











 English (pdf)
English (pdf)
 Article in xml format
Article in xml format Article references
Article references
 Send this article by e-mail
Send this article by e-mail Cited by SciELO
Cited by SciELO  Cited by Google
Cited by Google  Similars in
SciELO
Similars in
SciELO  Similars in Google
Similars in Google 
 Permalink
PermalinkIntroduction
The use of Physical Restraints (PR) within the psychiatric services is a common practice worldwide. Physical restraints refer to any physical methods of restricting a person's freedom of movement, physical activity or normal access to his or her body.(1) Use of restraints in mental health care setting perceived differently as some people view restraint of psychiatric patients as a violation of basic human rights, others as a necessity to reduce the risk of harm among psychiatric patients whether it is directed toward self or toward others (2) and others as a therapeutic modality. However, throughout history the practice of restraint has been associated with punishment, custodial care, institutional abuse and neglect.(3) On the other hand, using of physical restraints among psychiatric patients raises a range of ethical, legal, and clinical questions.(4,5) Psychiatric management in India often includes the practice of physical restraints to control aggressive patients not only in psychiatric hospitals and also in places of traditional healing.(6) For example, the Erwadi tragedy, which was a fire accident, occurred on August 06, 2001 and 28 psychiatric patients died at Moideen Badhusha Mental Home, because they had been fettered and could not escape. Today, nine years later, and despite the existence of laws against such practices, nothing has changed.(7) Drew et al also reported that mental health policies and laws in low- and middle-income countries failed to incorporate international human rights and best practice standards to prevent violation of human rights. India was not an exception. The new Mental Health Care Bill 2016 focused on a rights-based protection of persons with mental illness and guidelines for using seclusion and restraints.(8)
Earlier studies report that elderly and persons with mental illness have a higher rate of physical restraint use worldwide.(9) Nurses are ethically obligated to ensure the patient’s basic rights and restraints must not be used for coercion, punishment, discipline, or staff convenience.(10) Further, nurses are the health care providers who initiate restraint use and attribute its use to ensuring the safety of the restrained and the others.(11) Their role starts with the selection of appropriate restraint device to ending with modifying the patient care plan based on an hourly assessment of the patient's response and physical condition.(12) The nurses’ positive attitudes towards physical restraints may influence their practice in general.(13) A recent study among psychiatric nurses showed ambivalent attitudes towards use of physical restraints among mental health consumers.(14) Further, it was argued that nurses’ views and attitudes toward the use of physical restraints may create conflicts with patients’ rights, including their autonomy in making decisions for their own care.(15) In a recent cross sectional surveys from India and Australia, most psychiatrists opined that coercion violates the patients' integrity and may harm therapeutic relationships.(16) Since nurses' knowledge and attitude towards physical restraints is closely related to their practice, it is critical to assess nurses’ knowledge, attitude and practice towards use of physical restraints to develop standardized guidelines in mental health care settings. Further, there were no formal studies on this issue from India. Hence, the present study was aimed to assess knowledge, attitude and practice towards use of physical restraints among nurses those working in psychiatric health care settings.
Methods
The present study was carried out among nurses working at a tertiary care center in South India in the month of November 2015. Descriptive design was adopted for the present study. The study sample was selected through convenient sampling technique. The inclusion criteria for this study as follows; a) both gender, b) nurses those were working in different psychiatric units with minimum one year of experience. A total of 140 nurses were eligible to participate in the study. However, six of the participants were absent during data collection, four of them refused to participate and two of the incomplete questionnaires were discarded. Hence, the final sample consisted of 128 nurses with 86% response rate.
