










Services on Demand
Journal
Article
 English (pdf)
English (pdf)
 Article in xml format
Article in xml format Article references
Article references
 Send this article by e-mail
Send this article by e-mailIndicators
-
 Cited by SciELO
Cited by SciELO -
 Access statistics
Access statistics
Related links
-
 Cited by Google
Cited by Google -
 Similars in
SciELO
Similars in
SciELO -
 Similars in Google
Similars in Google
Share

 Permalink
PermalinkRevista Salud Uninorte
Print version ISSN 0120-5552
Salud, Barranquilla vol.28 no.1 Barranquilla Jan./June 2012
CASO CLÍNICO/ CLINIC CASE
Moebius-Poland syndrome: A case report
Síndrome Moebius-Poland: Reporte de un caso
Mostapha Ahmad1 , 2, Carlos Silvera Redondo1, Muna Hamdan Rodríguez2
1 Grupo de Investigación: Genética y Medicina Molecular, Universidad del Norte. Barranquilla (Colombia). csilvera@uninorte.edu.co
2 Grupo de Investigación en Enfermería, Fundación Centro Médico del Norte. Barranquilla (Colombia).
Correspondencia: Carlos Silvera Redondo. Universidad del Norte, km 5, vía a Puerto Colombia. Barranquilla (Colombia). A.A. 1569. Tel. 57-53509509. csilvera@uninorte.edu.co
Fecha de recepción: 14 de febrero de 2012
Fecha de aceptación: 15 de mayo de 2012
Abstract
The Moebius syndrome is an infrequent symptomology in which the sixth and seventh cranial nerves are involved. Such involvement is translated in facial paralysis. There have been described around 500 cases in the world medical literature and some of them have received surgical treatment. Moebius syndrome has also received other names such as congenital nuclear aplasia, childlike nuclear aplasia, Oculofacial congenital paralysis and facial diplegia. Poland syndrome is another rare congenital abnormality of the chest wall, characterized by unilateral partial or total absence of the great pectoral muscle and ipsilateral symbrachydactyly. However, the Moebius-Poland syndrome is rarer. Its first case was recently reported in 2007 by Diego López de Lara et al. In this article we will report this infrequent case; the combination between both syndromes Moebuis and Poland in a three –month- old male patient.
Keywords: Moebius syndrome, Poland syndrome, facial paralysis hypoplasia, symbrachydactyly.
Resumen
El síndrome de Moebius es una sintomatología poco frecuente en la que los pares craneales sexto y séptimo están involucrados. Esta implicación resulta en parálisis facial. Se han descrito unos 500 casos en la literatura médica mundial y algunos de ellos han recibido tratamiento quirúrgico. Además el síndrome ha recibido otros nombres, tales como aplasia congénita nuclear, aplasia nuclear infantil, parálisis congénita oculofacial y diplejía facial. El síndrome de Poland es otra anomalía congénita muy poco frecuente de la pared torácica, caracterizado por ausencia unilateral parcial o total del músculo pectoral mayor y braquisindactilia ipsilateral. Sin embargo, el síndrome de Moebius-Poland es más raro, ya que el primer caso fue reportado recientemente en el año 2007 por Diego López de Lara et al. En este artículo se presentará este caso poco frecuente, que es una combinación entre ambos síndromes Moebius y Poland en un paciente masculino de tres meses de edad.
Palabras clave: Síndrome de Moebius, síndrome de Poland, parálisis facial, hipoplasia, simbraquidactilia.
