











 texto em
texto em  Inglês (pdf)
Inglês (pdf)
 Artigo em XML
Artigo em XML Referências do artigo
Referências do artigo
 Enviar este artigo por email
Enviar este artigo por email Citado por SciELO
Citado por SciELO  Citado por Google
Citado por Google  Similares em
SciELO
Similares em
SciELO  Similares em Google
Similares em Google 
 Permalink
PermalinkIntroduction
The process of aging of the population favors the manifestation of chronic diseases, which may be associated to the gradual decrease of regulatory functions of the organism and cause a greater vulnerability to certain pathological factors.1 Among chronic diseases, chronic kidney disease (CKD) stands out as a pathology with high morbidity and mortality and progressive incidence in Brazil and worldwide.2 It is defined by the presence of a renal parenchymal lesion associated or not with reduced Glomerular Filtration Rate (GFR) for at least three consecutive months or, still, by the presence of GFR of less than 60 mL/minute/1.73 m2 for 3 months or more.3 Due to the progressive nature of the disease, CKD has been seen as a public health problem. In 2016, the Brazilian Society of Nephrology estimated that approximately 113 thousand patients were undergoing some kind of therapy for the control of CKD in Brazil, corresponding to an increase of 6.3% over the number of patients treated in the year 2011.4
The therapeutic modality chosen depends on the stage of the disease. Thus, CKD patients may receive conservative treatment with drug and dietary therapeutic measures, or renal replacement therapy (RRT), which is necessary when the disease progresses. The types of RRT currently available are: dialysis, represented by hemodialysis and peritoneal dialysis, and renal transplantation.5 Among renal replacement therapies, hemodialysis is the most commonly used by CKD patients. This modality requires adaptations in the patient's life due to the restrictions imposed by the treatment, with a direct impact on quality of life.6 These adaptations include, for example, the time reserved for treatment sessions and medical consultations. Physical, social, emotional and psychological changes are also caused by the pathology, which may have an impact leading to isolation and lack of energy to deal with daily assignments.1
In order to assist in the care of these patients, the Nursing Process must be deliberately and systematically implemented. To do so, five interrelated, interdependent and recurrent steps must be covered: Assessment, Diagnosis, Planning, Implementation and Evaluation.7 The Nursing Outcomes Classification (NOC) includes outcomes and indicators to be identified and evaluated during the planning of the nursing process. The use of this classification represents a device for the clinical practice of nursing. Among the nursing outcomes listed in the NOC, in the case of CKD patients, it is important to evaluate the "1803 - Knowledge: disease process, defined as the extent of understanding transmitted about the specific process of a disease and the prevention of its complications".8 Thus, it is considered essential to know the public of renal patients undergoing hemodialysis and their specificities in order to establish possible associations with the nursing outcome to be studied and contribute to a more effective planning of the guidelines provided. Therefore, the present article aims to verify the relationship between sociodemographic data and the nursing outcome Knowledge: disease process in patients undergoing hemodialysis.
Methods
This is a cross-sectional descriptive study with a quantitative nature developed in a hemodialysis unit of a public hospital, reference in nephrology, in the State of Pernambuco/Brazil between August and December 2016. The study population consisted of 74 patients, who represented the total number of individuals undergoing hemodialysis in the unit. For selection of the sample, eligibility criteria applied. The inclusion criteria were: to be older than 18 years and to present a medical diagnosis of CKD. Exclusion criteria were: to present difficulty in verbal communication or disorientation as to time, space or psychic state, and have the medical diagnosis of Acute Renal Failure. Thus, 23 patients did not participate in the study because of the presence of some exclusion criteria and/or because they did not meet the inclusion criteria. This left a sample of 51 patients. Data collection occurred by means of an interview with the patients during hemodialysis sessions and after reading and signing the Informed Consent Term. A form was used in the interview and was applied by two resident nurses of nephrology and two nursing undergraduate students from the Federal University of Pernambuco, who had been previously trained. The form used was composed of two parts: 1) questions on sociodemographic and clinical data, and 2) questions related to the indicators of the result of the NOC 1803 - Knowledge: disease process.