Data were collected through self administered questionnaire which comprised of 4 parts: 1- Socio demographic profile : included background information of the participants such as age, gender, experience and education; 2- Knowledge questionnaire about the use of physical restraints: used to assess nurses knowledge, towards using the Physical Restraints in psychiatric patients(17) and consisted of 11 items with closed ended responses such as ‘true’ or false. The correct responses were given a score of ‘1’and incorrect responses a score of ‘0’. Thus a score of 11 represented 100% correct responses; 3- Attitudes toward the use of physical restraints: This was a four point Likert scale with 12 items (4 negatively worded items) used to assess nurses’ attitudes towards use of physical restraints.(17) The responses were scored with a four for "strongly agree", to a one for "strongly disagree". Thus high scores reflected positive attitudes and low scores reflected negative attitudes. Items 4, 9, 10 and 12 were negative and their scores were reversed. Thus, high scores with cutoff point >24 reflected positive attitudes and low scores with cutoff ≤24 reflected negative attitudes (potential range: 12-48); 4- Nurses’ practice towards use of physical restraints: This part addresses nurses’ practice about use of physical restraints in mental health care settings. The participants were asked to respond to a three-point Likert scale ranged from ‘always’ (3) to never (1). Item no 10 was a negative item and the responses need to be reversed. Thus a score of 14 indicates the most undesirable practice and a score of 42 the best practice in terms of restraint use. The reliability coefficients for the knowledge, attitudes and practice scales were 0.65, 0.61 and 0.94 respectively.(17)
The questionnaire was piloted among 15 of participants and found that the study was feasible. Hence no necessary modifications were made. The lead researcher approached the nurses various departments of psychiatry units and the objective and procedure of the study were explained to potential participants. After obtaining permission from the administrators of the hospital, researchers met the participants individually at their workplaces and explained the purpose of the research data that would be collected from the nurses who were willing to participate in the study. Participants were reminded that they could withdraw from the study at any time and confidentiality of the data was assured. After obtaining written informed consent, the self-reported questionnaires were distributed to participants. For the Statistical analysis, negatively worded items were reverse coded and the data were analyzed using ‘R’ statistical software. The results were presented in narratives and tables. The t-test was used to determine whether significant differences existed between the participants regarding mean knowledge, attitude and practice scores. Statistical significance was assumed at p<0.05.
Results
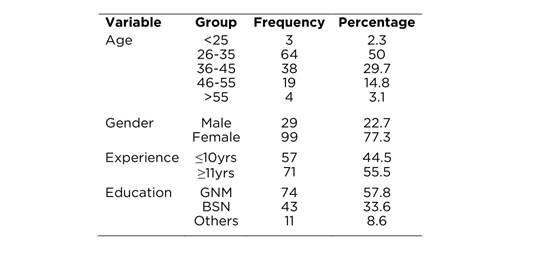
This study represents 79% of the nurses working at a Psychiatric hospital in South India. Among 128 respondents, a majority were females (77.3%). The mean age of the nurses was 36.9±8.66 (range 24-59 yrs, M±SD) and 50% of them were below 35 years of age. More number of them were experienced more than 11yrs (55.5%) and Diploma (GNM) holders(57.8%).
With regard to participants responses to knowledge about use of restraints, a majority of them agreed that ‘physical restraints are safety garments designed to prevent injury’ (78.1%), ‘restraints should be released every 2 hours’ (79.7%), and ‘when patient is restrained skin breakdown may increase’ (79.7%). While 39.1% agreed, a majority (60.9%) disapproved to the item ‘restraints should be used when one cannot watch the patient closely’. Most of the participants answered correctly to the items related to the rights of the patients i.e. ‘patients are allowed to refuse to be placed in a restraint’ (61.7%) and ‘physical restraints require a consent form from the family member’ (74.2%). However, the mean score on knowledge scale was above average of 7.2±1.7 (maximum possible= 11), that indicates good knowledge about use of restraints among the participants (Table 2).
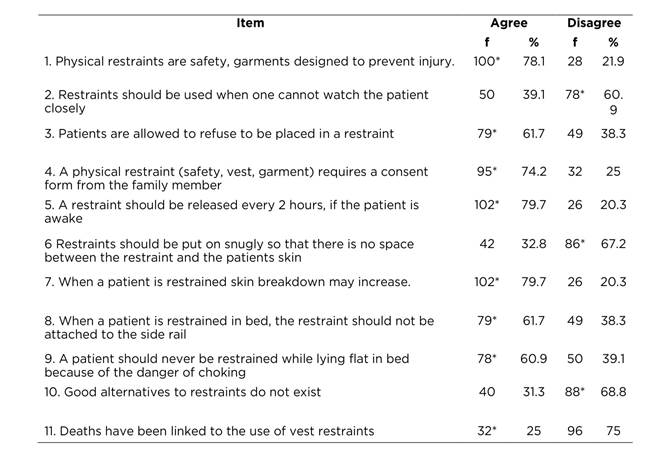
Table 3 depicts the participants’ attitudes towards use of physical restraints among psychiatric patients. A majority of the participants hold positive attitudes towards rights of the participants as they agreed with 1 and 2 items i.e. ‘I feel that family members have the right to refuse the use of restraints’ (78.9%) and ‘If I were the patient, I feel I should have the right to refuse or resist when restraints are placed on me’ (75.8%). Unfortunately, nearly half of the participants (n=61, 47.6%) disapproved that ‘patient suffers a loss of dignity when placed in restraints’. While 40.6% of the participants felt guilty, majority of them disagreed for placing a patient in restraints. Similarly, nearly three fourth of the participants did not feel embarrassed when the family enters the room of a patient who is restrained. However, more than 56% of the participants felt bad if the patients got upset or become more disoriented after the restraints have been applied. It was disappointing to note that 45.3% of the participants opined that ‘applying restraints assures legal protection to his/her self and his/her hospital’. The mean score on this section was 30.8± 3.3 (ranged from 24 to 45) of a maximum possible of 48 and suggest favorable attitudes among the participants towards use of physical restraints among persons with mental illness.
