











 English (pdf)
English (pdf)
 Article in xml format
Article in xml format Article references
Article references
 Send this article by e-mail
Send this article by e-mail Cited by SciELO
Cited by SciELO  Cited by Google
Cited by Google  Similars in
SciELO
Similars in
SciELO  Similars in Google
Similars in Google 
 Permalink
PermalinkIntroduction
Today, chronic diseases are recognized as the most important health problem, especially in developing countries. Asthma is a common chronic inflammatory disease of the respiratory tract characterized by a variety of symptoms, including airway obstruction and bronchitis. Asthma is currently considered as one of the most serious health problems.1,2 In a 2014 report on the global prevalence of asthma states that there are approximately 300 million people with asthma worldwide and that it is expected to increase by about 33% to 20 million until the year 2025.3 Also, the prevalence of asthma and chronic bronchitis in Iran has been reported from 4.8 to 5.6%.4
Quality of life is considered as an important criterion for studying chronic diseases. This means feeling good in physical, mental and social aspects. Accordingly, quality of life is used to assess community health needs, assess the social impact of the disease, identify at-risk individuals, implement appropriate health policies, and allocate health resources. Because asthma is a chronic disease with a high cost of treatment; it is difficult to manage, as a result, it reduces the quality of life of patients and their families.5,6) Despite many recommendations about the role of disease prevention and control through education of correct behaviors, many studies still acknowledge that the disease is slow and difficult to control. This disease is not curable, but with a series of treatment and care measures, it can be controlled to some extent.7,8
Educating patients increases their understanding of the disease, treatment, and can have positive effects on the patient's performance, physical condition, quality of life, adaptation, and reduction of emotional problems.9 One of the most effective methods to improve the understanding of education is the teach-back method. This method is a comprehensive, multidisciplinary, evidence-based strategy used to understand and retain information. Health care organizations have endorsed this approach as an effective way to ensure that health care information is understood and reduce the risk of patients misunderstanding essential information in clinical situations.10,11) In the teach-back method, essential information is explained to the patient in a way that the patient understands and is an educational method to ensure patients' understanding. The purpose of the feedback method is to provide effective learning at the patient literacy level. The advantages of using this method are improving the patient's relationship with the treatment staff, increasing patient safety, better evaluation of the educator from the patient, and usability in people with low literacy levels.12,13) Therefore, the aim of this study was to investigate the effect of teach-back education on patient asthma control and family care pressure of patients with asthma referred to clinics affiliated to Shiraz University of Medical Sciences, Shiraz, Iran. Accordingly, if the intervention performed in this study is effective, its results can be used as an effective way to increase the quality of life and improve asthma control of patients and reduce the stress of caring for their families.
Methodology
The present study is a clinical trial and the study population was patients referred to Shahid Faghihi and Shahid Motahhari clinics in Shiraz, Iran, who referred to the pulmonary ward in the year 2020. Overall, 58 patients with asthma who had the condition participated in the study.
Patients, inclusion, and exclusion criteria. The number of patiets in each group was 29 patients and 29 primary caregivers. Research units were selected by the available sampling method. Then they were assigned to two groups by random assignment. Additionally, inclusion criteria for patients included: moderate to severe asthma (Based on the doctor's opinion), age range 18 to 60 years, willingness to participate in research and fill out informed consent form, not participating in similar programs during the last 6 months, having the ability to understand based on the researcher's judgment, and the possibility of making telephone calls. On the contrary, exclusion criteria also included; absenteeism in educational classes, impossibility to continue cooperation, having a degree in medical sciences and suffering from other chronic diseases. Inclusion criteria for the patient's primary caregiver include: willingness to participate in research and filling out informed consent form, not participating in similar programs during the last 6 months, having the ability to understand based on the researcher's judgment, not caring for other chronic conditions, possibility Making phone calls and not having a critical or stressful event (such as death of relatives, divorce, illness, or immigration in the last three months). Furthermore, absenteeism in educational classes, the impossibility of continuing cooperation in the study, and having education in the medical sciences group were the exclusion criteria for the main caregiver.