The demographic data collected in this study were: age (in years), sex (female or male), marital status (with or without companion), origin (metropolitan region of Recife, coutryside of the state of Pernambuco, or others), a practitioner of a religion (yes or no), years of schooling, family income (number of minimum wages; one minimum wage = R$ 880, which was equal to $ 3520 in 2016), occupation (unemployed, retired/receiving benefit, or others). As to clinical data, the time of diagnosis of CKD (in months), time undergoing hemodialysis (in months) and the dialysis site (Arteriovenous Fistula-AVF, Double Lumen Catheter - DLC/Triple Lumen Catheter - TLC, Permcath and Prosthesis). The indicators used from the result of the NOC 1803 - Knowledge: disease process for specification of CKD were 15, namely: Specific process of the disease; Cause and contributing factors; Risk factors; Effects of the disease; Signs and symptoms of the disease; Usual course of the disease process; Strategies to minimize the progression of the disease; Potential complications of the disease; Signs and symptoms of complications of the disease; Precautions to prevent complications of the disease; Psychosocial effect of the disease on the individual; Psychosocial effect of the disease in the family; Benefits of disease control; Available support groups; and Respectable sources of specific information on the disease. (9
The grades used for the indicators presented the following classification: 1 = no knowledge; 2 = limited knowledge; 3 = moderate knowledge; 4 = substantial knowledge; and, 5 = broad knowledge. It noteworthy that, in order to elucidate the indicators and grades, operational definitions were identified from research carried out through a narrative review of the literature in textbooks and databases. Thus, grades were defined according to the number of correct responses indicated by the patient, except for the indicators Available support groups, Respectable sources of specific information on the disease, and Usual course of the disease process. In these indicators, there were four options of answers, and the absence of response or the choice of each of them by the patient related to a degree of knowledge. The results from the survey were entered into the Statistical Package for the Social Sciences (SPSS) version 20.0 to create a database. This enabled the analysis of these data with the development of descriptive statistics by means of absolute frequency, percentage, mean, median, standard deviation and percentiles of each variable. The Kolmogorov-Smirnov test was performed to evaluate the distribution of quantitative data as to normality. The Spearman correlation test, Mann-Whitney and Kruskal-Wallis test were used to verify the associations between variables. As for the classification of the strength of the correlation between the variables tested through the Spearman coefficient, the values adopted were: 0.00-0.19 (absent or very weak), 0.20-0.39 (weak), 0.40-0.59 (moderate), 0.60-0.79 (strong), and 0.80-1.00 (very strong).10 For the statistical significance of the cited tests, a level of 0.05 was adopted. The study was only initiated after approval by the Research Ethics Committee of the Federal University of Pernambuco (Opinion nº 1.451.524 and CAAE 53172216.9.0000.5208), respecting all the precepts of Resolution nº 466/2012 of the National Health Council of the Ministry of Health, which rules research involving human beings.
Results
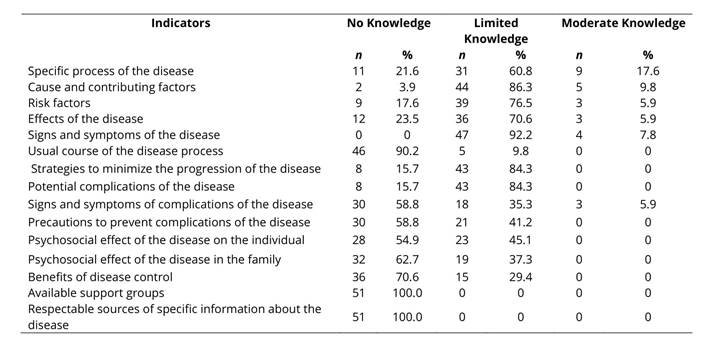
In this study, the mean age of CKD patients was 50.1±15.2 years (minimum = 20, maximum = 89), 62.7% were male (62.7%), from the Metropolitan Region of Recife (100%), 70.6% lived with a partner, had 9 ± 3.3 years of schooling, and family income of 1.7±1.1 minimum wages. Regarding religious belief, 84.3% practiced some religion. As for occupation, 60.8% were Retired/Receiving benefited (60.8%), 9.8% were unemployed and 29.4% had other non-listed occupation. About the clinical variables, the time of diagnosis of CKD was 31.1±16.5 months and the time undergoing the treatment was 29.5 ± 5.8 months. The prevalent dialysis site was AVF (88.2%), followed by Permcath (long term) and arteriovenous prosthesis, with 5.9% each. Regarding the indicators of the nursing outcome of the NOC 1803 - Knowledge: disease process, they are described in detail in table 1. It was observed that in none of the outcome indicators did the participants have knowledge classified as substantial or broad and that the category "no knowledge " prevailed in 8 out of the 15 indicators (in two, there was 100%: Support groups available and Respectable sources of specific information on the disease).
Table 1 Characterization of CKD patients undergoing hemodialysis in terms of knowledge about outcome indicators NOC 1803 - Knowledge: disease process. Recife - PE, 2016
Regarding the association between sociodemographic data and indicators of the outcome of the NOC Knowledge: disease process, a statistically significant but weak correlation was found between the following data: age versus the indicators Specific process of the disease (rs=-0.282, p=0.045), Cause and contributing factors (rs=-0.356, p=0.010), Signs and symptoms of the disease (p=0.032; rs=-0.300), Signs and symptoms of complications of the disease (rs=-0.370, p=0.007), Precautions to prevent complications of the disease (rs=-0.352, p = 0.011); number of years of schooling and the indicators Specific process of the disease (rs=0.286, p=0.042), Cause and contributing factors (rs=0.287, p=0.041), and Signs and symptoms of the disease (rs=0.342, p=0.014). A statistically significant correlation of moderate intensity was identified between the data: age and the Psychosocial effect of the disease on the individual (rs= -0.411, p=0.003), the Psychosocial effect of the disease in the family (rs=-0.436, p=0.001) and Benefits of disease control (p<0.001; rs=-0.489). And through the Mann-Whitney U test, it was observed an association between the sex variable and the indicator Specific process of the disease (p=0.029). No statistically significant associations were observed between any clinical variable and indicators of the outcome NOC Knowledge: disease process among the analyzed patients.