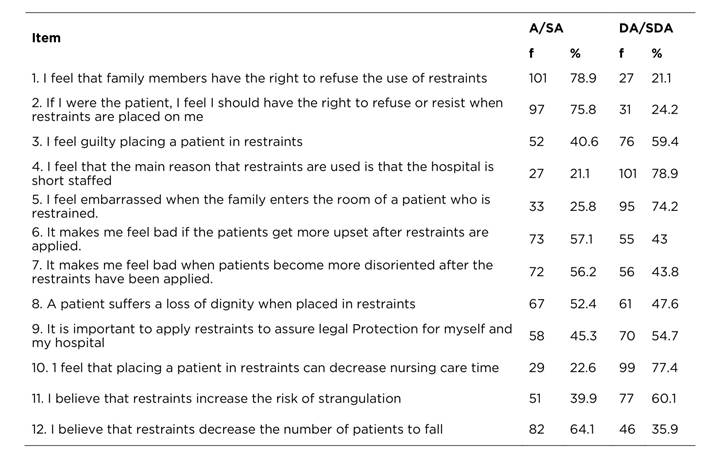
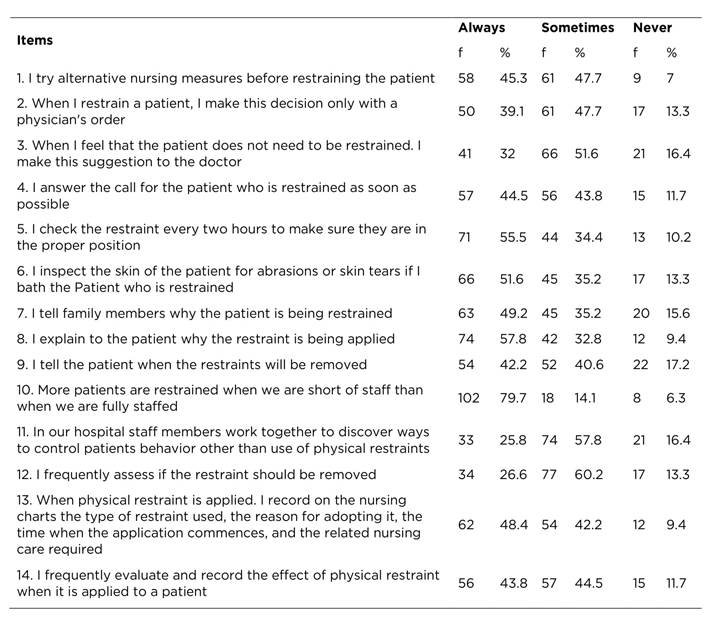
Table 4 addresses the nurses practices with regard to use of physical restraints in psychiatric patients. A majority (93%) of the nurses agreed that they always/sometimes try alternative nursing measures before restraining the patient. More number of the participants stated that they sometimes than always restraints the patients only with physicians’ order and they suggest the doctor when they feel that patient doesn’t need to be restrained. Majority of the participants expressed that they check the restraint every two hours to make sure they are in position and inspect the skin of the patient for abrasions or skin tears. Unfortunately, 79.7% opined that more patients are restrained when there is short of staff. Similarly, more number of the nurses felt sometimes than always work together to discover ways to control patients’ behavior than use of restraints and assesses if the restraint to be removed. The mean score of nurses’ practice related to use of restraints in psychiatric patients was 31.2±6.2 (range 15-42) of maximum possible of 42. These findings indicate good practice related to use of physical restraints among nurses.
On correlation analysis, it was revealed statistically significant association between gender with knowledge (r=0.30, p<0.001) and attitude (r=0.21, p<0.05) of the participants. Females had better knowledge, attitudes than males towards use of physical restraints. However there was no significant difference between gender and practice of the nurses with related use of physical restraints. Nurses those had more than ten years of experience found to be favorable attitudes than nurses with less experience (r=0.17, p<0.05). On one way analysis, nurses with higher education differed significantly on practice score than nurses with basic education in nursing (p<0.05). A significant correlation was found between nurses' total scores of knowledge (p<0.01), attitude (p<0.001) with their practice of using physical restraints.