Sample size. Based on the study of York et al.,1 the sample size in this study (n=58) also using NCSS software using the mean difference formula between the two groups considering α=0.05, power 80%, mean and standard deviation of group one (0.62 ± 0.05), the mean and standard deviation of group two (0.66 ± 0.05) was determined by considering a drop of 20% in each group:
Data collection tools. Data collection tools included patient demographic information questionnaire, demographic information questionnaire of the main caregiver, asthma control test, lung function test (Spirometry), and ZARIT care pressure questionnaire.
Asthma control test and lung function test (Spirometry). To evaluate the asthma control of patients, asthma control test and lung function test (Spirometry) were used at intervals before the start of the study, 4 and 8 weeks after the intervention. The asthma control test is based on GINA institute criteria and allows patients older than 12 years to assess their asthma control status over 4 weeks.2 The reliability of asthma control test in various studies has been reported equal to 0.94 and its validity has been confirmed based on the correlations between asthma control test and other tools for measuring asthma recovery status.3 In the asthma control test, a score of 5 indicates the best position and a score of 1 indicates the worst position of asthma control. The recorded scores were added together to obtain the total score. The total score was used to assess asthma control status includes score 25 (asthma has been completely under control for the past 4 weeks), score 20 to 24 (asthma has been under control for the past 4 weeks), and score 19 or less (has not been controlled in the last 4 weeks).
Lung function test is performed by a specialist technician using ZAN Spirometry device (Germany) in accordance with the principles related to this test. In this study, indicators such as Forced Expiratory Volume in first second (FEV1), Forced Vital Capacity (FVC), FEV1 / FVC ratio and Forced Expiratory Flow rate %25 - %75 (FEF25 -75%) were measured.
Assess the quality of life of patients. To assess the quality of life of patients, the 67-item questionnaire of Marx et al. was used at intervals before and 8 weeks after the intervention. This questionnaire measures quality of life in 5 dimensions: respiratory function, physical activity, mood function, social function and general perception of health. The answer to each question was scored on a 5 degree Likert scale. In this questionnaire, increasing the total score indicates an improvement in the quality of life. Each question has a number of qualitative answers including: ever, rarely, sometimes, most and always. The score of each positive question is between 1 and 5. The option "always" has a score of 5 and the option "never" has a score of 1. In the negative questions, the option "always" has a score of 1 and the option "never" has a score of 5. Responses to each scale were reported to be rated between 0-100 on average. The validity of this questionnaire in terms of content validity has been confirmed by Marx et al. and has a Cronbach's alpha of 94%. Also, Cronbach's alpha of the subscales of this questionnaire has been reported in the range of 0.79 to 0.85.4 Additionally, the validity of this questionnaire in Iranian society was assessed by Arab et al. (2012); The content validity index was 0.90 and in order to determine the internal reliability, the test-retest method was used and the correlation coefficient was 0.75.5
Assess the care burden of family caregivers. To assess the caregiver burden of family caregivers, the 22-item form of Zarit care burden questionnaire was used at intervals before and 8 weeks after the intervention. This questionnaire is about personal, social, emotional and economic pressures. Caregivers' responses for each statement were measured on a Likert scale with five options (never to always) that were scored from 0 to 4, respectively. In response to each question, the study units chose one of the cases never (zero score), rarely (score 1), sometimes (score 2), often (score 3) and always (score 4). Accordingly, the sum of the scores obtained varies from 0 to 88.6) Accordingly, the scoring of care burden of family caregivers is as follows; score between 0-20 (low or no care pressure to family caregivers), score 21-40 (moderate care pressure to family caregivers), and score 41-88 shows the severe care pressure to family caregivers.
Training procedure. At first, the subjects were divided into intervention and control groups using random method and using 4 blocks. Before the intervention, patients' demographic information questionnaire, asthma control test and quality of life questionnaire for patients in the intervention and control groups, caregivers' demographic information questionnaire, Zarit care burden questionnaire for the intervention and control groups, and lung function test (Spirometry) were completed for patients and control groups. 4 weeks after the intervention, asthma control test was completed for the patients in the intervention and control groups and lung function test (Spirometry) was performed for them. 8 weeks after the intervention, asthma control test and quality of life questionnaire for patients and control groups were completed and lung function test (Spirometry) was performed for them. The Zarit care burden questionnaire was also completed for the caregivers of the intervention and control groups.
