











 English (pdf)
English (pdf)
 Article in xml format
Article in xml format Article references
Article references
 Send this article by e-mail
Send this article by e-mail Cited by SciELO
Cited by SciELO  Cited by Google
Cited by Google  Similars in
SciELO
Similars in
SciELO  Similars in Google
Similars in Google 
 Permalink
PermalinkSummary of Findings
| Case management compared to usual care for hypertensive adults in primary care | Case management compared to usual care for hypertensive adults in primary care | Case management compared to usual care for hypertensive adults in primary care |
| Bibliography: Effectiveness of nursing case management versus usual care for blood pressure control in adults with hypertension: a systematic review | Bibliography: Effectiveness of nursing case management versus usual care for blood pressure control in adults with hypertension: a systematic review | Bibliography: Effectiveness of nursing case management versus usual care for blood pressure control in adults with hypertension: a systematic review |
| Systolic blood pressure (6 months) | 695 (4 RCTs) | ⨁◯◯◯ VERY LOWa,b,c |
| Diastolic blood pressure (6 months) | 695 (4 RCTs) | ⨁⨁◯◯ LOWa,c |
| Systolic blood pressure (12 months) | 1216 (2 RCTs) | ⨁⨁◯◯ LOWe,d |
| Diastolic blood pressure (12 months) | 1216 (2 RCTs) | ⨁⨁⨁◯ MODERATEe |
Explanations: (a) Risk of bias: downgraded once because one article scored 11/13, one scored 9/13, and two scored below 9 (JBI-SUMARI appraisal score); (b) Inconsistency: downgraded twice because heterogeneity was over 75%; (c) Inaccuracy: downgraded once due to sample size; (d) Inconsistency: downgraded once due to heterogeneity between 50 and 75%; and (e) Risk of bias: downgraded once because one article scored 11/13 and another article scored 7/13 (JBI-SUMARI appraisal score).
Introduction
Hypertension is one of the main risk factors for cardiovascular diseases (CVD). In recent years, progress has been made in its treatment, but the number of hospitalizations with important socioeconomic costs remains high.1) Worldwide, hypertension affects 22% of people over 18 years of age.2 In Brazil, data from the Surveillance of Risk and Protection Factors for Chronic Diseases by Telephone Survey (Vigitel) in 2018 pointed out that the prevalence of adults who reported having a medical diagnosis of hypertension was 24.7%, with frequency increasing with age in both sexes and in the less educated part of the population.3
Hypertension represents a public health problem due to its numerical magnitude and potential to cause damage to the population. In view of this context, research about hypertension aimed at enhancing prevention and control actions arising from the health policies of local governments is sorely needed. This health condition is considered a silent threat because it does not commonly present signs and symptoms that alert to the severity of complications.1 Thus, its prevention, diagnosis and control is an attribution of Primary Health Care, which may use measures that do not require a high investment, such as case management (CM), in order to keep the disease under control. According to Mendes,4 CM is a collaborative process between the patient and the professional case manager which aims to agree goals and try to achieve them with the sole purpose of preventing or delaying the occurrence of associated complications, increasing the individual autonomy that allows decision making in the health situation. Studies have shown evidence on the effectiveness of CM developed by nurses for reducing risk factors and decreasing blood pressure levels, as well as improving adherence to the therapeutic regimen.5-9
Case management actions also have proved beneficial to increase knowledge about the disease and self-management of treatment.10 They reduce the number of hospitalizations and aggravations that require emergency care, impacting the improvement of quality of life.11 The results of the systematic review12 confirmed that CM is the most frequent intervention in the chronic care model. It has been associated with significant improvements, especially in relation to diabetes and hypertension. Although publications consider the case manager nurse’s role important to control blood pressure levels, no systematic review published in the Cochrane, JBI Database of Systematic Reviews and Implementation Reports or PROSPERO Library, to our knowledge, has examined the effectiveness of nursing CM in the control of hypertension. This gap motivated the development of the present research, whose aim was to verify the effectiveness of nursing CM in primary care compared to usual care, already offered by the health system, in controlling blood pressure in adults with hypertension.
Because it is a chronic disease directly influenced by eating habits, levels of physical activity and adherence to treatment, it was decided to verify whether the literature addressed the influence of CM on these outcomes and blood pressure levels. The review question is: what is the effectiveness of nursing CM versus usual care in primary health care for improving blood pressure in adults over 18 years with hypertension?
Inclusion criteria
Participants. This review considered studies that included adult patients (over 18 years old) diagnosed with hypertension, with or without other concomitant chronic diseases and followed-up by a case manager nurse as part of a multiprofessional team.
