and results of care.(1) Improving the quality of nursing care is a constant goal for the discipline and the first challenge to achieve it is to develop skills to evaluate and analyze the quality of care offered. In recent years, new elements have been included within the framework analyzing the quality of health care, guiding it toward the need to involve in this process the staff, providers, patients, and families.(2) Precisely, the voices of users, their expectations and needs, have been gaining strength as a guiding element of processes to improve the quality of health care.(3) In fact, the perception of patients and their families on the quality of nursing care has been explored in diverse studies, countries and contexts, manifesting that the quality of care is largely conditioned by the communication and interpersonal skills of the professionals.(4,5)
Said skills have a disciplinary support in Jean Watson’s theory of human caring, which highlights the importance of interpersonal and transpersonal attributes of coherence, empathy, and warmth in caring, which supports the need to approach the human component of care quality, from the patients’ perceptions.(6) With neonates, the parents account for the quality of care their children receive in the neonatal units and - in this sense - it is important to recognize that they face a complex emotional moment in which their expectations regarding care, as well as their perception of said care, can be conditioned by their child’s health status and by their own needs.(7) Hence, it is necessary to know the parents’ perceptions on the nursing care offered to their children to implement improvement processes and/or validate the nursing practice in caring for neonates, a task in which it is useful to apply instruments that permit approaching objectively the needs of the parents and neonates.
The design and validation of instruments to measure the perception of the quality of care is a strategy that has permitted identifying voids in care and improving care processes; however, said instruments have been scarcely applied within the context of neonatal care and although some instruments have been used in the area,(8,9) it is still necessary to broaden the analysis framework from the constructs and dimensions proposed by the different measurement scales available in nursing. The Caring Assessment Instrument (CARE-Q) was created by Larson in 1984 to determine the aspects patients consider relevant in their interaction with the nursing actions that are important for them.(10) This instrument has been used in diverse care contexts nationally and internationally,(11-14) being - according to the findings - a reliable instrument to know of the quality of nursing care. In Colombia, said instrument was validated in 2008,(11) where it obtained a Cronbach’s alpha of 0.88, after extracting four items from initial 50 in the original scale. Since then, this scale has been used in diverse hospital settings with adult patients;(13-16) however, no results were found to account for the application of the CARE-Q instrument in el context of neonatal care. This study sought to identify the perceptions of parents of neonates hospitalized regarding the quality of nursing care through the CARE-Q instrument.
Methods
This was a descriptive cross-sectional study, conducted in a neonatal unit of a private tier III health care institution in the city of Medellín (Colombia), serving as maternal and child care reference institution. The information was gathered from January to March 2015. The study included the parents of all the newborns admitted to the neonatal intensive care unit (NICU) and intermediate neonatal care unit (INCU), hoping that with a cross-sectional measurement during the fourth part of the year this would yield an adequate representation of what occurs with the study variables. During the three months 137 neonates were admitted and for a total participation of 121 parents. Sixteen parents, who fulfilled the inclusion criteria, did not participate in the study due to reasons, like death of the neonate, quick referral, among others.
The study included both parents of the newborns, who had accompanied their child for at least 12 h within the neonatal intensive care or intermediate care settings, whether continuous or not. Given that these are open-door units, the parents can enter during the schedule they wish during the 24 hours and the periods of accompaniment tend to be alternated with rest periods in their homes. El minimum time of hospitalization was confirmed with the date of admission, information from the staff, and information from the parents. No maximum hospital stay was established. The exclusion criterion considered parents with cognitive deficit. The parents were contacted in the unit by the principal investigator. With prior information of the study objectives and after signing the informed consent, the participants answered the instrument’s questions by their filling out the questionnaire; only in the case of illiteracy by the parent were the questions read. In all cases, the parents filled out the instrument in the neonatal unit, during a moment that did not interfere with care moments and while their child was asleep and tranquil. The questionnaire filled out was composed of three parts: i) sociodemographic aspects, ii) clinical information of the neonate (gestational age, weight, and days of hospital stay in NICU or INCU) and admission diagnosis), and iii) the CARE-Q instrument.