In this study, patients and caregivers of the control group were not trained. In the intervention group, according to the pre-determined training program, the return method training was provided individually to the patient and his primary caregiver in three sessions of approximately 60 minutes at intervals of one day. The training was presented face to face, in simple and understandable language, without using special medical terms, along with PowerPoint and practical techniques. At the end of the training sessions, a training booklet related to that session was presented to patients and caregivers. Before each session, the patient and caregiver's knowledge were asked about the content of each session, and after each training session, the patient and caregiver were asked questions again to assess the individual's learning. Accordingly, the correct answer to these questions at the end of each session was the basis for completing the training. The score of the return training was determined in such a way that if the patient answered 75% of the questions correctly, it would be considered as the effectiveness of the training and otherwise the training would continue. In order to provide more guidance and support in the intervals between sessions and during the 8-week follow-up period, the researcher answered the possible ambiguities of the intervention group by phone for about 10 minutes and in accordance with the needs of the patient and his caregiver.
Content of training sessions for patients and caregivers. The content of the sessions conducted by the researcher for patients and caregivers of the intervention group included the following: (i) First session: In this session, they were taught about asthma, disease triggers and allergens, familiarity with common medications and their side effects, and ways to prevent infections and asthma attacks; (ii) Second session: in the session, the were taught about proper breathing techniques and effective coughing, motivational dialogue to quit smoking and prevent smoking, diet and complementary nutrition, an exercise in asthma, and how to properly deal with acute conditions; and (iii) Third session: In this session, the use of asthma and nebulizer, familiarity with the peak flow meter device and how to use it were taught. Also, patients were evaluated for the correct performance of the taught techniques and the contents of previous sessions.
Statistical analysis. Data were evaluated using SPSS v.19 software and the final analysis was performed on 58 patients and caregivers. Mean and standard deviation were used to describe the data. Furthermore, the frequency and percentage were used to describe the qualitative data. To comparison between the two groups, in case of parametric assumptions, the T-test of two independent samples was used and in case of no assumptions, Mann-Whitney test was used. Dependent t-pair test was used to evaluate the intra-group comparison and Wilcoxon nonparametric test was used if the hypotheses were not met. Repeated analysis test was used to compare more than two groups if parametric assumptions were made and Friedman test was used if no assumptions were made. The relationship between qualitative variables was also assessed by Chi-square test (Significance level was considered 0.05 for all tests).
Results
Table 1 shows that the only variables studied in which statistically significant differences were found were sex and other diseases, which had higher proportions in the intervention group than in the control group.
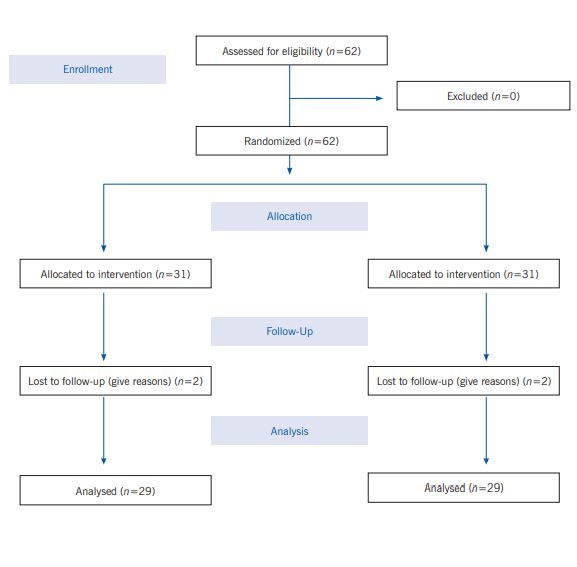
Table. 1 Frequency distribution of demographic variables of the studied units in the control and intervention groups
| Groups | Groups | Intervention | Intervention | Control | Control | p-value |
|---|---|---|---|---|---|---|