Intervention. This review considered studies that evaluated the effectiveness of case management carried out by nurses and a multidisciplinary team in improving blood pressure. Techniques involving follow-up, monitoring, and health interventions using call centers, tele-nursing, home visits and/or nursing consultations were considered as CM. All studies in which the only systematic difference between the groups was the presence or absence of case management were included; thus, studies with more than two arms were excluded.
Comparators. This review considered studies that compared the intervention to usual care already offered by primary health care centers, which involved the assistance of the health team, with actions that were already part of the normal schedule for patients diagnosed with hypertension, without adding extra activities, only the monitoring regular.
Outcomes. This review considered studies that included the following outcome measures: (i) Blood pressure in mmHg;1) (ii) Improvement in body mass index (BMI) measured as weight/height2 (kg/m2);1 (iii) Increased physical activity measured as time spent performing physical activity each day;(iv) Improvements in lipid profile measured by laboratory examination values of total cholesterol, or high-density lipoprotein, or low-density lipoprotein, or triglycerides; (v) Medication compliance assessed through self-report questionnaires, like the one described by Morisky et al.,13 the Brief Medication Questionnaire;14) (vi) Quality of life measured through validated generic or specific questionnaires, such as the hypertension quality of life questionnaire - short form,15 the Short Form-36 Health Survey;16) (vii) Smoking cessation assessed through data collection tools, questionnaires or patient self-reports, and eventually assessed by serum cotinine levels; (viii) Financial implications analyzed through cost differences (case management versus usual care).
Types of studies. This review considered study with experimental designs, including randomized and non-randomized controlled clinical trials published in Portuguese, English or Spanish between the years 1990 and 2018. The time limitation is due to the fact that CM has become a strategy used more frequently since the 1990s, due to the rising costs of complex treatments.17
Methods
This systematic review was conducted in accordance with the Joanna Briggs Institute methodology for systematic reviews of effectiveness evidence.18 This review was conducted in accordance with an a priori protocol19 (PROSPERO CRD42019112762 - Registration number).
Search strategy. Aiming to find both published and unpublished studies. A three-step search strategy was used in this review. First, an initial limited search of Pubmed an Cinahl was undertaken followed by analysis of the text words contained in titles and abstracts and the index terms used to describe the articles. The search strategy, including all identified keywords and index terms, was adapted for each included information source, and a second search was undertaken on July 12, 2018, to august 30, 2018.
PubMed
#1 (“adult”[MeSH Terms]) AND “hypertension”[MeSH Terms]) OR “hipertenso”[Title/Abstract]) OR “adult”[Title])
#2 ((((((((“case management”[MeSH Terms]) OR “case managers”[Title/Abstract]) OR “managed care programs”[MeSH Terms]) OR “patient care planning”[MeSH Terms]) OR “house calls”[MeSH Terms]) OR “office visits”[MeSH Terms]) OR “visitas a pacientes”[Text Word]))
#3 (((“nurses”[MeSH Terms]) OR “nursing”[MeSH Terms]) OR “nurse/case manager”[Title/Abstract]) OR “nurse/case management”[Title/Abstract]
#4 OR/2-3
#5 ((((((((((((((((((((((((“random allocation”[MeSH Terms] OR “randomized clinical trial”[Abstract]) OR “randomized clinical trial”[Title]) OR “randomized controlled trial”[Abstract]) OR “randomized controlled trial”[Title]) OR “randomized”[Abstract]) OR “randomized”[Title]) OR “randomised”[Abstract]) OR “randomised”[Title]) OR “clinical study”[Abstract]) OR “clinical study”[Title]) OR “clinical trial”[Abstract]) OR “clinical trial”[Title]) OR “clinical trials as topic”[MeSH Terms]) OR “randomly”[Abstract]) OR “trial”[Abstract]) OR “trial”[Title]) OR “groups”[Title]) OR “groups”[Abstract]) OR “placebos”[MeSH Terms]) OR “controlled clinical trial”[Abstract]) OR “controlled clinical trial”[Title] OR “randomised”)))))
# 6 AND/1,4-5 (Filters: Humans) (“1990”[Date - Publication])
Information sources. The databases searched included Pubmed, Cinahl, Lilacs, Web of Science, Scopus, Academic Search Premier, Cochrane Library, WHO Trials. Sources of unpublished studies and gray literature searched included the Directory of Open Acess Journal (DOAJ), CAPES System Portal, Open Gray, European Union Clinical Trial, Proquest Dissertations and Theses, DART Europe E-thesis Portal, World Cat and Electronic Thesis Online System (Ethos). The results obtained in each search in the databases were electronically imported to the Mendeley reference manager (Elsevier), and duplicate records were removed before screening. All the identified studies were evaluated according to the eligibility criteria, based on the information presented in the titles and abstracts. Studies were accessed and assessedin full length for compliance with the eligibility criteria when titles and/or abstracts were not clear/did not have sufficient details to support a decision on their inclusion or exclusion.