INTRODUCCIÓN
Moebius syndrome
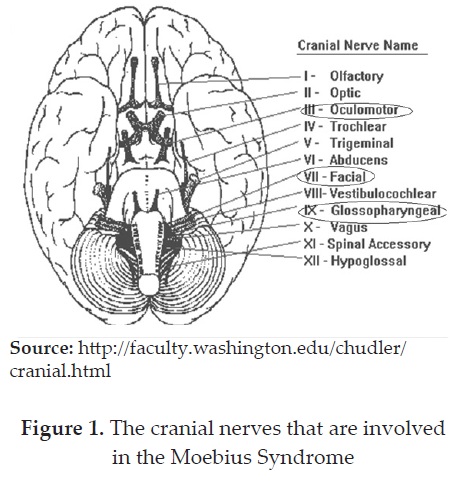
Unilateral or bilateral loss of ocular abduction, unilateral o bilateral complete or incomplete facial weakness, primary or secondary congenital anomalies of the extremities and possible other involvement of the branchial musculature are the principal clinical features of the Moebius syndrome (1), which was first described by Albrecht Von Gaefe and Saemisch in 1880. Other reports about the syndrome were those by Harlan in 1881, Chisholm in 1882, Schapringer 1889. However the Affirm was associated to a group of constant symptoms described by Moebius in 1888 and goes under his name after he realized a study in 43 cases of congenital and acquired facial paralysis (2). Figure (1).
Poland syndrome
Poland syndrome is a rare congenital abnormality of the chest wall, which was described for the first time by Alfred Poland in 1841(3), characterized by unilateral partial or total absence of the major pectoral muscle and ipsilateral symbrachydactyly. It also causes breast hypoplasia with an incidence of 1:3000 up to1:10000 in children (4). Figure (2).
In this case scenario we will report an infrequent case, which is a combination between both syndromes (Moebius and Poland) in a three – month- old male patient.
Case Scenario
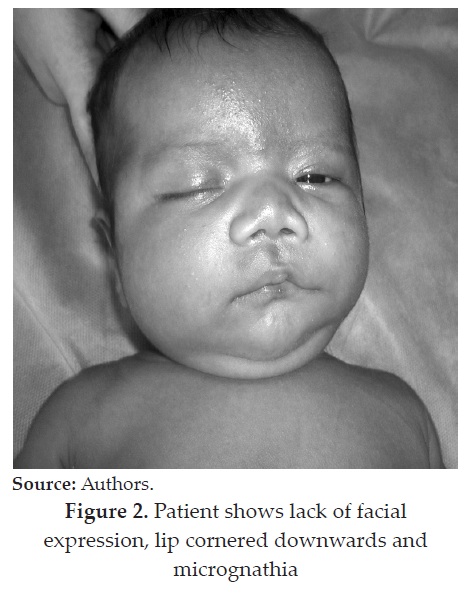
The case reported, shows a male patient of three- month - old, who proceeds from the second pregnancy of a healthy couple without consanguinity antecedents or inbreeding, normal pregnancy course, without (denies) exposure to teratogens, normal delivery, normal psychomotor development for his present age and with normal karyotype (46 XY). He was remitted to genetic consultation due to lack of his facial mimicry and abnormal morphology in his right hand.
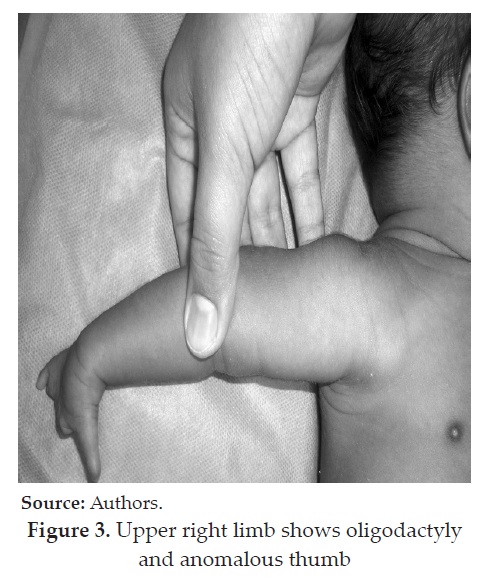
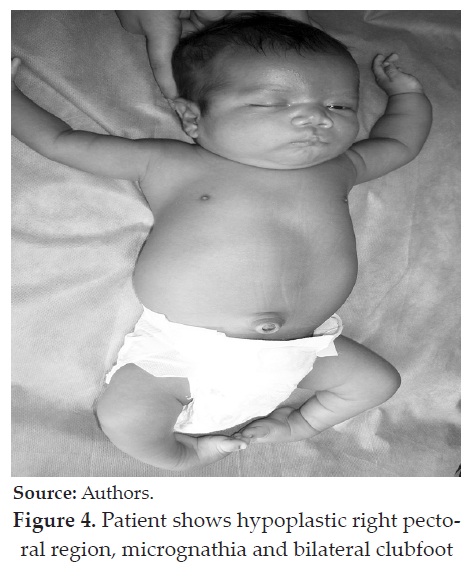
Physical examination shows brachycephaly, left facial paralysis, ptosis, lack of facial expression, strabismus and elongated ears rotated backwards. In addition, lip cornered downwards and micrognathia. Thoracic examination resulted in hypoplastic right pectoral region and inability to palpate the right pectoral muscle. Inferior limbs present bilateral clubfoot. Oligodactyly of the index, middle, ring and little finger of the right hand and anomalous thumb, due the hypoplasia of phalanx and nail, are presented. Chest X-ray study shows lack of soft tissue development in the right pectoral region. During the patient management, he was diagnosed with two pathologically related anomalies such as, Poland anomaly and Moebius syndrome; thus the natural history of the disease was oriented, family genetic counseling was offered. Figure (2, 3 y 4).
DISCUSSION