This instrument, validated for Colombia, is integrated by 46 items divided into six dimensions:(11) accessible (5 items) refers to behaviors of caring that are essential in the support relationship and help administered in timely manner, like “approaching the patient by dedicating time”; explains and facilitates (5 items) are the behaviors related with caring to explain aspects that are unknown or difficult to understand, in this case for the parents, related with the disease, treatment, or recovery of their children; comforts (9 items) has to do with the care offered for the patient and parents to feel comfortable, infusing encouragement and vigor; anticipates (10 items) evaluates care planned beforehand, bearing in mind the needs of the user to prevent complications; maintains a relationship of trust (9 items) involves care that generates empathy, including closeness and physical presence; and, lastly, monitors and follows through (8 items) refers to care that implies knowledge of each patient and domain of the technical scientific and procedural. To apply the scale, in all cases, the original question was made aimed at the parents’ perception of the care their children were receiving.
The statistical analysis was conducted with the SPSS software v. 23; absolute and relative frequencies were calculated for each of the items of the scale and central tendency and dispersion measurements were made for the total and the dimensions. To calculate the total scale score, the scores of the items were added and this was divided by the sum of the maximum score, this result was multiplied by 100. The same procedure was conducted for each dimension. For the total score and by dimensions, of the lost data were replaced by the average evaluation of the items that make up the dimension. It was considered that a higher score indicates better perception of the quality of nursing care provided. Additionally, Cronbach’s alpha of 0.96 for the scale total was calculated as internal consistency indicator, and per dimensions the scores were: accessible α = 0.72, explains and facilitates α = 0.69, comforts α = 0.81, anticipates α = 0.86, maintains a relationship of trust α = 0.82, monitors and follows through α = 0.79.
The following ethical aspects were considered: i) authorization was obtained from the instrument’s author and from the researcher who validated said instrument in Colombia. Likewise, they were consulted on the pertinence of its use in the population of interest in the present study; ii) approval was obtained from the Bioethics Committees from the University institution and from the health care institution; iii) participation in the study was voluntary and each participant signed the informed consent; and, iv) the ethical principles were protected and respected in keeping with Resolution 008430 of October 1993 by the Colombian Ministry of Health, according to which this research was classified as minimum risk.
Results
The study secured the participation of 121 parents of 97 neonates hospitalized in neonatal intensive and intermediate care. Prevailing sociodemographic characteristics: 67.8% were female, the mean age of the men was 28±6.9 years (minimum of 15 and maximum of 53) and the women were 26±6.2 years (minimum of 15 years and maximum of 43). Regarding the educational level, 47.9% of the participants had secondary studies, 28.1% university, and only 0.8% were illiterate. In terms of occupation, 37 mothers (30.6%) were housewives, 5 (4.1%) were students, and the rest (65.3%) held different jobs and were on maternity leave. In terms of the hours spent by the parents within the unit when filling out the instrument, it was found that 43% of the parents had spent over 48 h and the 57% remaining between 12 and 48 h.
As per the characteristics of the neonates, 52.9% were in NICU and 47.1% in INCU. Gestational age upon admission indicated that 66.9% were premature and 33.1% to term. In terms of weight, 56.2% weighed less than 2500 g, with an average weight of 2162 ±848 g (minimum 620 and maximum 4420). Prematurity was the principal admission diagnosis (50.4%), followed by perinatal asphyxia (8.3%) and respiratory distress syndrome (7.4%).
According to the data obtained by applying the CARE-Q instrument (Table 1), the parents perceived as positive the quality of nursing care in the neonatal unit with a global evaluation of 88.9 over 100 possible points, observing that the highest score averages were in the dimensions Monitors and follows through (95.2), Accessibility (90.8), and Maintains a relationship of trust (88.6), with the three other dimensions scoring above 85.