Discussion
This was a first cross sectional survey that assessed nurses’ knowledge, attitude and practice towards physical restraints in psychiatric patients. The findings reveled that nurses had better knowledge and favorable attitudes as reflected in good practice of using physical restraints in psychiatric patients. There were significant association between gender with knowledge and attitude of the participants towards use of the physical restraints. However, a positive significant correlation was found between knowledge, attitude and practice scores of the participants.
In the present study, majority (79%) of the nurses agreed that skin breakdown may increase when patients are restrained. These findings were in line with earlier studies that found ‘dehydration, choking, circulatory and skin problems, loss of muscle strength and mobility, pressure sores, incontinence and injury from associated physical/mechanical restraint, injury from other patients, increased psychological distress and, in rare circumstances, death were the adverse events associated with use of physical restraints among patients.(18) Although, nurses in the current study, endorsed good knowledge and positive attitudes towards rights of patients, nearly one quarter of nurses disagreed that ‘family members have the right to refuse the use of Physical restraints’. These findings were in consistent with earlier studies conducted among Psychiatric nurses(14) and ICU nurses.(19) These findings suggest need to improve nurses’ knowledge on patients’ rights and ethical issues related to use of physical restraints.(14)
In supporting the previous studies,(19) nearly half the participants in this study disapproved with the statement “A patient suffers a loss of dignity when placed in restraints”. It is unfortunate to note the nurses’ unawareness about the feelings of the psychiatric patients when they were restrained and this negative attitude also increases the use of physical restraints. Published evidence report that patients as a result of being restrained reported that they felt angry, helpless, sad, and powerless, punished, embarrassed, and that their right to autonomy and privacy has been violated, in addition to a feeling of loss of self worth, degradation, demoralization and humiliation while they are restrained.(20) Further, recent studies in India report that most of the psychiatrists’ had negative attitudes towards coercion among psychiatric patients as it violates the integrity of the patients.(21) Earlier research report array of emotional reactions among nurses while restraining the patients such as anxiety, anger, feeling bored or distressed, crying, inadequacy, hopelessness, frustration, fear, guilt, dissatisfaction, isolation, being overwhelmed, feeling drained, vengeance and repugnance.(22) In line with these findings, the present study also showed guilty and disagreement among the participants to place patients on restraints.
In the current study, nearly three fourths of the participants did not feel embarrassed when the family enters the room of a patient who is restrained and support the earlier evidence.(19) Further nearly 43% of the participants did not feel bad if the patients got upset or become more disoriented after the restraints have been applied. Earlier studies also indicate no emotional reaction among nurses.(22) These findings could be attributed to the fact the practice of physical restraints had become so ritualized that it does not provoke any reaction among nurses.(23)
A vast majority of the nurses in this study agreed that they would try alternative nursing measures before restraining the patients. These results were in concordance with previous research among nurses that found several alternative methods that could be used before applying Physical Restraints such as providing companionship and supervision, offering physical and diversional activities, playing soft music, manipulating environments.(14) Interestingly, merely 9.4% of the nurses in this study agreed that they never record on the nursing charts about the type and the reason for applying restraints. These findings were inconsistent with earlier studies that indicate less than half of the nurses do not record data about PR use in patient's chart.(14) However, majority (79.7%) of the nurses felt that more patients are restrained when they are short of staff. These findings were inconsistent with other studies(19) and suggest the need for creating awareness among nurses regarding the reasons for applying the restraints.
The result of the current study is consistent with earlier studies (19) found that more than 50% of the patients were restrained physically and removed without written medical orders. However, this number is lesser than the present study where 39% of the nurses restrain the patients with doctors’ order. In line with previous findings,(14) in the present study nurses those had more than ten years of experience found to be favorable attitudes than nurses with less experience. These findings suggest that better experience improves nurses’ decision making about proper use of physical restraints. In the current study, female nurses with higher education had better knowledge and positive attitudes towards use of physical restraints and these findings were in support of the earlier evidence.(24) In addition, nurses’ knowledge, attitude and practice scores towards use of physical restraints were positively correlated. These findings were in agreement with other studies.(19)
The present study has certain limitations such as cross sectional survey, small and convenient sampling and the data was collected from a single setting. Hence, it is difficult to generalise the findings. However, the study contributes to the literature by assessing nurses’ knowledge, attitudes and practices towards use of physical restraints in mental health care settings which is a common practice in India. The findings may be helpful to nursing administrators to develop standardized protocols about using of physical restraints among psychiatric patients.
Conclusion
This study revealed good knowledge, positive attitudes and good practices among nurses about using physical restraints in mental health services. Further, in line with earlier findings,(6) out study also showed that nurses with higher education had good practice related to use of physical restraints. These findings indicate the need for continuing education about use of physical restraints among nurses may help to protect human rights of patients with mental illness.