The Moebius syndrome (OMIM 157900) is an infrequent symptomology in which the sixth and seventh cranial nerves are involved, this results in facial paralysis (5). There have been described around 500 cases in the world medical literature; some of them have received surgical treatment. Mobeius syndrome has also received other names such as congenital nuclear aplasia, childlike nuclear aplasia, oculofacial congenital paralysis and facial diplegia (6). It is most commonly sporadic and of an unknown cause (7). The syndrome´s etiology is controversial. Different theories associate the syndrome to the alteration in the mesodermic and ectodermic level during the embryonic development (6). Other studies demonstrated that it has a genetic origin (locus 13q12.2), associated to autosomic dominant inheritance, autosomic recessive and including cases with recessive inheritance linked to the X chromosome (8, 9, 10, and 11). On other hand it can derive from isquemic vascular origin, which is associated to a polygenic factor or to an interaction with teratogenic agents, such as Misoprostol (12, 13, and 14). Moebius syndrome can also be associated with diseases and disorders, such as hypogonadotropic hypogonadism, Poland syndrome (15), cataplexy (16), bilateral vocal cord paralysis (17), total anomalous pulmonary venous connection (18), narcolepsy and parasomnias (19).
The syndrome is usually diagnosed during the first few days of life, because of the incomplete closure of the eyelids during sleep and the difficulty in lactation. The masklike facial expression is also noticed while the infant is crying or laughing, associated with dribbling saliva, depending on the degree of involvement of the facial musculature (1). The differential diagnosis should be reached after inspecting for and excluding diseases that produce facial paralysis, such as, neonatal traumatism (forceps), pseudo bulbar paralysis, myotonic dystrophy, skull base fractures, infectious illnesses (otitis, herpes zoster, mastoiditis, mononucleosis), tumors, Hodgkin disease, Guillain-Smeared syndrome, etc. The treatment is fundamentally surgical. However, there are necessary measures to be adopted at the moment of birth in order to prevent further complications caused by the syndrome, such as using artificial tears, diet instructions, nocturnal ocular seal, etc. As mentioned before, surgery constitutes the fundamental support in the treatment of Moebius syndrome. This requires the use of multiple reconstructive surgery resources, which will focus on the following aspects: Management of the epicanthic fold, correction of the palpebral closure, correction of the facial ptosis (2), correction and elongation of the upper lip and dynamic suspension of the mouth.