Study selection. Following the search, all the identified citations were collated and uploaded into the Mendeley reference manager (Elsevier) and duplicates were removed. Titles and abstracts were screened by two independent reviewers for assessment based on the inclusion criteria for the review. Potentially relevant studies were retrieved in full length and their citation details imported into the Joanna Briggs Institute System for the Unified Management, Assessment and Review of Information (JBI-SUMARI) (Joanna Briggs Institute, Adelaide, Australia). Any disagreements that arose between the reviewers were resolved through discussion, or with a third reviewer.
Assessment of methodological quality. Eligible studies were critically appraised by two independent reviewers at the study level (ATM and JPA) for methodological quality in the review using standardized critical appraisal instrument from the Joanna Briggs Institute.20 Any disagreements that arose between the reviewers were resolved through discussion, or with a third reviewer (MFM).
Data extraction. Data were extracted from the studies included in the review by two independent reviewers using the standardized Joanna Briggs Institute data extraction tool.20 The data extracted included specific details about the intervention and time of follow-up, number of participants, comparison group, and results of interest to the review question [systolic (SBP) and diastolic (DBP) blood pressure, BMI, knowledge about hypertension, treatment adherence, abdominal circumference (CA), lipid profile, smoking, consumption of fruits, salt, and alcohol, and physical activity]. Any disagreements that arose between the reviewers were resolved through discussion, or with a third reviewer.
Data synthesis. The results were synthesized using the JBI-SUMARI tool,20 which were expressed as continuous variables (means and standard deviations), when available, and analyzed. After the analysis, wide heterogeneity was identified for the main outcomes (SBP and DBP) and thus the results of similar outcomes were not grouped in statistical meta-analysis. A narrative and tabular format was used to synthesize and present the results of this review.
Assessment of certainty of evidence in the findings. The Grading of Recommendations, Assessment, Development and Evaluation (GRADE) approach for grading the certainty of evidence followed.21 The certainty of evidence can be classified high, moderate, low or very low. High certainty: the true effect lies close to that of the estimate of the effect. Moderate certainty: the true effect is likely to be close to the estimate of the effect, but there is a possibility that it is substantially different. Low certainty: the true effect may be substantially different from the estimate of the effect and, Very low certainty: the true effect is likely to be substantially different from the estimate of effect.21) A Summary of Findings (SoF) was created using GRADEPro GDT (McMaster University, ON, Canada). The SoF presents the following information when appropriate: absolute risks for treatment and control, estimates of relative risk, and a ranking of evidence quality based on the risk of bias, directness, heterogeneity, precision and risk of publication bias of the results of the review. The outcomes reported in the SOF included the PAS and PAD (main outcomes).
Results
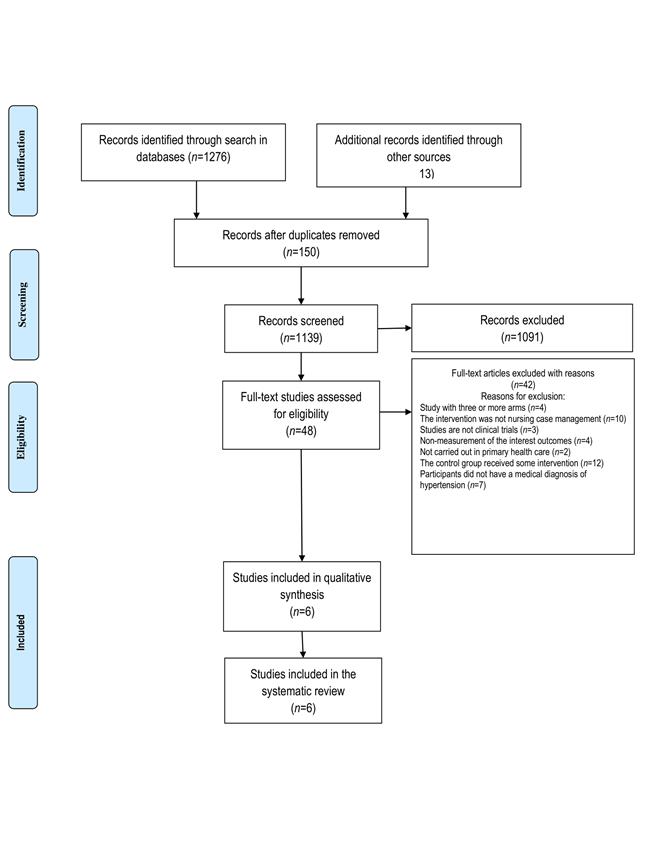
Study inclusion. The initial search for commercially published articles and gray literature resulted in a total of 1289 studies. Forty-eight articles remained after removing duplicates and analyzing the titles and abstracts. They were read in full length, and 42 were excluded for not meeting the eligibility criteria. The six remaining articles were critically analyzed using standardized instruments provided by JBI-SUMARI. The main reason for exclusion of articles in this stage - a total of 13 articles - was the fact that none of the study groups received only usual care (Figure 1).