| Variable | Variable | Number | Percentage | Number | Percentage | p-value |
| Age | 18-30 | 1 | 3.4 | 0 | 0.0 | 0.132 |
| Age | 31-40 | 7 | 24.1 | 7 | 24.1 | 0.132 |
| Age | 41-50 | 5 | 17.2 | 11 | 37.9 | 0.132 |
| Age | 51-60 | 14 | 48.3 | 11 | 37.9 | 0.132 |
| Sex | Male | 3 | 10.3 | 13 | 44.8 | 0.003 |
| Sex | Female | 26 | 89.7 | 16 | 55.2 | 0.003 |
| Level of education | Illiteratee | 5 | 17.2 | 1 | 3.4 | 0.060 |
| Level of education | Primary | 6 | 20.7 | 10 | 34.5 | 0.060 |
| Level of education | Lower than diploma | 3 | 10.3 | 9 | 31.0 | 0.060 |
| Level of education | Diploma | 9 | 31.0 | 6 | 20.7 | 0.060 |
| Level of education | Bachelor | 6 | 20.7 | 2 | 6.9 | 0.060 |
| Level of education | Upper than bachelor | 0 | 0.0 | 1 | 3.4 | 0.060 |
| Marital status | Single | 3 | 10.3 | 1 | 3.4 | 0.106 |
| Marital status | Married | 20 | 69.0 | 27 | 93.1 | 0.106 |
| Marital status | Divorced | 3 | 10.3 | 0 | 0.0 | 0.106 |
| Marital status | The wife died | 3 | 10.3 | 1 | 3.4 | 0.106 |
| Employment status | Employee | 1 | 3.4 | 3 | 10.3 | 0.140 |
| Employment status | Farmer | 0 | 0.0 | 1 | 3.4 | 0.140 |
| Employment status | Free | 1 | 3.4 | 6 | 20.7 | 0.140 |
| Employment status | housewife | 20 | 69.0 | 11 | 37.9 | 0.140 |
| Employment status | Unemployed | 1 | 3.4 | 1 | 3.4 | 0.140 |
| Employment status | Worker | 1 | 3.4 | 2 | 6.9 | 0.140 |
| Employment status | Retired | 5 | 17.2 | 5 | 17.2 | 0.140 |
| Income level | Less than 30 dollar | 8 | 27.6 | 9 | 31.0 | 0.892 |
| Income level | Between 30-60 dollar | 14 | 48.3 | 12 | 41.4 | 0.892 |
| Income level | More than 60 dollar | 7 | 24.1 | 8 | 27.6 | 0.892 |
| Having health insurance | Yes | 28 | 96.6 | 28 | 96.6 | 0.754 |
| Having health insurance | No | 1 | 3.4 | 1 | 3.4 | 0.754 |
| Habitat | City | 28 | 96.6 | 27 | 93.1 | 0.079 |
| Habitat | Village | 8 | 27.6 | 2 | 6.9 | 0.079 |
| Another diseases | Yes | 18 | 62.1 | 9 | 31.0 | 0.034 |
| Another diseases | No | 11 | 37.9 | 20 | 69.0 | 0.034 |
Comparison of the mean score of asthma control test in control and intervention groups
Based on the results of repeated measures test, the mean score of asthma control test was different. The trend of changes in the mean score of asthma control test in the intervention group (before intervention =14.37±4.24, 4 weeks after intervention = 17.34±4.02, 8 weeks after intervention =20.03±3.51) more than the control group (before intervention = 14.86±3.80, 4 weeks after the intervention = 13.41±3.69, 8 weeks after the intervention = 13.03±3.64 which indicates the effect of the intervention on this group (p = 0.001), the asthma control score was statistically significant between the intervention and control groups (p <0.05); but the time and time/group variables showed no significant effect on asthma control score. In other words, time had no effect on asthma control test.
Comparison of mean scores of Spirometry indices in intervention and control groups
According to Table 2, in comparing the mean scores of Spirometry indices between the intervention and control groups before, 4 weeks after and 8 weeks after the intervention, it was found that 8 weeks after the intervention in the mandatory vital capacity index, there was a statistical difference between the control and intervention There was significance (p = 0.028). Regarding Spirometry FEV1 index, 8 weeks after the, there was a statistically significant difference between the control group and the intervention (p = 0.022). Regarding Spirometry FEV1/FVC index, 8 weeks after the intervention, there was a statistically significant difference between the control and intervention groups (p = 0.019). According the Spirometry FEF 25-75% index in 8 weeks after intervention, there was a statistically significant difference between control and intervention (p =0.023).