Poland syndrome (OMIM 173800) is a rare congenital abnormality of the chest wall. It was described for the first time by Alfred Poland in 1841 (3). The incidence of this syndrome has been estimated to be 1:32000 with higher frequency among males (ratio 2: 1 and 3: 1) and affects the right side of the body twice as often as the left (20). It was also reported in 20 patients with deletion of a dominant autosomic gene (21, 22). The most common clinical features of the syndrome are: hypoplasia of hemithorax or ribs, latissimus dorsi, anterior serratus, external oblique, intercostal muscles, infra and supraspinatus and deltoid muscle, Hypoplasia or absence of the nipple and breast (absent sternocostal head of the major pectoral and absence of the minor pectoral), bony dysostosis affecting the hand (brachymesophalangy with syndactyly, biphalangy, ectrodactyly), wrist, forearm, upper arm, scapula, axillary webs and absence of axillary hair, minimal subcutaneous fat, lung herniation and scoliosis (23,24,25,26).
Despite the unclear pathogenicity of this syndrome, it is mostly believed that in the embryonic development, during the sixth week of pregnancy, a momentary stoppage or reduction in the circulation of the thoracic artery or one of its peripheral ramifications primes the pathogenic mechanism of the syndrome and results in different degrees of syndrome severity, depending on the length and intensity of the vascular interruption (27, 28). Many associations were described between this syndrome and a variety of diseases or other syndromes, such as Adams-Oliver syndrome which is characterized by defects of the limbs, scalp, and skull (29), Goldenhar syndrome which is facio-auriculo-vertebral syndrome (30), Wilms tumor (31), breast carcinoma (32), lung cancer (33), neuroblastoma (34), lymphoma (35), arterial septal defects, were found in some patients in an early or late stages (36) and eye abnormalities (37).
Moebius syndrome is characterized by neurological malformations of the basal ganglia (38). Malignancies like acute leukemia, non-Hodgkin lymphoma, lung cancer (39) and breast cancer (40) were also reported. Hypogonadotropic Hypogonadism, where the first case was reported about a male who was born at 39 weeks of gestation(15) and renal anomalies have been reported infrequently (41,42). An example of the latter is a reported case of an infant with a Poland syndrome, who also had ipsilateral aplasia of his kidney (43). It was also demonstrated that the delayed carpal bone maturation, disharmonious ossification and carpal coalition, particularly of the scaphoid and trapezium bones, are characteristics of Poland syndrome (22, 44).
Poland syndrome can be diagnosed at a primary instant by the clinical features as mentioned before. Still, in order to confirm the affected morphology and functionality of the major pectoral muscles, we must apply further examinations such as electromyography, ecography and computed tomography (26, 21). This syndrome is treated using mainly reconstructive surgery. Fused fingers are separated as early as possible and breast or chest implants may be used after full physical development has been reached. Today, bioengineered cartilage can be implanted to help and give the chest a more normal appearance (Surgical Reconstructions in 18 cases) (45).
CONCLUSION
Moebius syndrome etiology has been related with alteration in the mesoderm and ectoderm levels during embryonic development. However, other studies have proposed a genetic origin (locus 13q12.2), associated to autosomic dominant or recessive inheritance, including cases with recessive inheritance linked to the X chromosome.
Nowadays, a vascular origin associated to teratogenic agents, such as Misoprostol derivatives drugs have increased the Moebius clinical frequency. Although, there is a commonly well-accepted vascular theory associated to Moebius, Poland and Klippel- Feil syndromes. In this case study, neither family history nor teratogen exposure was found. This case was classified as a sporadic vascular originated defects and family counseling was offered.
Conflicts of interests: None.
Funding: Universidad del Norte.