Methodological quality. The reviewers, in teams of two, independently assessed the methodological quality. Despite methodological limitations, none of the six studies undergoing critical appraisal were excluded from the review, because all obtained scores above 60% for the evaluated items. Table 1 outlines the critical appraisal scores for the studies. The assessment of evidence quality and the strength of recommendation of the results obtained through the GRADEPro GDT are presented for the main outcomes of interest in this review (SBP and DBP) according to time of follow-up (6 and 12 months). In none of the studies the participants or researchers who performed the intervention were blind to treatment assignment, or this information was not even described. As for the evaluators, only two studies23,24) report that they were blinded, avoiding detection bias. In one of the articles25 it was not possible to identify how the allocation of participants was made and in another,7 this item was not respected. This may be related to the nature of the intervention that did not allow the participant or the nurse to be unaware of the division of the groups. The factors that influenced the reduction of evidence quality were mainly the presence of risk of bias, inconsistency related to high heterogeneity, and imprecision due to the reduced sample.
Table 1 Critical appraisal results of eligible studies
| Studies | Q1 | Q2 | Q3 | Q4 | Q5 | Q6 | Q7 | Q8 | Q9 | Q10 | Q11 | Q12 | Q13 | Total |
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Leiva et al. 201423 | Y | Y | Y | N | N | Y | Y | Y | Y | Y | Y | Y | Y | 11/13 |
| Beune et al. 201424 | Y | Y | Y | N | N | Y | Y | Y | Y | Y | Y | Y | Y | 11/13 |
| Cicolini et al. 20146 | Y | Y | Y | U | U | U | Y | Y | Y | U | U | Y | Y | 8/13 |
| Dean et al. 20147 | Y | N | Y | N | N | N | Y | Y | Y | Y | Y | Y | Y | 9/13 |
| Guirardo et al. 201125 | U | U | Y | U | U | U | U | Y | Y | Y | Y | Y | Y | 7/13 |
| Tonstad et al. 200726 | Y | Y | Y | U | N | N | Y | N | N | Y | Y | Y | Y | 8/13 |
| % | 83.3 | 66.6 | 100.0 | 0.0 | 0.0 | 33.3 | 83.3 | 83.3 | 83.3 | 83,3 | 83.3 | 100.0 | 100.0 |
Y = Yes, N = No, U = Unclear. JBI critical appraisal checklist for randomized controlled trials: Q1 = Was true randomization used for assignment of participants to treatment groups?; Q2 = Was allocation to treatment groups concealed?; Q3 = Were treatment groups similar at baseline?; Q4 = Were participants blind to treatment assignment?; Q5 = Were those delivering treatment blind to treatment assignment?; Q6 = Were outcome assessors blind to treatment assignment?; Q7 = Were treatment groups treated identically other than the intervention of interest?; Q8 = Was follow-up complete, and if not, were strategies to address incomplete follow-up utilized?; Q9 = Were participants analyzed in the groups to which they were randomized?; Q10 = Were outcomes measured in the same way for treatment groups?; Q11 = Were outcomes measured in a reliable way?; Q12 = Was appropriate statistical analysis used?; Q13 = Was the trial design appropriate, and any deviations from the standard RCT design (individual randomization, parallel groups) accounted for in the conduct and analysis of the trial?
Characteristics of included studies. All studies were carried out in primary care centers on the European continent, two in Spain,23,25 one24 in the Netherlands, one6 in Italy and one7 in England. However, one of them24 was performed on a specific population of Ghanaians and Surinamese. As for the division by sex, all studies included participants of both sexes in both groups (control and intervention). The average percentage of men in the control groups was 49.7% and in the intervention groups 40.8%. As for age, the participants were aged between 18 and 80 years in two studies,23,25 between 30 and 69 years in one study,26 over 18 years in one study,7 over 20 years in one study24 and there was no age limit in one study.6) The mean age per group, but not per sex, could be identified. The mean age of participants was 59.6 years in the intervention group [min 53.3,24 max 64.523 ] and 60 years in the control group [min 54.6,24 max 66.723 ]. Hypertension was defined in all articles as SBP greater than or equal to 140 mmHg and DBP greater than or equal to 90 mmHg. There was heterogeneity in interventions, frequencies of activities developed, and comparisons. Detailed descriptions of interventions can be seen in Table 2 and a summary of the analyzed outcomes and measurement methods in Table 3.