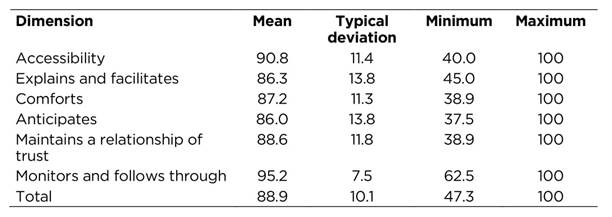
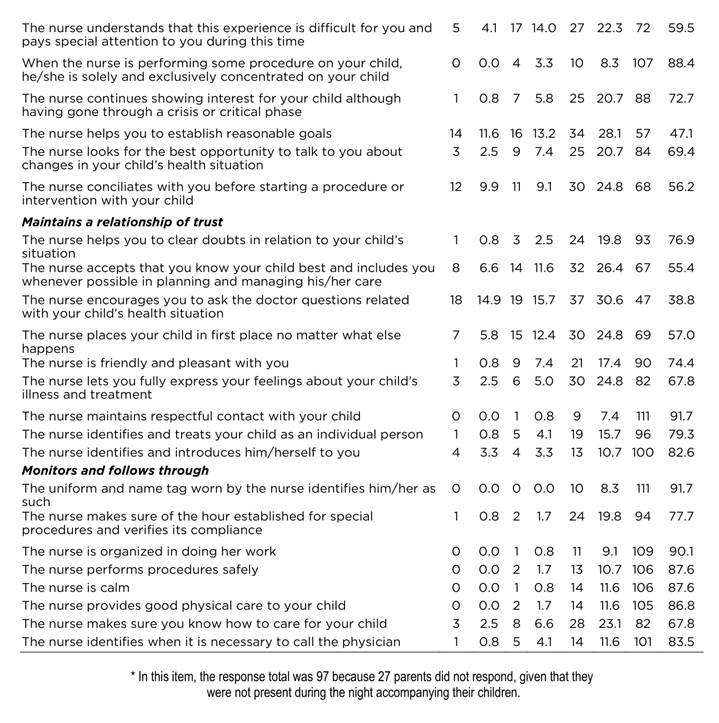
Table 2 shows the frequency of the nurse’s care actions, contemplated in the CARE-Q, according to the dimensions and responses of the parents who participated in the study. In the Accessibility dimension, the responses were predominantly in the categories always and almost always. The item best evaluated by the parents was if the nurse approaches your child to offer measures to relieve pain or to perform procedures (always = 81%). In the Explains and facilitates dimension, the item The nurse is honest with you regarding your child’s medical condition obtained the best evaluation (always = 98.3%), while the lowest items were the nurse suggests questions you could ask the doctor when needed (always = 40.5%) followed by the nurse teaches you how to care for your child (always = 66.1%) and told you about support groups available in the health care institution to learn how to care for your child (always = 66.1%).
In the Comforts dimension, 88.4% states that the nurse is always kind with their child in spite of having difficult situations. It is striking that only 22.3% of the parents expressed that the staff always sits with them to start a conversation. In the Anticipates dimension, the lowest percentages in the always item, were for the item when you feel overwhelmed by your child’s illness, the nurse agrees with you on a new intervention plan (42.1%) and the nurse helps you to establish reasonable goals (47.1%). In the Maintains a relationship of trust dimension, the items with the highest scores were: the nurse maintain respectful contact with your child (always = 91.7%) and the nurse identifies and introduces him/herself to you (always = 81.6%). The lowest evaluation was given to the item the nurse encourages you to ask the doctor questions related with your child’s health situation (always = 38.8%). Lastly, the Monitors and follows through dimension highlights that 90.1% of the parents indicated always in the item the nurse is organized in doing his/her work, while only 67.8% indicate that the nurse makes sure you know how to care for your child.
Discussion
The CARE-Q instrument in this research obtained a general Cronbach’s alpha of 0.955, indicating that its application is highly reliable in the study population.(17) This is an aspect of interest, given that other experiences were not found of the application of this instrument in the context of neonatal care. Studies with other populations in which the same instrument was applied(11-15) obtained Cronbach’s alpha >0.7, but are not comparable with that obtained in this study applied to the parents of the neonates and not directly to the patient object of the care.