REFERENCES
(1) Robert N. Richards. The Moebius Syndrome. J Bone Joint Surg Am 2010; 35:437-444. [ Links ]
(2) Villafranca A J, Castillo D P, Garcés SM, Villalón FE, Grez lE, Díaz GA, Síndrome de Moebius, Rev. Chilena de Cirugía 2003; 55 (1): 75-80. [ Links ]
(3) Ferraro GA, Perrotta A, Rossano F, D'Andrea F, Napoli, Italy. Poland Syndrome: Description of an Atypical Variant. Aesth. Plast. Surg 2205; 29:32–33. [ Links ]
(4) Mentzel HJ, Seidel J, Sauner D, Vogt S, Fitzek C, Zintl F, Werner A.Ka iser, Radiological aspects of the Poland syndrome and implications for treatment: a case study and review. Eur J Pediatr 2002; 161: 455–459. [ Links ]
(5) Möbius PJ. Über angeborene doppelseitige Abducens- Facialis Lahmung. Munch Med Wochenschr; 35:91-94. [ Links ]
(6) Coiffman F, Cantini J. Síndrome de Moebius. En: Coifman F, editor. Cirugía Plástica Reconstructiva y Estética. Barcelona: Masson-Salvat; 1994. p. 1321-1325. [ Links ]
(7) Kumar D. Moebius syndrome. J Med Genet 1990; 27:122-126 [ Links ]
(8) OMIM (Online Mendelian Inheritance in Man). Catálogo de V.A. McKusic Baltimore University. [ Links ]
(9) López E, Pérez J, Marín C, Camino R, Ibarra I, Velasco M. Síndrome de Möbius y episodio aparentemente letal. Anales de Pediatría 2005; 62(4):373. [ Links ]
(10) Verzijl H, Van den Helm B, Veldman B, Hamel B, Kuyt L, Padberg G et al. A Second Gene for Autosomal Dominant Möbius Syndrome Is Localized to Chromosome 10q, in a Dutch Family. Am J Hum Genet 1999; 65:752-6. [ Links ]
(11) Lipson AH, Wabster WS, Brown-Woodman PDC, Osborn RA. Moebius syndrome: animal mode-human correlations and evidence for a brainstem vascular etiology. Teratology 1989; 40: 339-350 [ Links ]
(12) Marti M. Cabrera JC. Toledo L, Perez V, Bonnet D. Moebius syndrome. Three different forms of presentation. Rev Neurol 1998; 27(160):975-8. [ Links ]
(13) Fontenelle L, Prufer A, Fontana R. Síndrome de Moebius. Arq Neuro-Psiquiatr 2001; 59(3B). [ Links ]
(14) Fernández C, Hernández E, Silvera C, Jiménez B, Quintero E, Idrovo A, Manneh R. Síndrome de Moebius: Genopatía vs efecto teratogénico. Salud Uninorte 2006; 22(2): 182-187. [ Links ]
(15) López D, Cruz J, Sánchez J, Gallego M, Lledó G. Moebius-Poland syndrome and hypogonadotropic hypogonadism. Eurr J Pediatr 2008; 167(3): 353-354. [ Links ]
(16) Harrington H. Cataplexy in association with Moebius syndrome. J Neurol 2003; 250:110-111. [ Links ]
(17) Kanemoto N, Kanemoto K, Kamoda T, Hasegawa M, Arinami T. A case of Moebius syndrome presenting with congenital bilateral vocal cord paralysiss. Eur J Pediatr 2007; 166:831-833. [ Links ]
(18) Suvarna J, Bagnawar M, Deshmukk C. Moebius syndrome with total anomalous pulmonary venous connection. Indian J pediatr 2006; 73(5):427-429. [ Links ]
(19) Mayer G, Blanke G, Moebius Syndrome, Narcolepsy and Parasomnias: Report on Two Patients. Somnologie 2004; 8:110-114. [ Links ]
(20) Wang X, Ning L. Breast Carcinoma Associated with Poland's Syndrome: One Case Report and Literatures Review. Clin Oncol Cancer Res 2008; 5:223-225. [ Links ]
(21) Fokin A, Robicsek F. Poland_s syndrome revisited. Ann Thorac Surg 2002; 74:2218-2225. [ Links ]
(22) Urschel HC. Poland_s syndrome. Chest Surg Clin North Am 2000;10:393-403. [ Links ]
(23) Bouvet J, Leveque D, Bernetieres F, Gros J. 1978 Vascular origin of Poland syndrome? Eur J Pediatr 128: 17-26. [ Links ]