Table 2 Characteristics of the studies included in the sample
| Study | Synthesis of intervention | Duration and frequency of intervention | Comparison | Outcomes |
|---|---|---|---|---|
| Leiva et al. 201423 | Divided into 5 components: 1 - A motivational interview based on the Health Belief Model; 2 - Reminders to take the medication; 3 - Family support; 4 - Blood pressure measurements and reminders; 5 - simplification of the therapeutic regime. | Duration: 12 months; Follow-up frequency: 1, 3 and 9 months. | Usual care | SBP and DBP BMI Adherence to treatment/lifestyle Cholesterol (total, LDL, HDL) |
| Beune et al. 201424 | Usual care plus three counseling sessions using culturally adapted educational materials and, if necessary, referrals to walking clubs and healthy food stores. | Duration: 6 months; Follow-up frequency: 2 weeks, 8 weeks and 20 weeks. | Usual care | SBP and DBP BMI Adherence to treatment/lifestyle |
| Cicolini et al. 20146 | Usual care, follow-up visits with nurses, and reminders by email and phone calls. | Duration: 6 months; Follow-up frequency: 1, 3 and 6 months. Every day, participants filled out a self-assessment form for treatment adherence and followed an educational program. | Usual care | SBP and DBP BMI Adherence to treatment/lifestyle Cholesterol (total, LDL, HDL) Triglycerides Smoking Alcohol consumption, fruit and vegetable consumption, salt intake, and physical activity |
| Dean et al. 20147 | Medication review, follow-up with motivational interviews where nurses encouraged changes in habits, and phone calls. | Duration: 6 months; Follow-up frequency: monthly. | Usual care | SBP and DBP |
| Guirardo et al. 201125 | Four visits adapted according to the needs of the patients. Guidelines were used and leaflets were provided containing information on prescription drugs, dosage and schedule, as well as basic advice on how to maximize treatment schedules. | Duration: 12 months; Follow-up frequency: 1, 3, 6 and 12 months. | Usual care | SBP and DBP BMI Knowledge about hypertension Adherence to treatment/lifestyle |
| Tonstad et al. 200726 | Monthly meetings with nurses, promotion of changes in lifestyle based on the behavioral self-management model. Individual guidelines were reinforced every month. | Duration: 6 months; Follow-up frequency: monthly. | Usual care with the primary care physician. | SBP and DBP BMI Abdominal circumference Cholesterol (total, LDL, HDL) Triglycerides Glucose |
Table 3 Summary of analyzed outcomes and measurement methods
| Outcome | Study | Evaluation mode |
|---|---|---|
| SBP and DBP | Cicolini et al. 20146; | The device used for measurement is not described. |
| SBP and DBP | Tonstad et al. 200726 | The device used for measurement is not described. |
| SBP and DBP | Leiva et al. 201423; | Atomatic device (Omrom-705 IT/Omrom 705 CP) |
| SBP and DBP | Beune et al. 201424 | Atomatic device (Omrom-705 IT/Omrom 705 CP) |
| SBP and DBP | Dean et al. 20147 | Computerized method |
| SBP and DBP | Guirardo et al. 201125 | Mercury sphygmomanometer (average of two measurements with an interval of 2 minutes). |
| BMI | Beune et al. 201424; | Weight divided by height in meters |
| BMI | Guirardo et al. 201125 | Weight divided by height in meters |
| BMI | Cicolini et al. 20146 | Evaluated through a questionnaire validated during a previous cluster randomized trial |
| BMI | Tonstad et al. 200726 | Not described |
| BMI | Leiva et al. 201423 | Not described |
| Knowledge about hypertension | Guirardo et al. 201125 | Batalla test |
| Adherence to treatment/lifestyle | Guirardo et al. 201125 | Haynes-Sackett and Morisky-Green questionnaires |
| Adherence to treatment/lifestyle | Cicolini et al. 20146; | Morisky-Green questionnaire |
| Adherence to treatment/lifestyle | Beune et al. 201424 | Morisky-Green questionnaire |
| Adherence to treatment/lifestyle | Leiva et al. 201423 | Retrospective evaluation and determination by the ratio between the number of drugs obtained for the period and the number of days evaluated (6 months) |
| Abdominal circumferenc | Tonstad et al. 200726 | Manual |
| Cholesterol (total, LDL, HDL) | Cicolini et al. 20146; | Blood sample (automated equipment) |
| Cholesterol (total, LDL, HDL) | Tonstad et al. 200726 | Blood sample (automated equipment) |