Table. 2 Comparison of mean scores of Spirometry indices by moment and groups
| Spirometry | Moment | Intervention | Intervention | Control | Control | p-value |
|---|---|---|---|---|---|---|
| Spirometry | Moment | Mean | SD | Mean | SD | p-value |
| FVC | Before intervention | 75.89 | 22.52 | 81.34 | 22.63 | 0.428 |
| FVC | 4 weeks after the intervention | 89.79 | 22.12 | 83.55 | 20.32 | 0.268 |
| FVC | 8 weeks after the intervention | 90.89 | 20.60 | 79.27 | 18.46 | 0.028 |
| FEV1 | Before intervention | 66.13 | 22.53 | 74.93 | 23.69 | 0.189 |
| FEV1 | 4 weeks after the intervention | 80.44 | 20.90 | 74.17 | 22.76 | 0.279 |
| FEV1 | 8 weeks after the intervention | 85.51 | 21.03 | 70.62 | 22.78 | 0.022 |
| FEV1/FVC | Before intervention | 72.68 | 12.71 | 75.68 | 12.31 | 0.319 |
| FEV1/FVC | 4 weeks after the intervention | 75.96 | 12.71 | 72.06 | 14.87 | 0.312 |
| FEV1/FVC | 8 weeks after the intervention | 80.37 | 13.99 | 72 | 12.59 | 0.019 |
| FEF 25-75% | Before intervention | 48.82 | 31.77 | 61.10 | 35.20 | 0.124 |
| FEF 25-75% | 4 weeks after the intervention | 57.75 | 29.92 | 58.3 | 32.30 | 0.973 |
| FEF 25-75% | 8 weeks after the intervention | 67.31 | 28.92 | 49.58 | 28.82 | 0.023 |
Frequency distribution of demographic variables of patients' primary caregiver
Using Chi-square and Fisher tests, it was shown that the two groups of control and intervention did not have a statistically significant difference with each other in terms of age and sex (p> 0.05). In addition, there was no statistically significant difference between the two groups of control and intervention in terms of variables of education level, marital status, patient relationship and chronic diseases (p> 0.05) (Table 3).
Table 3 Demographic variables of patients' primary caregiver
| Groups | Groups | Intervention | Intervention | Control | Control | p-value |
|---|---|---|---|---|---|---|
| Variable | Variable | Percentage | Number | Percentage | Number | p-value |
| Age | Less than 20 | 10.3 | 3 | 10.3 | 3 | 0.91 |
| Age | 20-30 | 13.8 | 4 | 13.8 | 4 | 0.91 |
| Age | 31-40 | 17.3 | 5 | 20.18 | 6 | 0.91 |
| Age | 41-50 | 13.8 | 4 | 20.18 | 6 | 0.91 |
| Age | 51-60 | 27.6 | 8 | 27.6 | 8 | 0.91 |
| Age | 61-70 | 13.8 | 4 | 3.4 | 1 | 0.91 |
| Age | More than 70 | 3.4 | 1 | 3.4 | 1 | 0.91 |
| Sex | Male | 48.3 | 14 | 48.3 | 14 | 0.793 |
| Sex | Female | 51.7 | 15 | 51.7 | 15 | 0.793 |
| Level of education | illiterate | 10.3 | 3 | 10.3 | 3 | 0.955 |
| Level of education | Lower than diploma | 44.8 | 13 | 48.3 | 14 | 0.955 |
| Level of education | Diploma | 27.6 | 8 | 31.1 | 9 | 0.955 |
| Level of education | College education | 17.3 | 5 | 10.3 | 3 | 0.955 |
| Marital status | Single | 17.2 | 5 | 13.8 | 4 | 0.219 |
| Marital status | Married | 69 | 20 | 86.2 | 25 | 0.219 |
| Marital status | Divorced | 6.9 | 2 | 0 | 0 | 0.219 |
| Marital status | The wife died | 6.9 | 2 | 0 | 0 | 0.219 |
| Relationship with the patient | Father | 10.3 | 3 | 3.4 | 1 | 0.260 |
| Relationship with the patient | Mother | 0 | 0 | 3.4 | 1 | 0.260 |
| Relationship with the patient | Wife | 51.7 | 15 | 72.5 | 21 | 0.260 |
| Relationship with the patient | Sister | 3.4 | 1 | 3.4 | 1 | 0.260 |
| Relationship with the patient | Brother | 0 | 0 | 0 | 0 | 0.260 |
| Relationship with the patient | Child | 34.6 | 10 | 17.3 | 5 | 0.260 |
| Chronic diseases | Yes | 24.1 | 7 | 31 | 9 | 0.770 |
| Chronic diseases | No | 75.9 | 22 | 69 | 20 | 0.770 |
Comparison of mean scores of care stress in control and intervention groups
Mann-Whitney test was used to compare pre-intervention care pressure in the two groups due to non-normality of data. According to the results, there was no statistically significant difference between the two groups in terms of mean score of care pressure (mean care pressure of the control group= 35.24±10.73 and the intervention group = 35.51±11.31; p = 0.75). To compare the care pressure 8 weeks after the intervention in the two groups, due to the normal distribution of data, t-test was used and the results showed that there was a statistically significant difference between the two groups in terms of mean care pressure score (The mean care pressure of the control group = 35.72±9.63 and 18 ±6.61 in the intervention group (p<0.001). In other words, the Tech-back training method has reduced the care pressure in the caregivers of the intervention group.