Regarding the sociodemographic variables, the study population was predominantly young adult parents, with mean age at 26 years and medium educational and socioeconomic levels. These findings, in general, coincide with those found in populations from other studies conducted in Latin America.(18,19) Furthermore, in terms of the variables of the neonate’s health status, prematurity was the first cause of admission and weight was <2 500 g, findings coherent with the local, national, and international context, where prematurity and low weight are the first causes of admission to the neonatal unit.(19,20) From a general perspective, the quality of nursing care perceived by the parents of the neonates evaluated with the CARE-Q is high. Studies with other populations conducted with this instrument are coherent from the general perception point of view, given that high evaluations were also found in the care actions during hospitalization.(14-16)
In the analysis by dimensions, Explains and facilitates and anticipates obtained high scores, but with broad standard deviations, which suggests a low score in some of its items, being an aspect of interest and analysis. As per the dimension Explains and facilitates, which refers to the information the nursing staff offers the parents about difficult or unknown aspects,(11) other studies carried out in the country, also obtained high evaluations,(15,16) but in this study, differences exist in the analysis of the items. A particular finding has to do with the items with lower evaluation being related with communication processes with the parents and with the health staff. Communication is, among others, a fundamental element to provide education and teach the parents how to care for their children, with this being a continuous task of the nursing staff in the neonatal units throughout the hospitalization process.21 In this regard, Swanson’s(6) theory defines care as an educational way of relating with a loved one towards whom one feels a commitment and personal responsibility. In this sense, we should consider the importance of strengthening educational processes for the parents as an element of the quality of nursing care for neonates.
In addition, the dimension Anticipates was generally well evaluated, a finding contrary to that of another study conducted in the country with the same instrument, where this dimension was perceived with a lower level of quality.(22) Anticipates is a dimension that refers to the nursing staff’s capacity of preventing complications and preempting the satisfaction of the patient’s needs, an aspect Kristen Swanson reaffirms in her theory.(6) When the care subjects are neonates and their families, anticipating is an aspect that gains especial importance, given that the emotional needs of the parents within the neonatal context are common and, in many cases, predictable.(21)
In this dimension, the items having to do with parent participation in establishing reasonable goals and proposals of new care intervention plans obtained low scores. This element proposes the importance of generating actions that favor parent participation to achieve greater empowerment during the care process, (23) which is a very important goal for parents to gain confidence in caring for their children.
The dimension Monitors and follows through received the highest evaluation in this study. This finding is interesting because it asks about the domain of the technical scientific and procedural. Neonatal care demands developing specific practical skills, given the neonate’s vulnerability(24) and the findings herein show a positive panorama on the quality of care perceived by the parents in this sense. In the other dimensions, the analysis according to the items proposes aspects of interest, among which are highlighted that in the dimension of Accessibility, the item best evaluated by the parents has to do with the role of the nursing staff in relieving their children's pain, which indicates that the nurse prioritizes this need in neonates, an aspect of great importance within this care environment.(25)
Similarly, in the Comforts dimension, it is noted that the parents had a low evaluation regarding the possibility of the nursing staff to sit and start a conversation with them, but evaluated positively the nurse always being kind with their child in spite of having difficult situations. This finding makes sense, in that it shows that nurses can implement interpersonal and therapeutic communication; however, establishing a transpersonal relationship9) can be complicated in neonatal units where the burden of excessive work and concern for the development of techniques displaces the recognition of the place occupied by significant human relations.(26) Lastly, in the dimension maintains relations of trust the results indicate that parents perceive that the nursing staff encourage them to ask the physician questions about their child’s health, which indicates that it is necessary to strengthen communication not only in direction of the families,(27,28) but also among the health staff.
In conclusion, from a general point of view, parents have a positive perception of the nursing care their children receive in the neonatal unit. However, in the analysis by dimensions, the need exists to strengthen aspects mainly related to: Explains and facilitates and Anticipates, among which interpersonal relations and communication processes with the families and the health staff are highlighted.
The results guide toward the need to propose actions aimed at establishing settings and communication channels for the parents and health staff to enhance the creation of clearly defined and individualized care plans, involving the family as a subject of care. Likewise, it is important for the communication processes to favor the education provided to the parents for the care of their children and to involve them early on in said care, given that this aspect is determinant in the parents’ trust and capacity of caring. The type of sampling is recognized as a study limitation, which for this study was not probabilistic, given that the dynamics of the unit has low rotation due to the prolonged hospitalizations of patients derived from their high complexity.