| Cholesterol (total, LDL, HDL) | Leiva et al. 201423 | Form of measurement is not reported, only the parameters used are described. |
| Triglycerides | Cicolini et al. 20146; | Blood sample (automated equipment) |
| Triglycerides | Tonstad et al. 200726 | Blood sample (automated equipment) |
| Glucose | Tonstad et al. 200726 | Automated equipment (Hitachi 911) |
| Smoking | Cicolini et al. 20146 | Evaluation through a questionnaire validated during a previous cluster randomized trial. |
| Alcohol consumption, fruit and vegetable consumption, salt intake, and realization of physical activity | Cicolini et al. 20146 | Evaluated through a questionnaire validated during a previous cluster randomized trial. |
Review findings
The reading of the selected articles revealed a significant reduction in SBP in two studies,6,7 and in DBP in three studies (6,7,24 and such reductions were favorable for the intervention group (Table 4). All studies that showed statistical significance were those with a six-month follow-up. Noteworthy is the study by Guirardo et al.25 which did not present the mean values of SBP and DBP at the end of the study, after a 12-month follow-up, showing only the average difference without a significance test. BMI was another outcome analyzed in two studies, as shown in Table 5.
Table 4 Results of studies analyzing SBP and DBP
| Study/Groups | Sample | Baseline | End | p-value a | Baseline | End | p-value |
|---|---|---|---|---|---|---|---|
| Beune et al. 201424 | SBP | SBP | SBP | SBP | DBP | DBP | DBP |
| Intervention | 71 | 156.7±12.26 | 146.8±16.23 | 0.119a | 91.02±9.61 | 85.3±10.93 | 0.009a |
| Usual care | 68 | 155.2±10.69 | 148.9±13.25 | 0.119a | 89.60±9.36 | 87.9±9.53 | 0.009a |
| Cicolini et al. 20146 | |||||||
| Intervention | 100 | 150±11 | 135±8 | < 0.001b | 87.5±5.7 | 76.4±5.8 | < 0.001b |
| Usual care | 98 | 153±12 | 143±6 | < 0.001b | 88.6±2.3 | 81±3.6 | < 0.001b |
| Dean et al. 20147 | |||||||
| Intervention | 144 | 154.2±17.7 | 142±15.6 | 0.021c | 85.6±11.6 | 79.4±11.1 | 0.004c |
| Usual care | 169 | 152.9±14.0 | 146.1±18.9 | 0.021c | 85.5±1.7 | 82.6±11.8 | 0.004c |
| Tonstad et al. 200726 | |||||||
| Intervention | 29 | 157±9 | 147±9 | >0.05c | 94±6 | 91±8 | >0.05c |
| Usual care | 16 | 153±9 | 143±10 | 71±10 | 92±8 | >0.05c | |
| Leiva et al. 201423 | |||||||
| Intervention | 115 | 156.3±15.1 | 151.3±18.3 | 0.208 c | 84.7±10.7 | 83.4±11.1 | 0.405 c |
| Usual care | 105 | 155.5±13.4 | 153.7±16.8 | 0.208 c | 83.6±10.3 | 83.6±10.3 | 0.405 c |
| Guirardo et al. 201125 | |||||||
| Intervention | 515 | 140.9±22.8 | - | - | 82.5±8.9 | - | - |
| Usual care | 481 | 139.3±17.3 | - | - | 82.2±8.8 | - | - |
Note: (a) Linear regression analysis; (b) t-test for normally distributed continuous variables; Kruskal-Wallis test for non-normally distributed continuous variables; (c) t-test
Table 5 Results of studies analyzing BMI, cholesterol and triglyceride levels
| Study/Groups | Sample | Baseline | End | p-value |
|---|---|---|---|---|
| BMI | ||||
| Cicolini et al. 20146 | ||||
| Intervention | 100 | 29±6.7 | 26.5±5.1 | < 0.001 a |
| Usual care | 98 | 26.5±5.1 | 27.7±4.6 | < 0.001 a |
| Tonstad et al. 200726 | ||||
| Intervention | 29 | 27.7±4 | 27.9±3.9 | >0.05 b |
| Usual care | 16 | 28.6±3.7 | 29±4 | >0.05 b |
| Cholesterol levels | ||||
| Cicolini et al. 20146 | Total cholesterol (mg/dL) | Total cholesterol (mg/dL) | Total cholesterol (mg/dL) | |
| Intervention | 100 | 265±64 | 205±40 | < 0.001 a |
| Usual care | 98 | 251±59 | 218±32 | < 0.001 a |
| Tonstad et al. 200726 | Total cholesterol (mmol/l) | Total cholesterol (mmol/l) | Total cholesterol (mmol/l) | |
| Intervention | 29 | 6.5 | 6.3 | >0.05 b |
| Usual care | 16 | 6.2 | 5.9 | >0.05 b |
| Triglyceride levels | ||||
| Cicolini et al. 20146 | Triglyceride level (mg/dL) | Triglyceride level (mg/dL) | Triglyceride level (mg/dL) | |
| Intervention | 100 | 166±40 | 142±24 | 0.12a |
| Usual care | 98 | 177±34 | 160±37 | 0.12a |
| Tonstad et al. 200726 | Triglyceride level (mmol/l) | Triglyceride level (mmol/l) | Triglyceride level (mmol/l) | |
| Intervention | 29 | 1.97±2.16 | 1.56±1.40 | 0.03b |
| Usual care | 16 | 1.93±1.39) | 2.08±1.30 | 0.03b |
Note: (a) t-test for normally distributed continuous variables; Kruskal-Wallis test for non-normally distributed continuous variables; (b) t-test