Discussion
Today, no one doubts the need for disease prevention to take precedence over treatment, because any disease, in addition to the suffering it imposes, requires a high cost to cure it, which affects both the individual and the community, as a result, it can be helpful to teach disease-related content in a way that stays in the mind for a long time and promotes better interaction between the patient and the nurse. Although some diseases, such as asthma, are not curable, they can be controlled. In this study, we used the Teach-back education method for patients with asthma and measured its effect on patients' asthma control and family care pressure in patients with asthma.
Based on the results, in comparing the mean scores of asthma control test in the control and intervention groups, it was found that the mean scores of asthma control test in the control group, before, 4 weeks after and 8 weeks after the intervention were 14.86, 13.41, and 13.03 respectively. Accordingly, the results of the control group showed that their disease was not under control in all 3 time periods. On the contrary, our training method on the intervention group led to disease control in patients in this group. After 8 weeks, the patients in the intervention group went from uncontrolled asthma to controlled asthma. Due to the significance of the group variable, there was a statistically significant difference between the intervention and control in terms of asthma control. In addition, the time and time / group variables showed no significant effect on asthma control score. These findings indicate the effectiveness of Teach-back education in controlling asthma.
Furthermore, in comparing the mean scores of Spirometry indices, it was found that the mean scores of all Spirometry indices in the intervention group were statistically significant and not the same. Also, the trend of changes in the mean of these scores showed that this educational method has a positive effect on patients and their Spirometry index has increased.
Shermans et al.14 conducted a randomized controlled clinical trial with the aim of the effect of a 10-minute training session on patients' asthma control. In the intervention group, a 10-minute training including basic information about asthma and the effectiveness of medications was given. This training was not provided to the control group. The training session caused that after 3 months, asthma was significantly controlled in the intervention group compared to the control group. However, in the study of Arikan-Yildiz et al.15 the scores of asthma control test were not significantly different in comparison before and after the intervention; which did not agree with the results of the study. The reasons for this difference in results include differences in the number of training program sessions (one hour training session), the age range of study participants (5-18 years), the manner of holding training sessions or the educational content presented in the sessions
In comparing the mean scores of caregiving stress in the two groups of control and intervention before and after the intervention, it was found that there was no statistically significant difference between the two groups in terms of mean scores of caregiving pressure before the intervention; But 8 weeks after the intervention, there was a statistically significant difference between the two groups in terms of mean care pressure score. Ghaneh et al.16) conducted a study to determine the effect of supportive education program on the care pressure of family caregivers of patients undergoing hemodialysis. The results showed that the care pressure in the experimental group decreased after the intervention. According to the results of this study, it can be said that the use of educational-supportive programs can be effective in reducing the care pressure of family caregivers.
In conclusion, the results of the present study showed that teaching asthma related topics to the patient and her caregiver along with the follow-up and supervision of the nurse improves asthma control and also reduces the caregiver pressure. Additionally, this study also shows that the use of educational methods by asthmatics in a way that stays in the mind for a long time leads to an improvement in their condition. Nursing managers should inform staff about the importance and learning of these training methods by holding training courses. It is also suggested that more educational-therapeutic methods be used to cure diseases.