Discussion
The discussion was based on the data to which significant statistical association was found. The sample was found to be predominantly adult, male and with complete primary education. These variables (age, sex and schooling) had a statistically significant association with eight of the indicators on the knowledge about chronic kidney disease. Age presented a statistical association with the indicators Specific process of the disease, referring to the definition of CKD, and Causes and contributing factors, referring to the main causes that lead to CKD. This was also pointed out in a survey conducted in an outpatient clinic of Nephrology in Goiás, in which CKD patients showed ignorance about important information concerning the disease, such as its incurable character, which was the case of 20% of the sample, and the main causes of kidney disease.11 Similarly, another study pointed to a low rate of CKD patients who identified diabetes and hypertension as possible causes of renal impairment.12
Age was also significantly related with the indicator Signs and symptoms of the disease, referring to the possible signs and symptoms of CKD. A survey that surveyed the knowledge of self-management among CKD patients showed a significant deficit in the recognition of the symptoms of the disease in advanced stages and revealed ignorance about the asymptomatic form of the pathology. This fact can lead to detrimental outcomes, as a long-term search for health care.13 Likewise, statistical significance was observed between age and the indicators Signs and symptoms of complications of the disease, and Precautions to prevent complications of the disease, referring to signs and symptoms of complications and ways to prevent complications, respectively. A study carried out in a clinic for chronic kidney patients aimed to determine the knowledge perceived by patients in dialysis therapy and revealed that patients younger than 50 years presented better scores in relation to knowledge about kidney disease.14 Another study also pointed out that older patients were little aware of CKD.15
This reinforces the importance of knowledge about signs and symptoms of complications of CKD and about the precautions to prevent them. Research indicated that the most prevalent self-reported complications in elderly CKD patients were hypertension (77.1%), cramps (57.1%), anemia (54.3%), weight loss (54.3%) and pain (51.4%), and these were correlated with the frailty scores presented.16 The variable age presented, still, moderate correlation with the Psychosocial effect of the disease on the individual and Psychosocial effect of the disease in the family. Regarding this effect in renal patients, it was found that older individuals require more help and support than the younger ones.17 It is known that social support is indispensable in the management of kidney disease and should be directed to both patients and caregivers. Despite this, low mean scores were identified of these types of support among caregivers compared to those reached by the patients.18 Such facts reinforce the importance of interventions for educational, social and psychological support in order to promote the capacity to deal with the adversities generated by the disease.
In this study, age also showed correlation with the indicator Benefits of the control of CKD. A survey of individuals undergoing hemodialysis in a renal replacement therapy unit in São Paulo reported statistically significant correlations between self-care capability and quality of life of CKD patients.19 Quality of life, in this case, can be considered a benefit of self-care actions that help in the control of kidney disease. Another study that analyzed the factors related to self-care of CKD patients showed a positive correlation between age and self-care. Similarly, a positive correlation between self-care and knowledge of the patient was identified. (20 Thus, when kidney patients have accurate information about self-care, this can influence them to develop such care. As to the variable sex, there was no statistically significant correlation with the indicator specific processof the disease. Contrary to the results of this study, a survey of patients in outpatient clinics of Jordan found no statistically significant results when comparing the level of knowledge between men and women. However, there was significance when the gender was associated with attitudes and practices towards prevention and early detection of chronic kidney disease.21 In turn, the variable schooling had a weak correlation with the indicators Specific process of the disease, Cause and contributing factors, and Signs and symptoms of the disease. A study that evaluated the influence of educational training on health evidenced that the level of schooling was associated with learning and led to differences in health outcomes among CKD patients.22 On the indicator Signs and symptoms of chronic kidney disease, a study reinforced its correlation with the variable schooling. It was observed that subjects with incomplete elementary education presented a 4.7-fold higher risk of loss than respondents with more education in relation to the domain "signs and symptoms" of the scale used to measure quality of life in the study.23
In view of the findings presented, it is recognized that knowledge about CKD can be an important factor in the search for better adherence and coping with the pathology by the patient. Educational interventions addressing general questions about the disease and ways to deal with the changes can be implemented to improve the outcomes among kidney patients. However, it is important to remember the various stages and representations of disease, which require different knowledge and coping strategies.12 Finally, no relationship between the clinical data and the nursing outcome indicators NOC 1803 - Knowledge: disease process was observed. It was also recognized the need for developing nursing interventions in the field of health education, highlighting the involvement of patients and their families in the learning process with a focus on approaching the knowledge of the disease, particularly directed to the profile of the individuals.