In addition to the two studies mentioned above, it was found that three others23-25 measured BMI values, but did not compare the outcome at baseline and end moments through statistical tests. The study by Guirado et al.25 pointed out the average change between the first and the last measurement, without stating whether the value was significant. Regarding treatment adherence, three studies6,24,25 evaluated the outcome using the Morisky-Green questionnaire. One of them6 used only one question of the instrument (Did you take your medication yesterday?) and Guirardo et al.25 also assessed adherence with the Haynes-Sackett questionnaire.
Leiva et al.23) measured adherence by counting medications and not by a specific instrument like the other studies. However, the research did not compare baseline and end values after the intervention. Guirardo et al.25 evaluated adherence to treatment through the percentage of people who were adherent to treatment at the initial visit and then presented the percentages of adherence changes for both questionnaires (Haynes-Sackett and Morisky-Green) and identified an increase in treatment adherence assessed by the Morisky-Green Test of 9.6% (95% CI: 5.5-13.6) in the intervention group and 8.8 (95% CI: 4.9-12.6) in the usual care group. The studies by Beune et al.24 and Cicolini et al.6 demonstrated an increase in adherence to treatment in both groups. Cicolini et al.6 analyzed adherence by domains, namely: complete adherence to the drug, dose and hours of therapy. There was an improvement in the percentage of adherence to treatment for all domains in both groups.
Beune et al.24) presented the results in terms of averages. Higher scores in the questionnaire indicated greater adherence to treatment. Thus, the average score at baseline was 5.99 in the intervention group, reaching 6.49 at the end of the study, whereas, these values were 5.59 and 6.24, respectively, in the usual care group. The total cholesterol was an outcome assessed and compared in two studies.6,26 Both showed a reduction in cholesterol levels after a six-month follow-up, with a significant reduction in Cicolini et al.6) (Table 5).
Cicolini et al. (6 compared LDL-cholesterol levels and identified a significant reduction in the intervention group by the end of the follow-up when compared to the change that occurred in the usual care group (p<0.001). Tonstad et al.26) measured HDL-cholesterol levels and found a reduction, although not significant, in both groups after follow-up.
Leiva et al.23 evaluated total cholesterol only for the the purpose of characterization of the sample at baseline. Two clinical trials6,26 evaluated triglyceride levels as outcome at the beginning and end of the follow-up; one observed a significant reduction in the intervention group26 and the other showed a reduction in both groups.6
The waist circumference was an outcome assessed by Tonstad et al.26 showing no improvements at the end of the follow-up in either of the groups. This study also evaluated the glucose outcome. It was observed that glucose levels after six months of intervention decreased in the intervention group and increased in the control group, but these differences were not significant. The smoking outcome was assessed in the clinical trial by Cicolini et al.6 There were significant improvements only for the intervention group in the first three months of follow-up, and this difference was confirmed at the end of the six months. Leiva et al.23 evaluated smoking only for baseline sample characterization.
In Cicolini et al.6 fruit consumption and physical activity were evaluated. There was a significant increase of fruit consumption in the intervention group, with a consequent decrease in the percentage of people who had low fruit consumption per day. With regard to physical activity, at the end of the CM actions, a significant increase in the time of physical activity performed by the intervention group was detected. Alcohol and salt consumption was also evaluated in the clinical trial of Cicolini et al.6 A significant decrease in the number of alcohol doses per day consumed by the intervention group was observed at the end of the treatment, but no significant differences in salt consumption were seen. The included studies did not analyze the influence of CM on quality of life, nor the financial implications in relation to usual care.