(24) Skandalakis J, Gray S. Embryology for surgeons. 2nd edn. Williams and Wilkins, Baltimore; 1994. [ Links ]
(25) Taybi H, Lachman R. Radiology of syndromes, metabolic disorders, and skeletal dysplasias,. 4th ed. Mosby.St. Louis;1996. p. 388-389. [ Links ]
(26) Wright A, Milner R, Bainbridge L, Wilsdon J. MR and CT in the assessment of Poland syndrome. J Comput Assist Tomography 1992; 16: 442-447. [ Links ]
(27) Bouvet J, Leveque D, Bernetieres F, Gros J. Vascular origin of Poland syndrome. Eur J Pediatr 1978; 128:17-26. [ Links ]
(28) Keymolen K, De Smet L, Bracke P, Fryns J. The concurrence of ring constrictions in Adams-Oliver syndrome: additional evidence for vascular disruption as common pathogenetic mechanism. Genet Couns 1999; 10: 295-300. [ Links ]
(29) Cobben J, Robinson P, van Essen A, van der Wiel H, ten Kate L. Poland anomaly in mother and daughter. Am J Med Genet 1989; 33: 519-521. [ Links ]
(30) Athale UH, Warrier R. Poland's syndrome and Wilms' tumor: an unusual association. Med Pediatr Oncol 1998; 30:67-68. [ Links ]
(31) Katz S, Hazem A, Colen S, Roses D. Poland's syndrome and carcinoma of breast: a case report. Breast 2002; 7:56-59. [ Links ]
(32) Ahn Mi, Park SH, Park YH Poland's syndrome with lung cancer. A case report. Acta Radiol 2000;41:432-434. [ Links ]
(33) Caksen H, Patriroglu T, Ozdemir M, Patiroglu T, Poyrazoglu M, Tercan M Neuroblastoma and Poland's síndrome in a 15 year-old boy. Acta Pediatr Jpn 1997; 39:701-704. [ Links ]
(34) Hershatter B, Montana G. Poland's syndrome and lymphoma. Am J Dis Child 1983; 137:1211-1212. [ Links ]
(35) Samant A, Sridhars S, Desser K, Benchimol A. Association of arterial septal defect with Poland's syndrome. Am Heart J 1993; 106:159-161. [ Links ]
(36) Gomez-Ulla F, Gonzalez F. Retinal vascular abnormality in Poland's syndrome. Br J Ophthalmol 1999; 83: 1092. [ Links ]
(37) Larrandaburu M, Schuler L, Ehlers JA, Reis AM, Silveira EL. The occurrence of Poland and Poland-Moebius syndromes in the same family: further evidence of their genetic component. Clin Dysmorphol 1999; 8: 93-99. [ Links ]
(38) Ahn MI, Park SH, Park YH Poland's syndrome with lung cancer: a case report. Acta Radiol 2000; 41: 432-434. [ Links ]
(39) Katz S, Hazen A, Colen S, Roses D. Poland's syndrome and carcinoma of the breast: a case report. Breast J 2001; 7:56-59. [ Links ]
(40) Mace J, Kaplan J, Schanberger J, Gotlin R. Poland's syndrome. Clin Pediatr 1972; 11:98- 102. [ Links ]
(41) Bouwes Bavinck J, Weaver D. Subclavian artery supply disruption sequence: hypothesis of a vascular etiology for Poland, Klippel- Feil, and Moebius anomalies. Am J Med Genet 1986; 23:903-918. [ Links ]
(42) Assadi FK, Salem M, Poland syndrome associated with renal agenesis. Pediatr Nephrol 2002; 17:269-271. [ Links ]
(43) Urschel H. Poland syndrome. Chest Surg Clin North Am 2000;10:393-403 [ Links ]
(44) Friedman T, Reed M, Elliott A. The carpal bones in Poland syndrome. Skeletal Radiol 2009; 38:585-591. [ Links ]
(45) Renato da Silva Freitas, Andre´ Ricardo Dall_Oglio Tolazzi, Vanessa Dello Monaco Martins, Breno Albuquerque Knop, Ruth Maria Graf, and Gilvani Azor de Oliveira e Cruz. Poland_s Syndrome: Different Clinical Presentations and Surgical Reconstructionsin 18 Cases. Aesth Plast Surg 2007; 31:140-146. [ Links ]