Discussion
The purpose of this review was to synthesize the best available evidence on the effectiveness of nursing CM in primary health care, compared to usual care, in improving hypertension in hypertensive adults over 18 years of age. The main challenge was related to the type of intervention, which was considered complex because different components were involved. The heterogeneity of the interventions and assessment methods limited the comparisons of results and demonstrated that there is a variety of possible readings about what it means to be a case manager nurse among hypertensive patients, and what strategies can be used for this purpose.
All studies included in this review6,7,23-26 applied CM with several activities such as home visits, telephone contact, reminders about the therapeutic regime, motivational interviews, counseling with culturally adapted educational materials, and monthly meetings with nurses. It was found that two studies with duration of six months6,7 showed a significant reduction in SBP and DBP over time for the intervention group, one of which6 applied CM through visits for follow-up by nurses, as well as email and phone reminders. Dean et al.7 carried out follow-up by nurses with motivational interviews to encourage changes in habits, phone calls and medication reviews.
Although two studies showed significant results of the intervention in the SBP and DBP outcomes, Beune et al (24 reported a greater reduction in blood pressure levels and Tonstad et al.26) demonstrated a similar reduction in SBP. In both studies, a greater reduction in DBP was obtained for the intervention group. According to the GRADE approach for assessing the certainty of evidence, a low degree of certainty was found. This fact was mainly due to the risk of bias,6,7,24,26 and serious inaccuracy due to the sample size. (24,26 Despite the absence of significant results in the comparison between reductions in blood pressure levels in both groups, the 12-month study of Leiva et al.23 found higher values for the intervention group. However, another study25 with the same follow-up time found greater reduction in DBP for the intervention group, although SBP was reduced in the control group.
Regarding the quality of the evidence analyzed according to the GRADE approach, it was found that the degree of certainty was low for the SBP outcome due to the risk of bias and inconsistency (heterogeneity above 75%). For the DBP outcome, the degree of certainty was moderate due to the observed risk of bias.
BMI was assessed between the groups in three articles,6,25,26 with only one of them6 showing a significant reduction in this outcome for the group followed-up with CM, while the other studies showed an increase in values. Regarding adherence to treatment, although different instruments were used to measure this outcome,6,24,25 a fact that hinders comparisons, all showed improvement in treatment adherence among people followed-up with CM. Total cholesterol had a significant reduction in the intervention group in the six-month studies.6,26 As for triglyceride levels, only Tonstad et al.26) reported significant improvement for the group followed-up with CM.
Tonstad et al.26 was the only study assessing waist circumference and glucose, without significant improvements for the intervention group. Although only one of the articles evaluated these two outcomes, both are risk factors for hypertension and must be a target of intervention for primary care nurses to reduce complications related to the disease.
Lifestyle changes such as smoking cessation, increased fruit consumption, realization of physical activity, and decreased salt consumption were assessed by Cicolini et al.6 which obtained significant improvements in all outcomes. It is known that lifestyle changes together with the use of the prescribed therapy are key points for the control of hypertension1.
The strong point of this review is the inclusion of literature from a wide variety of databases and gray literature, as well as the inclusion of studies published in several languages. The limitations of this review are the heterogeneity of the data and the quality of the articles which prevented a meta-analysis. Although comprehensive, it is possible that smaller potentially eligible studies have been published in different languages and were not captured by the search strategies employed here.
Conclusions. Efectiveness of nursing CM for adults with hypertension treated in primary care was not consistently detected in this review. However, some clinical trials reported positive results in terms of reduced blood pressure, improved treatment adherence, and improved cholesterol levels. The wide variety of actions used in CM, as well as the different ways of measuring the analyzed outcomes, prevented a statistical comparison of studies.
Recommendations for practice. The findings of this review demonstrated with low and very low certainty that case management performed by six months had a positive impact in reducing DBP and SBP respectively. Although there is no high evidence, it is considered that CMs performed in primary health care can assist in the planning of health actions, health promotion activities, disease prevention, reduction of comorbidities, and control of chronic diseases, as for example control of hypertension.
Recommendations for research. Many studies address the importance of monitoring by nurses to reduce pressoric levels, but the methodologies used in the studies do not provide strong evidence to confirm this statement. More randomized clinical trials with methodological quality and expressive samples need to be performed to confirm or refute the effect of case management for people with hypertension in primary care.

